Several epidemiological surveys
(1 –
5) have shown an increased prevalence of the nonmedical use of pharmaceutical opioid products, including codeine (tablets, cough syrups), hydrocodone, and oxycodone. The media has focused special attention on a sustained-release oxycodone preparation, OxyContin, which is typically prescribed for chronic pain in doses ranging from 10 to 80 mg. If used as prescribed, the opioid in OxyContin is slowly released over 12 hours, providing safe and effective pain relief
(6,
7) . However, in the latter part of the 1990s, it became widely known that crushing OxyContin tablets would free oxycodone from the sustained-release matrix and inhaling or dissolving and injecting the resulting powder would result in a pronounced “high.”
There have been several scientific studies that have examined national tendencies in the use (medical and nonmedical) and abuse of OxyContin and other pharmaceutical opiates
(2,
3), particularly among those prescribed for pain management in specialty clinics
(3,
7,
8) . These studies have also evaluated the role of prescription opioids in drug-induced deaths
(9 –
12) . The findings from these studies suggest that the role of OxyContin alone is minimal in the use and abuse of pharmaceutical opiates and the problems identified are not specific to OxyContin
(8,
10) .
A very different characterization of the increase in pharmaceutical opioid use is found in popular media reports. These reports are often inflammatory and accusatory in nature
(13,
14) . They frequently focus on OxyContin, referring to its increased use as “a plague”
(15) or “nuclear bomb”
(15,
16) . Moreover, many of these media reports describe people who receive OxyContin as “drug naive” individuals who began using the medication after receiving a prescription for legitimate medical reasons, followed quickly by escalating use, addiction, and sometimes overdose and death
(2,
16 –
25) .
While the extant scientific literature has characterized the general population of OxyContin “users” as well as those who have been receiving prescriptions for the medication in the course of pain treatment, there have been few large-scale studies of those whose use of this medication has led to a diagnosis of abuse or dependence and who have sought treatment for the disorder
(26,
27) . This subgroup of treatment-seekers is of particular interest, since their severe use and associated problems may be the most visible and socially problematic. However, they may also represent an entirely different group of users than those described in the media or prior reports.
As part of a separate study, our group of researchers recorded admission drug use reports from all patients entering a large, diverse sample of addiction treatment programs in the United States. These reports were collected using a standardized, validated, and computerized data collection protocol
(28 –
31) .
A series of OxyContin-focused questions were added to the Drug Evaluation Network System protocol and administered to 27,816 individuals admitted to the 157 addiction treatment programs participating in this network system from 2001 through 2004. Descriptive characteristics were provided for patients who reported any OxyContin use (regardless of other drug use) as well as for patients who reported no OxyContin use and for those who reported other opioid use (i.e., heroin, oxycodone, hydrocodone, or hydromorphone) but no OxyContin use. In the present study, we examined the overall prevalence of OxyContin use and employed multivariate analyses to characterize those individuals who abused OxyContin within the broader population of entrants to addiction treatment programs as well as within a subsample of users of other opioids (heroin and prescription). Finally, we examined changes in the prevalence of OxyContin use among persons entering treatment over time as well as changes in health and social variables.
Method
The Drug Evaluation Network System
The Drug Evaluation Network System
(28 –
31) is a sentinel system designed to track changes in substance use patterns and substance abuse-related health and social problems among entrants to addiction treatment programs across the United States. Individuals who are admitted to addiction treatment programs represent at best only 10% of all those who meet diagnostic criteria for substance use disorder
(32), and those individuals are generally the most severely affected.
Data Collection Procedures
The data collected derived from a computer-assisted Addiction Severity Index
(33 –
35) assessment interview performed by counselors as part of the standard admission procedure for each program. All counselors in each program were trained in the criterion of administration of the Addiction Severity Index
(36) . The interview included eight additional questions pertaining to OxyContin and 12 additional questions pertaining to the use of other pharmaceutical opioids. Beyond the initial training, there were 150 consistency checks built into the software program to assure internal consistency as well as range checks on all items. Collected admission data were automatically removed from individual patient identifiers and transferred to a central database each week via a computer modem
(28) . All patients admitted to these programs were interviewed; therefore, these findings represent essentially 100% of the samples at all programs throughout the time period.
Additional Questions
The following eight questions were asked:
1. How many days in the past 30 have you used OxyContin?
2. How many years in your life have you used OxyContin at least three times weekly?
3. By what route of administration did you use OxyContin (oral, nasal, smoking, injection)?
These questions were also asked about hydrocodone, oxycodone, and hydromorphone.
The following questions were only asked of patients who reported using OxyContin at least once:
1. Was the OxyContin prescribed for you for diagnosed pain or medical reasons?
2. Did you use the OxyContin to “get high or get a buzz”?
3. Did you take the OxyContin in combination with other opioids, heroin, or methadone?
4. How many months ago did you first use OxyContin?
5. Did you get the OxyContin from a friend, family member, or on the street?
The Drug Evaluation Network System Program Sample
A total of 157 treatment programs participated in the Drug Evaluation Network System during the time period when the OxyContin questions were added (2001–2004). These programs were located in 22 states and 105 different cities. Fifty-seven percent (N=89) of the sites were located in major urban areas, whereas 43% (N=68) were located in nonurban areas. Most of the sites (61%) were outpatient programs, 22% were inpatient/residential programs, 11% were methadone treatment programs, and 6% were mixed-modality programs.
When this set of programs was originally selected in late 2001, it was a random, nationally representative sample from the federal registry
(37), representing all licensed, adult treatment programs (public and private) and all major rehabilitation modalities (residential, outpatient, methadone). However, there have been substantial and repeated reorganizations within the treatment system, including closure and merger rates of up to 20% per year
(38,
39) . Because of these changes, it is no longer reasonable to regard this program sample as nationally representative. Nonetheless, it consists of a large number of randomly selected adult addiction treatment programs and all patients entering those programs.
The Drug Evaluation Network System Patient Sample
The procedures described above resulted in 27,816 unique patients. Patients were predominantly male (64%), white (42%), or black (42%), and the mean age was 36 years (range: 18–87 years). Approximately 40% of patients reported that their entrance into treatment was prompted by the criminal justice system. In terms of their primary problem, alcohol alone was reported by 17% of patients, 11% indicated heroin/opioids, and 12% reported cocaine. However, the largest percentage (47%) of patients reported problems with multiple substances, including alcohol.
Analyses
All analyses were performed using SPSS 12.0 and SAS 9.1.
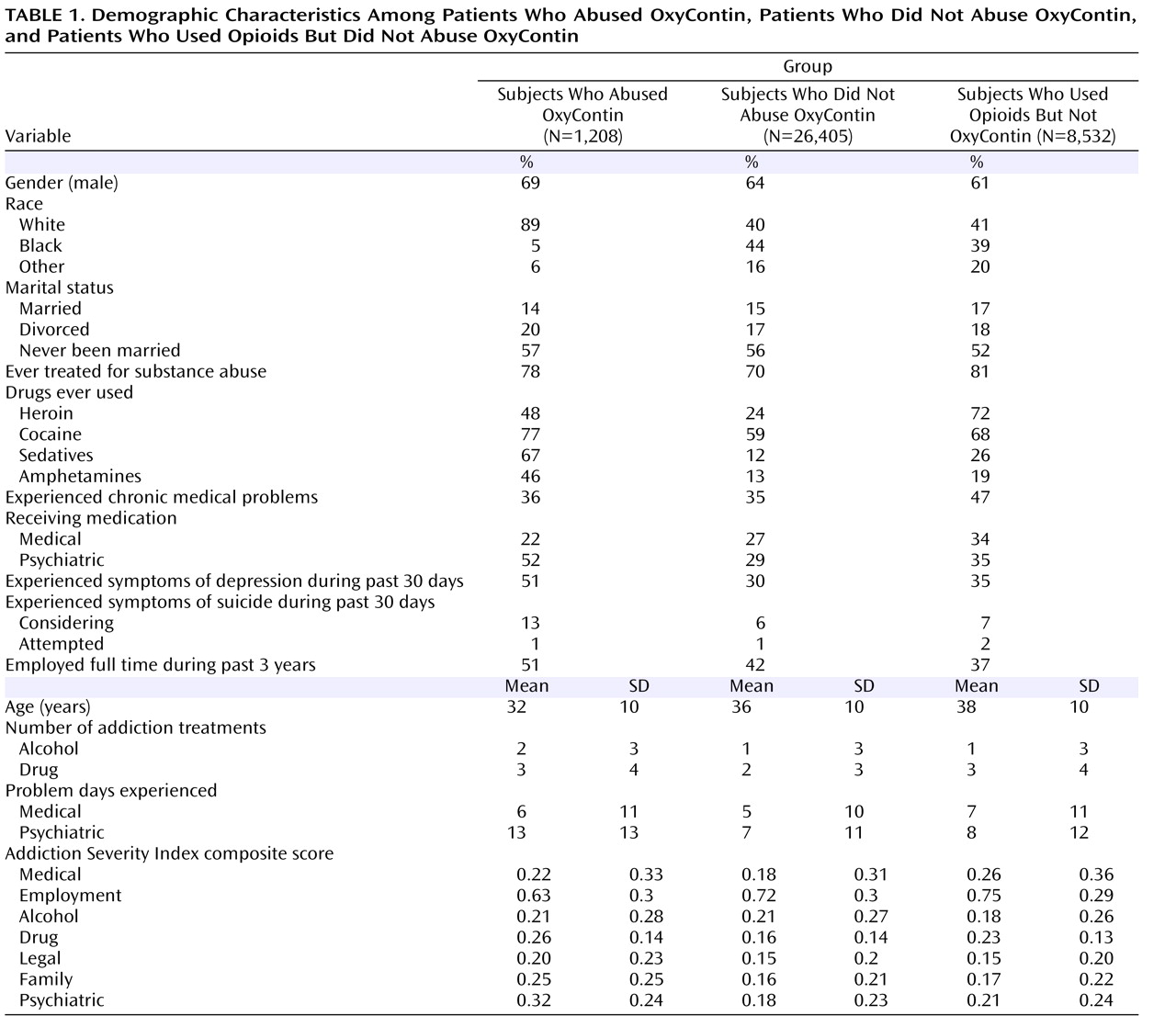
Table 1 shows the characteristics of patients who reported any OxyContin use, those who had not used OxyContin, and those who had used other opioids (i.e., heroin, oxycodone, hydrocodone, or hydromorphone) but not OxyContin. Additional analyses were performed on individuals who used OxyContin and reported using it to “get high or get a buzz.” We categorized these individuals as “abusers” of OxyContin. General Estimating Equation models were used to identify variables that differentiated individuals who abused OxyContin from the broader population of patients admitted into the programs and from those patients admitted who reported other opioid use.
A final set of General Estimating Equation analyses assessed changes over time in the prevalence of OxyContin abuse as well as changes in health and social variables of those reporting OxyContin use. In this regard, the sample of treatment programs in DENS changed over time (mostly because of closures, mergers, and replacements), and thus these analyses were calculated only on the 27 programs that collected and reported data across the final eight quarters (July 2002–June 2004). The General Estimating Equation models allowed for the nesting of patients within sites and of time points within sites for the change-over-time analyses and utilized an exchangeable working correlation structure.
Results
Overall Prevalence and Characteristics of OxyContin Use
Of the 27,816 clients presenting with substance problems at the 157 treatment programs during 2001–2004, approximately 5% (N=1,425) reported ever using OxyContin. Clinicians estimated the duration of regular use (>3 times/week) by rounding to the nearest year (³6 months=1 year). Among those patients, almost all (87% [N=1,243]) were classified as using OxyContin regularly (>3 times/week) for at least 1 year (range: 1–9 years; mean=2.3 years [SD=1.6]). The use of OxyContin within the past 30 days was reported by 2% (N=562) of the total sample, with an average frequency of 12 days (SD=11). In this section, we present data from the follow-up questions asked of the 1,425 patients who reported any use of OxyContin.
How many months ago did you first use OxyContin? Thirty-six percent (N=502) of the individuals categorized as “users” of OxyContin had been using the drug less than 1 year prior to their treatment admission. An additional 25% had been using the drug less than 2 years. The remaining 39% had been using the drug for more than 2 years.
Route of administration
Seventy-two percent (N=981) of individuals categorized as “users” of OxyContin reported the oral route of administration, 11% (N=153) reported inhaling crushed tablets, and 17% (N=234) reported injecting crushed tablets.
Was OxyContin used to “get high”? Eighty-six percent (N=1,208) of individuals who used OxyContin reported using it to “get high or get a buzz.”
Was OxyContin prescribed for diagnosed pain or medical reasons? Seventy-eight percent (N=1,095) reported that OxyContin had not been prescribed for any medical reason. One-third (N=100) of the 300 patients who did report receiving a prescription also reported receiving OxyContin through illicit means, and 56% (N=171) reported using the medication to “get high.”
Did OxyContin “users” receive prior substance abuse treatment? Nearly three-quarters (N=1,026) of individuals categorized as “users” of OxyContin had received substance abuse treatment prior to their admission. On average, these patients had received 3.8 prior treatments (SD=3.7 [range: 1–20 treatments]).
Was OxyContin used in combination with other opioids (includes heroin, methadone, hydromorphone, hydrocodone, and oxycodone)? Ninety-two percent (N=1,242) of individuals categorized as “users” of OxyContin reported using the medication with one or more other opioid. Eight percent (N=102) of patients categorized as “users” of OxyContin reported no other opioid use, but 66% (N=67) reported the use of cocaine, 69% (N=70) reported heavy alcohol use, and 75% (N=76) reported using pot.
Only eight of the 1,425 (0.5%) individuals categorized as “users” of OxyContin reported no use of any additional drugs other than alcohol. Four of these patients were older males who were admitted for alcohol problems only. They reported daily, chronic medical problems and received prescribed OxyContin for pain. The remaining four patients were also male but younger, with no chronic medical problems. They reported using only OxyContin and used the medication only to “get high.” They used OxyContin an average of 14 days prior to admission, spending an average of $1,737 on the drug during that period.
All of the preceding analyses reported were on all patients who reported any OxyContin use (N=1,425). The following analyses describe the 1,208 individuals who abused OxyContin: those who reported using the medication simply to “get high or get a buzz.”
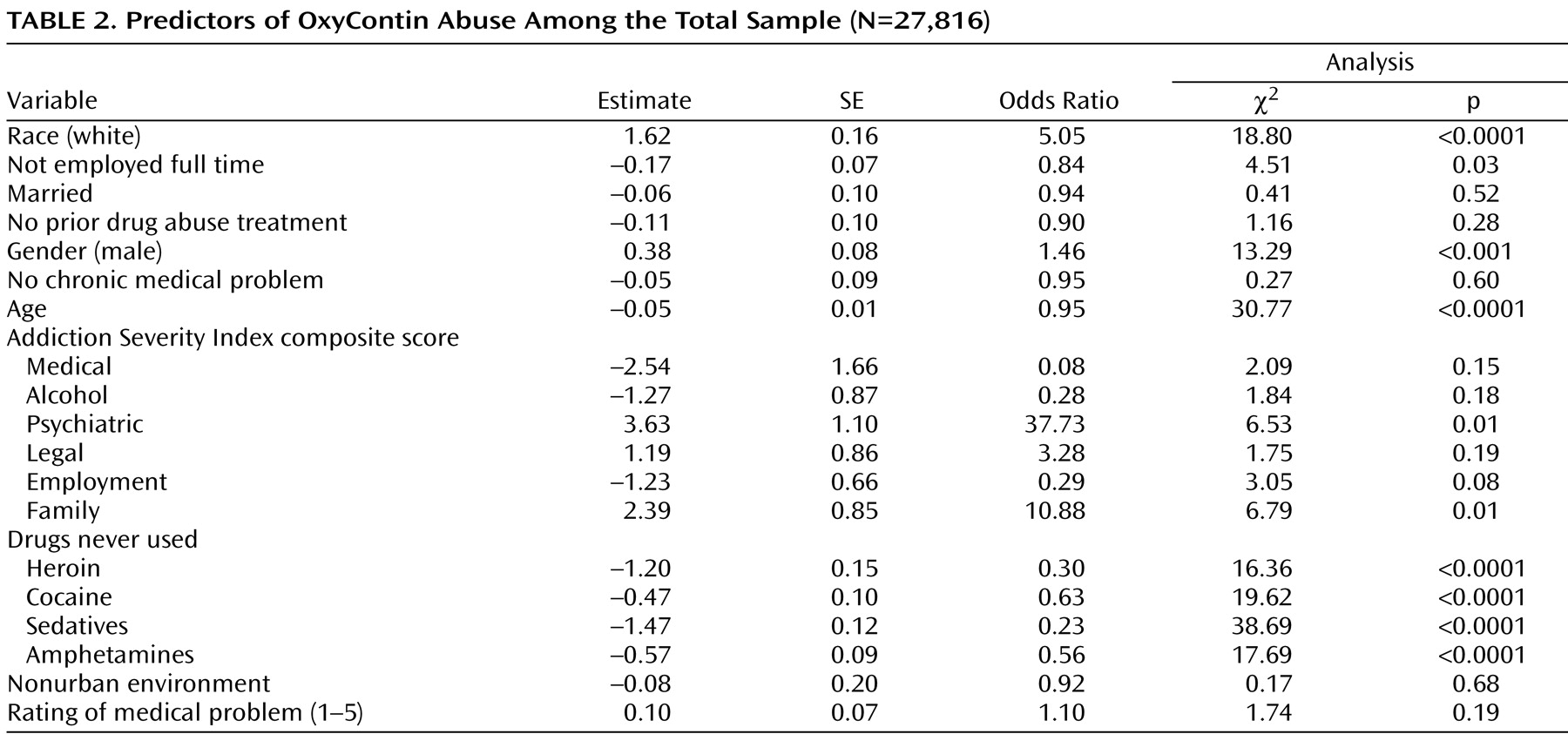
Predictors of OxyContin abuse among the total sample
A General Estimating Equation analysis was used to identify variables that differentiated those individuals who abused OxyContin (i.e., to “get high”) from the total sample of all individuals admitted to the treatment programs. Those who reported abuse of OxyContin were significantly more likely to be white (χ
2 =18.80, df=1, p<0.0001), male (χ
2 =13.29, df=1, p<0.001), older (χ
2 =30.77, df=1, p<0.0001), and employed full time (χ
2 =4.51, df=1, p<0.05). The odds of reporting OxyContin abuse increased significantly with higher admission Addiction Severity Index composite scores (indicating greater problems or acuity) on the psychiatric (χ
2 =6.53, df=1, p<0.05) and family (χ
2 =6.79, df=1, p<0.01) problem areas. Finally, the odds of reporting OxyContin abuse were decreased for patients who had not used heroin (χ
2 =16.36, df=1, p<0.0001) or other illicit drugs (all χ
2 values>19; all p values<0.0001 [
Table 2 ]).
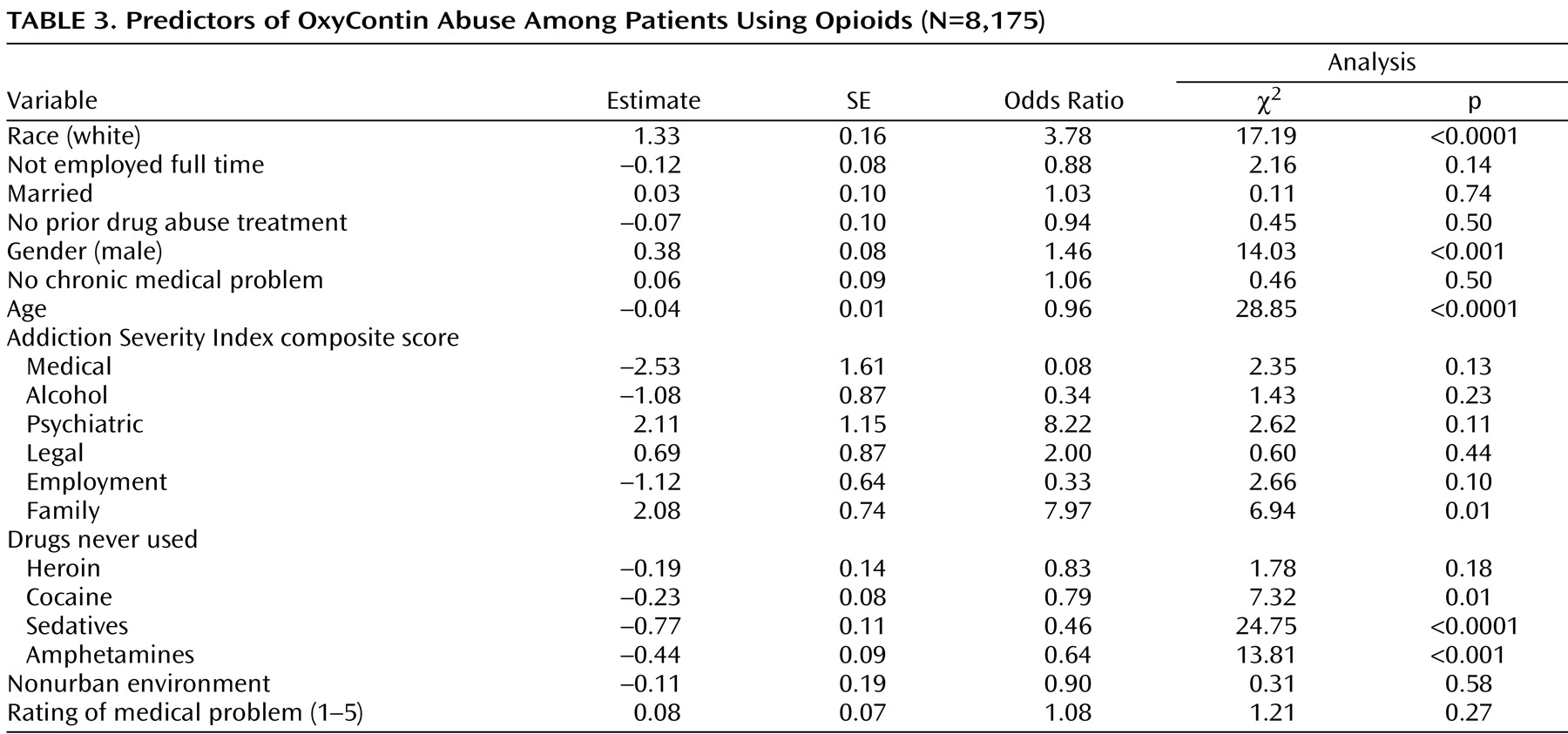
Predictors of OxyContin abuse among patients who used opioids
A separate General Estimating Equation analysis was performed on all patients who reported any opioid use (N=8,175) (i.e., OxyContin, hydrocodone, hydromorphone, or heroin) to differentiate individuals who abused OxyContin from those individuals who used other opioids. Once again, being white (χ
2 =17.19, df=1, p<0.0001), male (χ
2 =14.03, df=1, p<0.001), older (χ
2 =28.85, df=1, p<0.0001), and having greater family problems on the Addiction Severity Index (χ
2 =6.94, df=1, p<0.01) significantly differentiated those who abused OxyContin from those who used other opiates. With regard to other drug use, patients who reported that they had never used cocaine, sedatives, and amphetamines were 21%, 54%, and 46%, respectively, less likely to have abused OxyContin than patients who reported any use of these drugs (
Table 3 ).
OxyContin Abuse—Changes Over Time
We examined changes over time in the prevalence of OxyContin abuse as well as the demographics and problem severity profiles of those reporting its use among the 12,530 individuals admitted to the 27 treatment programs that reported in all quarterly periods from 2002–2004. The General Estimating Equation analysis for those sites indicated no significant changes in the prevalence of those individuals who reported OxyContin use or those individuals who met our criterion for abuse during this time (χ 2 =6.51, df=1, p=0.48). Individuals categorized as “users” of OxyContin ranged from 2%–4% of all admissions per year. Further, examination of all seven Addiction Severity Index composite scores (drug, alcohol, medical, psychiatric, employment, family, legal) among OxyContin “users” during this period revealed no significant changes (p>0.10).
Discussion
Media reports have often portrayed people who receive OxyContin and develop substance abuse problems as “drug naive” individuals or as individuals with “accidental” addiction
(40 –
42), and in turn they have brought about the speculation that this opioid has unique properties that make it more likely to induce or prompt abuse and dependence among the general population. Although some reporters have rescinded their reports or noted that OxyContin abuse may have been overstated
(43), this is the only prescription medication, to our knowledge, that has been compared with “a plague”
(15) or “nuclear bomb”
(15,
16) by the media.
In fact, prior research studies of OxyContin use or abuse among the general population and among those receiving the medication for pain management in specialty clinics have not supported such media claims
(1 –
3,
5,
8 –
11,
44) . These studies have reported that while the rates of OxyContin use have increased since 2000, the proportion of those individuals who are prescribed OxyContin and have shown signs of abuse or dependence are quite low (less than 2%).
This ongoing project measuring the nature and severity of addiction problems among individuals admitted to 157 addiction treatment programs across the United States
(28 –
31) enabled us to examine the prevalence of OxyContin use and abuse among those whose substance use had become severe enough to require treatment for abuse or dependence. While it should be clear that this group is quite different from a general population sample, the group does offer a complementary perspective on the nature of OxyContin use.
We found that 5% (N=1,425) of the 27,816 individuals who were admitted to 157 addiction treatment programs in the United States from 2001–2004 reported ever using OxyContin, with no change in prevalence rates over the course of the study. Only 22% of these individuals who used OxyContin reported receiving the medication through prescription for any medical reason, and 86% of individuals who used OxyContin (whether prescribed or not) acknowledged using the medication primarily to “get high.” Only eight (0.5%) of the 1,425 individuals who used OxyContin in our sample reported no other drug use.
Patients who reported any OxyContin use were also likely to have reported the use of hydromorphone, oxycodone, and hydrocodone (25%, 62%, and 70%, respectively). Although these medications were not the focus of our study, it is clear that within this sample of patients entering addiction treatment programs, those who received OxyContin also used other drugs, especially other pharmaceutical opioids.
It is important to clarify the limitations of this study. First, we should emphasize that this study was not completed in a general population sample. This was a national sample of individuals admitted to adult addiction treatment centers and therefore likely represents those persons with the most severe and complex substance abuse problems. Although this is an important group, its tendencies cannot be generalized to the general population, nor does it address the tendencies of abuse among adolescents presenting for treatment. There are other studies that have examined prescription opioid use among the general population, in emergency rooms, etc. Likewise, additional studies in primary care offices and other types of health care provider service organizations are needed. In addition, while the patients in our study were drawn from a large, randomly selected sample of addiction treatment programs, because of constant and frequent changes in the population of treatment programs in the United States
(38), there simply is no way to maintain a sample of programs that would be nationally representative. Moreover, for implementation of the study, the sample was weighted to be likely to overinclude programs in urban or suburban areas
(45), and OxyContin abuse may be more prevalent in rural sections of the Eastern and Northeastern regions of the country.
Conclusion
One main finding of this study was that most of the OxyContin use reported in the sample of individuals seeking addiction treatment did not originate from physician prescriptions, but rather from illicit sources, such as family, friends, or other illegitimate sources. Clearly, the pharmaceutical opioid problems of the individuals in this sample were part of a larger pattern of alcohol and other drug use—the problems were not “accidental,” secondary to prescribed use for pain or other medical problems. These results also suggest that those who suffer from OxyContin abuse or dependence share many characteristics with those who are dependent on other classes of drugs. In turn, this suggests that treatments that have been shown to be effective in heroin-dependent patients (including methadone, buprenorphine, and psychosocial treatments) and others may also be effective in persons dependent on OxyContin or other prescription opioids.