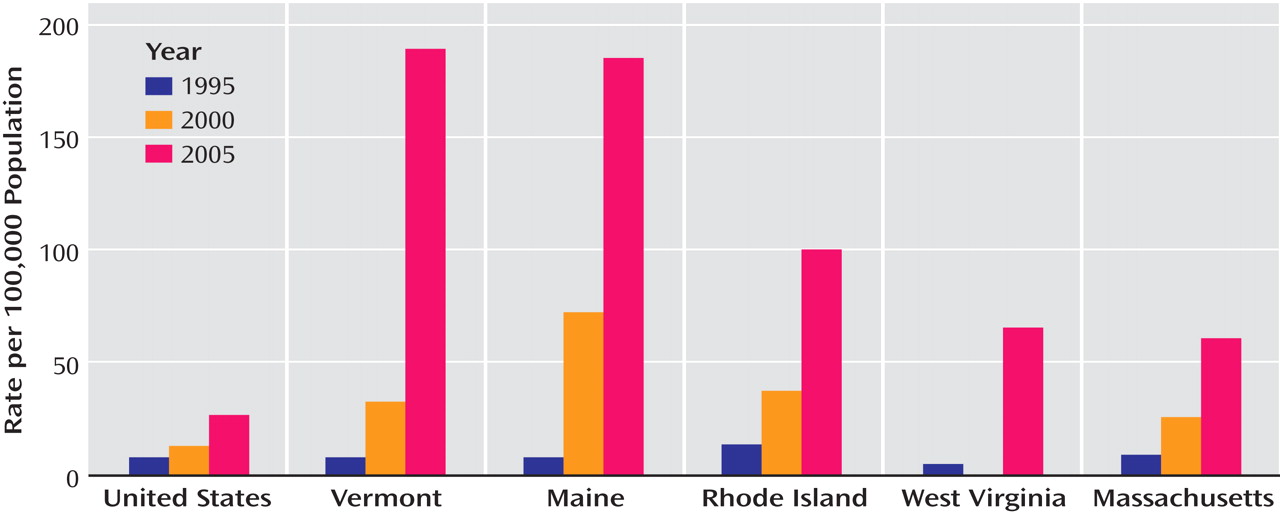
Recent epidemiological reports suggest that prescription opiate use has increased sharply in many parts of the United States (
Figure 1 )
(1 –
4) . There is evidence that the Internet has become a new source of prescription drugs, increasing their availability and eliminating the need for a prescribing physician. In addition, in response to concerns about the undertreatment of pain, more opiate painkillers are being prescribed
(5) . Is there an epidemic of prescription opiate use? Who are the users of prescription opiates? Effective prevention, public information, and treatment policies require sound drug use epidemiological data to ensure that policy making is not hijacked by stories of celebrity arrests and media-generated hysteria.
In this issue of the Journal, the article by Carise et al. provides some very useful data on a sample of OxyContin users who have been admitted into a variety of treatment programs around the United States. The authors present data from a very valuable drug abuse indicator system, the Drug Evaluation Network System (DENS), established to collect information on individuals admitted to substance abuse treatment at selected specialty centers throughout the United States. The data in DENS are collected using the well-established Addiction Severity Index. The use of this validated data collection instrument results in data with known validity and reliability parameters. DENS provides a rich set of timely data, captured and transmitted electronically at the time of admission, which allows for rapid analysis and information to policy makers about changes in the characteristics of patients admitted to the network’s participating treatment agencies. Access to these current data is important for the substance abuse monitoring system in the United States.
The data presented by Carise et al. offer some very useful insights into the nature of the patient population that has entered treatment at a set of treatment centers with OxyContin as their primary drug of choice. It is clear that many of the people who enter treatment in these treatment programs for OxyContin abuse/dependence are not naive individuals with accidental addiction who were introduced to opiate painkillers by their physicians as reported by the media. The individuals admitted to the treatment organizations participating in DENS are, for the most part, individuals with extensive drug use histories and involvement in the criminal justice system. Their use of OxyContin as their current preferred drug is related to the fact that in some parts of the United States there is easy access to OxyContin
(1) . Hence, OxyContin use among this group simply represents a drug preference based primarily on convenience. This is an important finding and adds a useful perspective to understanding the nature of the drug abuse problems that are associated with the use of OxyContin.
The sample examined in the Carise et al. study is an important segment of the OxyContin using population. However, as noted by the authors, the DENS sample is not intended to be a representative sample of the general population. The DENS system collects information about individuals admitted into treatment programs that have volunteered to participate in the DENS program. As the authors acknowledge, it is not known how representative the DENS treatment program sample is of the entire addiction treatment system, and as the authors suggest, the programs tend to be generally urban and suburban, while many of the OxyContin reports have described major problems in rural areas. One predominantly rural state, Maine, has witnessed an increase of methadone programs in the past 5 years and an increase in annual methadone admissions from 1,158 in 2002 to 1,677 in 2005
(6) . It would be of great interest to determine if this new influx of patients to new methadone programs had the same chronic history of addiction as reported in the DENS data.
The OxyContin phenomenon has affected a number of states.
Figure 1 shows the rate of admissions reported to the Treatment Episode Data Set (TEDS) of “Other Opiates” per 100,000 individuals in the population from 1995–2005 for the United States and for the five states with the highest rates in 2005
(3) . The Other Opiate category is defined as codeine, hydromorphone, morphine, meperidine, opium, oxycodone, and any other drug with morphine-like effects.
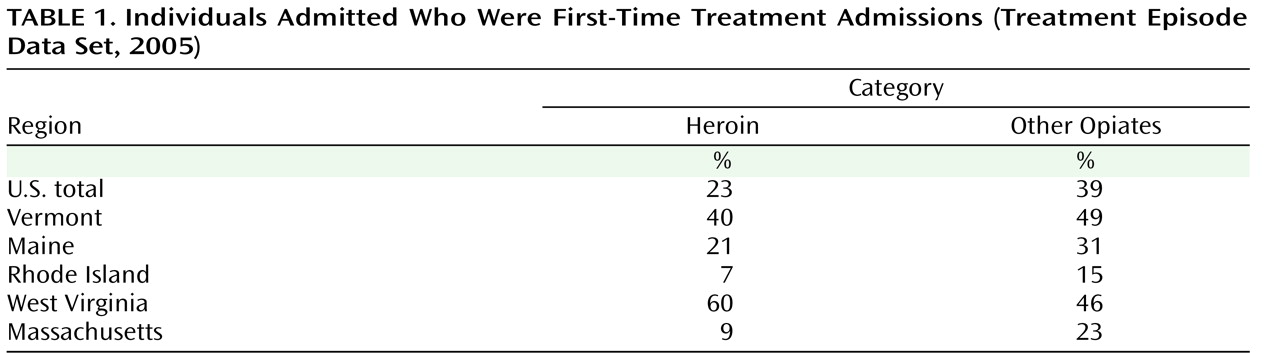
Table 1 shows the percent of individuals admitted with a primary problem with heroin or other opiates in 2005. Notice that in states that have had a long-standing problem with heroin (e.g., Massachusetts and Rhode Island), the proportion of first-time admissions is low—consistent with Carise et al.’s finding that only 22% of the DENS clients had no previous treatment admissions—while in those states that have developed problems with abuse of other opiates (including OxyContin) more recently (e.g., Maine and Vermont), the proportion of first-time admissions for problems with heroin or other opiates is much higher
(7) . This may indicate two different groups of users: long-term users, as identified by Carise et al., and novice users whose introduction into opiate use may be the result of their exposure to OxyContin.
In addition, as noted by the authors, the substance abuse specialty treatment system has historically become a place where the most difficult patients are referred and treated. Large proportions of individuals who walk through the doors of these specialty clinics are long-term drug users who use multiple drugs, are involved in the criminal justice system, and have numerous previous treatment episodes. Not surprisingly, OxyContin users who enter treatment in the specialty care addiction treatment system have many characteristics in common with others who enter treatment in these clinics. These data clearly support the view that OxyContin users who access the specialty treatment clinics in the DENS sample are not naive, accidental, first-time users.
However, there is no way of knowing if the OxyContin users who end up under the care of physicians prescribing buprenorphine in office-based practices have the same characteristics as the DENS sample. It is possible that these naive individuals with accidental addiction (if they do exist) do not seek treatment at the specialty treatment centers. If in fact there is a new unique cohort of addicted individuals who have become dependent on OxyContin as a result of their “accidental” misuse of pain medication, it is highly possible that these individuals would not seek assistance at the treatment clinics where chronic, polydrug, criminally involved, previously treated individuals with addiction go for assistance. The stigma of entering treatment in a specialty clinic (particularly many of the publicly funded clinics that are often in minority neighborhoods characterized by poverty) may deter entry into these clinics, especially since from the DENS sample and previous samples it appears that a majority of OxyContin users are Caucasian.
The question of who are the users of OxyContin is an important one. This is a drug problem in which the drug supply has emerged from a disturbing new set of sources. Gaining an accurate picture of who this drug use phenomenon affects is a bit like the story of the blind men who were asked to touch one part of an elephant and then describe the entire animal. Each set of drug use data from a specific source offers a detailed description of that particular sample, but it is never clear whether each sample accurately reflects the nature of other samples. We need a more complete picture of the entire elephant before we can be sure who has and who has not been affected by the OxyContin problem.