Despite its severity and stability
(1,
2), narcissistic personality disorder is one of the least studied personality disorders. The goals of this study were to gain a richer understanding of narcissistic personality disorder by identifying the most characteristic and the most distinctive features of the disorder and to identify subtypes of the disorder.
Previous research indicates that the phenomenon of narcissism may be broader than the DSM-IV formulation. In one study, a random national sample of psychologists and psychiatrists described patients with personality disorders by using the Shedler-Westen Assessment Procedure–200
(3,
4), an instrument that allows clinicians to record their psychological observations systematically and reliably. The portrait that emerged of narcissistic personality disorder encompassed DSM-IV criteria but also included psychological features absent from DSM-IV, notably painful insecurity, interpersonal vulnerability, and feelings of fraudulence.
An emerging literature also supports the long-held clinical hypothesis that there are two subtypes of narcissistic individuals, grandiose and vulnerable
(5 –
11) . The former has been described as “grandiose, arrogant, entitled, exploitative, and envious” and the latter as “overly self-inhibited and modest but harboring underlying grandiose expectations for oneself and others” (
5, pp. 188–189). The two subtypes have different correlates with external criterion variables, supporting the validity of the distinction (see reference
10, for example).
In this article, we report data from a national sample of patients described by their treating clinicians using the Shedler-Westen Assessment Procedure–II (SWAP-II;
3,
4,
12 –
14), the latest edition of the instrument. The study has two goals: to refine the construct of, and diagnostic criteria for, narcissistic personality disorder and to empirically identify subtypes of the disorder. Our research approach is analogous to a diagnostic field trial that tests alternative diagnostic criteria. However, the logistical constraints of field trials (e.g., limited time available for patient assessment, patient contact at only a single time point) limit the number of alternative diagnostic criteria that can be tested and place the diagnostic emphasis on relatively overt signs and symptoms that can be assessed by asking participants direct questions. Overreliance on direct questions may be especially problematic for patients with narcissistic personality disorder, who lack self-awareness or minimize their own psychopathology (see also reference
15 ).
In previous studies, we identified the most descriptive or characteristic features of narcissistic personality disorder but not necessarily the most distinctive features
(3,
12) . For example, lack of empathy is highly descriptive of narcissistic personality disorder but is not specific to the disorder—patients with other personality disorders also lack empathy. In this study, we performed separate analyses to identify the most characteristic and the most distinctive features of narcissistic personality disorder. To identify the most characteristic features, we created composite personality descriptions by aggregating raw SWAP-II item scores across patients diagnosed with narcissistic personality disorder. To identify the most distinctive features, we created composite personality descriptions by aggregating standardized SWAP-II item scores (z scores). The latter procedure deemphasizes items that are descriptive of personality disorder patients in general and highlights items specific to each personality disorder.
Results
The total sample included 1,201 patients. Of these, 255 met DSM-IV criteria for narcissistic personality disorder based on the axis II checklist (five or more diagnostic criteria checked), 122 received the diagnosis based on the personality disorder construct ratings (ratings ≥4), and 101 received the diagnosis by both methods; thus, 83% of those who received a diagnosis via the construct ratings also met DSM-IV criteria. Narcissistic personality disorder construct ratings correlated highly with the number of DSM-IV criteria met (r=0.71, df=1194, p<0.001). Of patients who met criteria using both methods, 71% were male; their mean age was 44 years (SD=14.01); and 87% were Caucasian, 8% African American, 3% Hispanic, and 2% other.
Composite Portraits of Narcissistic Personality Disorder: Characteristic Features
To identify the SWAP-II items that are most central and defining of narcissistic personality disorder, we created composite descriptions by aggregating (averaging) the SWAP-II item scores across all patients diagnosed with the disorder. The psychometric effect of aggregation is that idiosyncrasies of individual patients and clinicians (i.e., error variance) cancel out
(18,
19), and only those items that consistently receive high scores across patients with narcissistic personality disorder receive high scores in the composite description. Thus, the high-scoring SWAP-II items reflect the core psychological features shared by patients with narcissistic personality disorder.
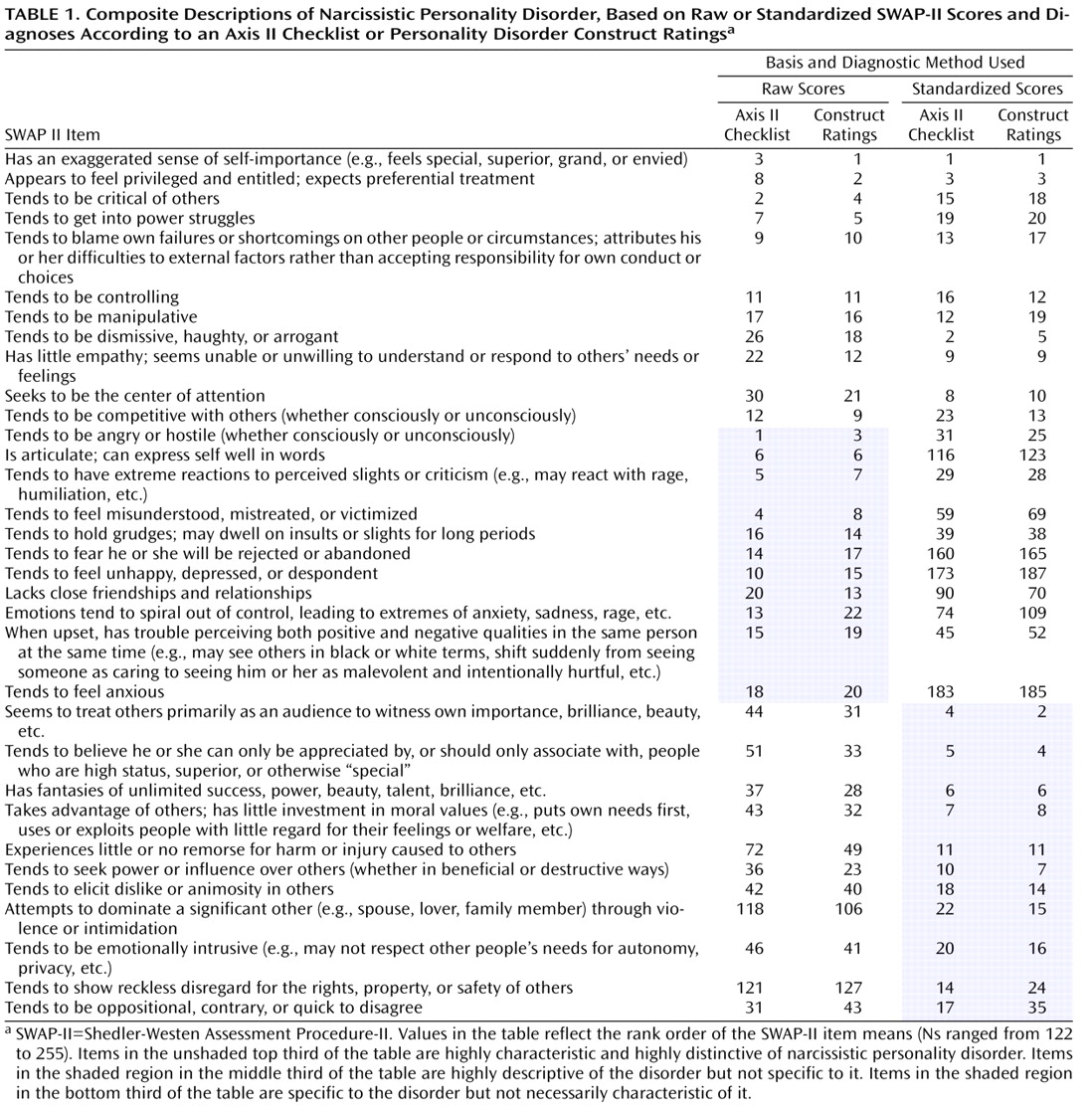
Table 1 lists the SWAP items that are most defining of the disorder.
The items listed in
Table 1 are based on four different composite descriptions of narcissistic personality disorder. The first is a composite description of patients who met DSM-IV criteria for the disorder based on the axis II criterion checklist (
Table 1, column 1). The second is a composite description of patients diagnosed with the disorder on the basis of personality disorder construct ratings (with ratings ≥4 treated as positive diagnoses;
Table 1, column 2). The values in the table indicate the rank order of the SWAP items in each description. The rankings indicate the relative importance of the items in describing narcissistic personality disorder. For example, in the composite description based on personality disorder construct ratings (column 2), the five top ranked items were: “Has an exaggerated sense of self-importance (e.g., feels special, superior, grand, or envied)”; “Appears to feel privileged and entitled; expects preferential treatment”; “Tends to be angry or hostile (whether consciously or unconsciously)”; “Tends to be critical of others”; and “Tends to get into power struggles.” The first two descriptors resemble DSM-IV criteria; the next three do not. Thus, patients with narcissistic personality disorder appear more hostile, critical, and power-oriented than DSM-IV would lead us to expect.
Composite Portraits of Narcissistic Personality Disorder: Most Distinctive Items
The composite descriptions described above (created by aggregating raw SWAP-II scores) identify features that are characteristic of narcissistic personality disorder but are not necessarily specific to the disorder. For example, patients with narcissistic personality disorder are angry and hostile, but so are patients with other personality disorders (e.g., borderline, paranoid). Such descriptors are necessary for an accurate and comprehensive portrait of narcissistic personality disorder, but they do not necessarily distinguish this disorder from “near neighbor” disorders.
To identify the most distinctive diagnostic features, we mathematically transformed the SWAP-II item scores to create standardized scores (z scores), so that each SWAP-II item score would be expressed as a deviation from the sample mean for that item, expressed in standard deviation units. In practical terms, the effect of this transformation is to deemphasize items that have high scores in the psychiatric sample generally and emphasize items that uniquely distinguish specific personality disorders within the sample. For example, most patients in a psychiatric sample experience dysphoric affect (e.g., “Tends to feel unhappy, depressed, or despondent”), and so do patients with narcissistic personality disorder. However, the item is not particularly helpful for distinguishing narcissistic personality disorder from other personality disorders.
To identify the SWAP-II items most distinctive of narcissistic personality disorder, we created composite descriptions by aggregating standardized SWAP-II scores across patients with the disorder. In
Table 1, columns 3 and 4 contain the item rankings in the composite description of patients who met DSM-IV criteria for narcissistic personality disorder based, respectively, on the axis II criterion checklist and on personality disorder construct ratings.
Again, the rankings indicate the relative importance of the items. For example, the item “Seems to treat others primarily as an audience to witness own importance, brilliance, beauty, etc.” received the second highest rank in the composite description based on personality disorder construct ratings (column 4). This personality characteristic may not be prominent in all patients with narcissistic personality disorder; when it is prominent, however, it may be pathognomonic.
Identifying Optimal Diagnostic Criteria
The items in
Table 1 are grouped to facilitate interpretation. The items in the top third of the table (no shading) are both highly characteristic and highly distinctive of narcissistic personality disorder. These items ranked among the top 30 most descriptive items in all four composite descriptions.
Items in the shaded region in the middle third of the table are highly descriptive of narcissistic personality disorder but not specific to it. These items are necessary to provide a clinically complete description of narcissistic personality disorder, even though they may apply to other personality disorders as well. Items in this section had top rankings in the composite descriptions based on raw SWAP-II scores (columns 1 and 2) but not in the composite descriptions based on standardized SWAP-II scores (columns 3 and 4).
Finally, items in the shaded region in the bottom third of the table are specific to narcissistic personality disorder but not necessarily characteristic of the average patient with the disorder. In other words, these personality features are not necessarily common in narcissistic personality disorder, but they are highly diagnostic when present.
Key findings are that interpersonal vulnerability and underlying emotional distress are core features of narcissistic personality disorder. The typical patient tends to fear rejection and abandonment; tends to feel misunderstood, mistreated, or victimized; tends to have extreme reactions to perceived slights or criticism; tends to feel unhappy, depressed, or despondent; and tends to feel anxious. Other prominent features include anger and hostility, difficulty in regulating affect, interpersonal competitiveness, power struggles, and a tendency to externalize blame. These features are absent from the DSM-IV description of narcissistic personality disorder, and they are unlikely to be identified using research methods that rely exclusively on what patients with the disorder report about themselves (e.g., via questionnaires or structured interviews).
Reliability of the Composite Swap-II Descriptions
The reliability of a composite SWAP-II description is measured by Cronbach’s alpha. The logic is identical to computing the reliability of a psychometric scale, except that patients are treated as “items” (columns in the data file) and SWAP-II items are treated as cases (rows in the data file). This approach is well established
(14,
20) . Values for Cronbach’s alpha for this study ranged from 0.94 to 0.98, suggesting that the descriptions of narcissistic personality disorder in
Table 1 contain very little error variance.
Subtypes of Narcissistic Personality Disorder
Our second analysis was designed to identify subtypes or variants of narcissistic personality disorder. We applied Q-factor analysis to analyze the SWAP-II descriptions of patients meeting the diagnosis of narcissistic personality disorder by both diagnostic methods (DSM-IV and construct ratings). We conservatively included only those patients who met both sets of diagnostic criteria because DSM-IV criteria tend to overdiagnose all personality disorders. Thus, imposing the additional criterion of positive diagnosis using the construct ratings minimizes the possibility of identifying artifactual subtypes.
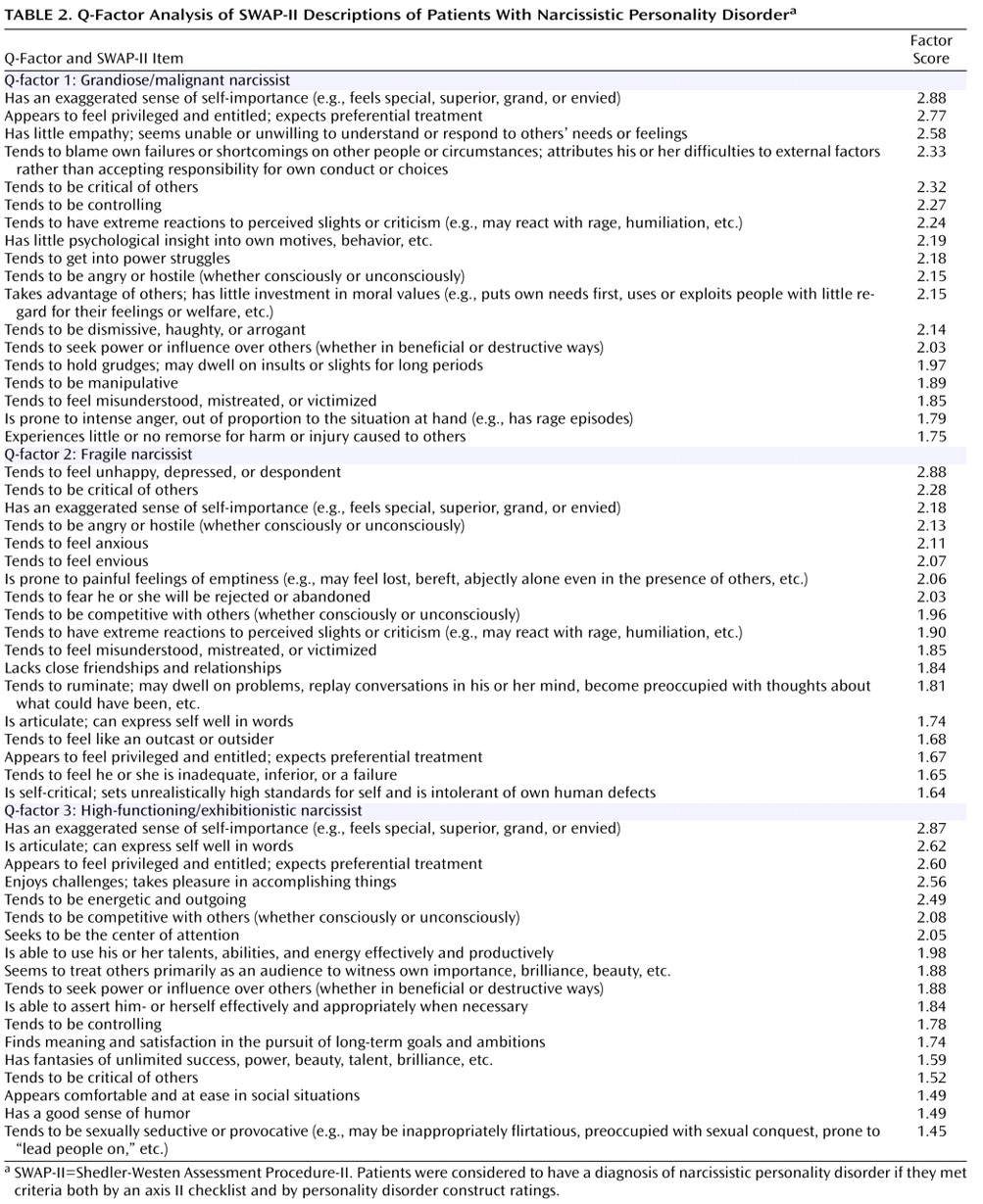
Q-factor analysis is computationally equivalent to conventional factor analysis except that it identifies groupings of similar people, whereas conventional factor analysis identifies groupings of similar variables. We used standard exploratory factor analysis with principal axis factoring and an oblique (promax) rotation. We retained the first three of the four rotated factors. The factor scores listed in
Table 2 indicate the importance or centrality of the items in defining each subtype of narcissistic personality disorder. The Q-factors showed low to moderate intercorrelations with each other (r values ranging from –0.01 to 0.35), indicating that the subtypes do represent distinct groups.
We labeled the narcissistic personality disorder subtypes grandiose/malignant, fragile, and high-functioning/exhibitionistic. Grandiose/malignant narcissists exploit others with little regard for their welfare, and (unlike other narcissistic patients) their grandiosity appears to be primary rather than defensive or compensatory. Fragile narcissists experience feelings of grandiosity and inadequacy, suggesting alternating cognitive representations of self (superior versus inferior), defensive grandiosity, or a grandiosity that emerges under threat. High-functioning/exhibitionistic narcissists are grandiose, competitive, attention seeking, and sexually seductive or provocative, and also have significant psychological strengths (e.g., being articulate, energetic, interpersonally comfortable, achievement oriented).
Relationships With Criterion Variables
In a valid taxonomy, different diagnoses should show different relationships with external (criterion) variables
(21,
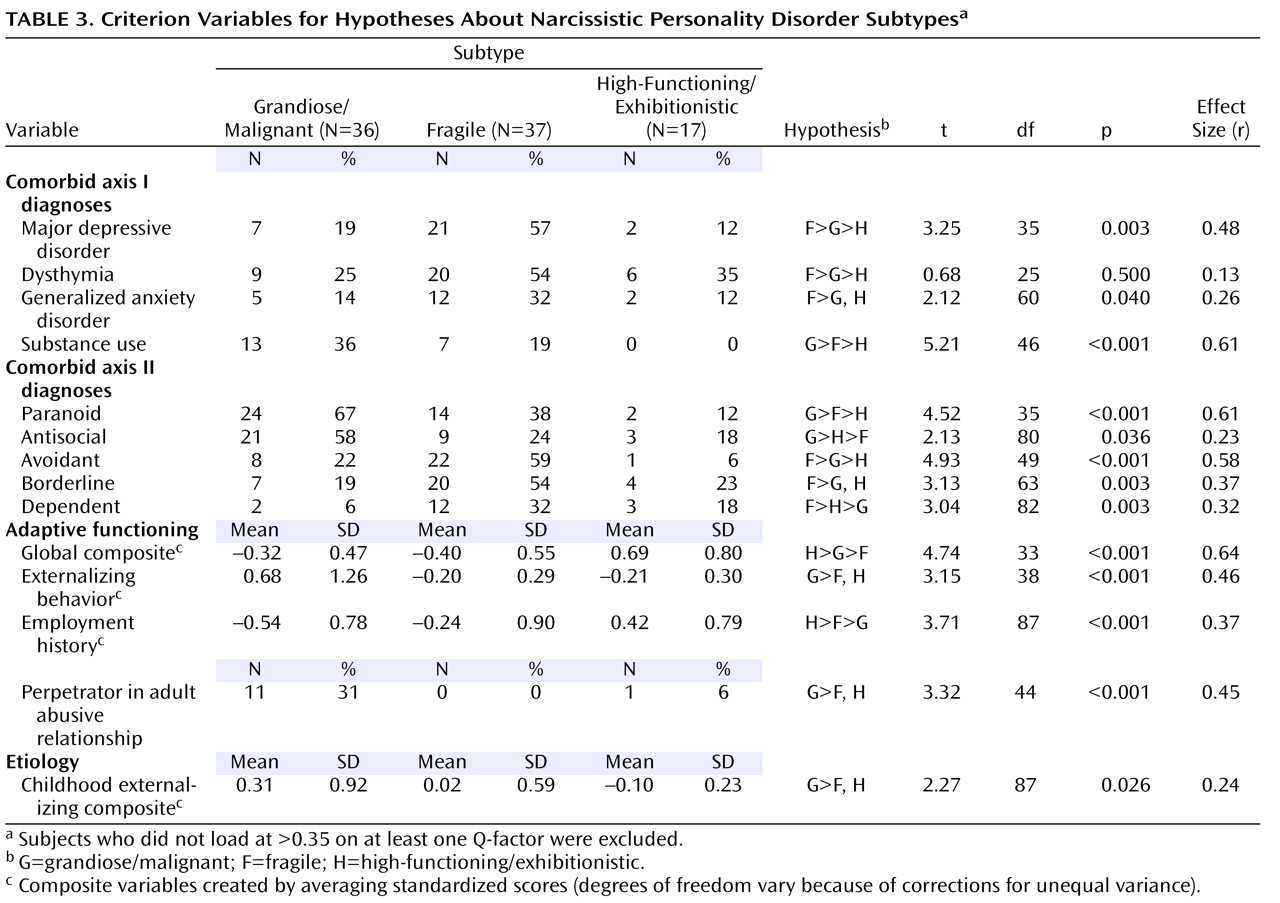
22) . To provide preliminary data on the validity of these subtypes, we conducted contrast analyses on variables predicted a priori to differ across subtypes (
Table 3 ). We assigned patients to subtypes for these analyses depending on their highest factor loadings, provided they loaded >0.35 on at least one Q-factor (in Q-factor analysis, patients load on factors, indicating the degree to which they represent good “exemplars” of the diagnosis). This procedure resulted in 90 (89%) patients receiving a subtype classification.
Overall, we predicted that patients with the high-functioning subtype would have the least comorbidity with other disorders and the highest adaptive functioning; those with the fragile subtype would have the most comorbidity with mood and anxiety disorders and with avoidant, borderline, and dependent personality disorders and the lowest adaptive functioning; and patients with the grandiose/malignant subtype would have the most comorbidity with substance use disorders and paranoid and antisocial personality disorders. These hypotheses were largely supported, as shown in
Table 3 .
Discussion
Empirically Identifying Optimal Diagnostic Criteria
Our findings suggest that DSM-IV criteria are too narrow, underemphasizing aspects of personality and inner experience that are empirically central to narcissistic personality disorder. Some items were both characteristic and distinctive of the disorder and hence are prime candidate criteria for future editions of DSM. Other items are characteristic of typical patients with narcissistic personality disorder but do not necessarily distinguish this disorder from other personality disorders. These items include a mix of features common to most personality disorder patients (e.g., “Tends to feel unhappy, depressed, or despondent”) and features shared with other specific personality disorders, such as paranoid, antisocial, and borderline (e.g., “Tends to be angry or hostile”). DSM task forces have attempted to minimize overlap between diagnostic criteria by excluding such items from the criteria for narcissistic personality disorder, but doing so may not provide a faithful portrait of the syndrome. Overall, the findings suggest that the DSM-IV criteria lack sufficient breadth to accurately capture the phenomenon of narcissism.
Subtypes of Narcissistic Personality Disorder
Q-factor analysis identified three subtypes of narcissistic personality disorder. Grandiose/malignant narcissism is characterized by seething anger, interpersonal manipulativeness, pursuit of interpersonal power and control, lack of remorse, exaggerated self-importance, and feelings of privilege. Grandiose/malignant narcissists do not appear to suffer from underlying feelings of inadequacy or to be prone to negative affect states other than anger. They have little insight into their own behavior and tend to blame others for their problems.
Fragile narcissism is characterized by grandiosity that serves a defensive function, warding off painful feelings of inadequacy, smallness, anxiety, and loneliness. The fragile narcissist wants to feel important and privileged, and when defenses are operating effectively, he does. However, when the defenses fail, there is a powerful undercurrent of negative affect and feelings of inadequacy, often accompanied by rage.
High-functioning/exhibitionistic narcissism has received little empirical attention but is well represented in the clinical literature (e.g., see reference
23 ). Patients in this subtype have an exaggerated sense of self-importance but are also articulate, energetic, and outgoing. They tend to show good adaptive functioning and use their narcissism as a motivation to succeed.
Validity analyses indicate clear differences among the subtypes. Fragile narcissists suffer the most; they have the poorest global adaptive functioning and the highest comorbidity with major depressive disorder and generalized anxiety disorder. Grandiose/malignant narcissists have the most problems with substance abuse and the most externalizing behavior (e.g., spouse abuse). High-functioning/exhibitionistic narcissists have relatively good adaptive functioning and less psychiatric comorbidity.
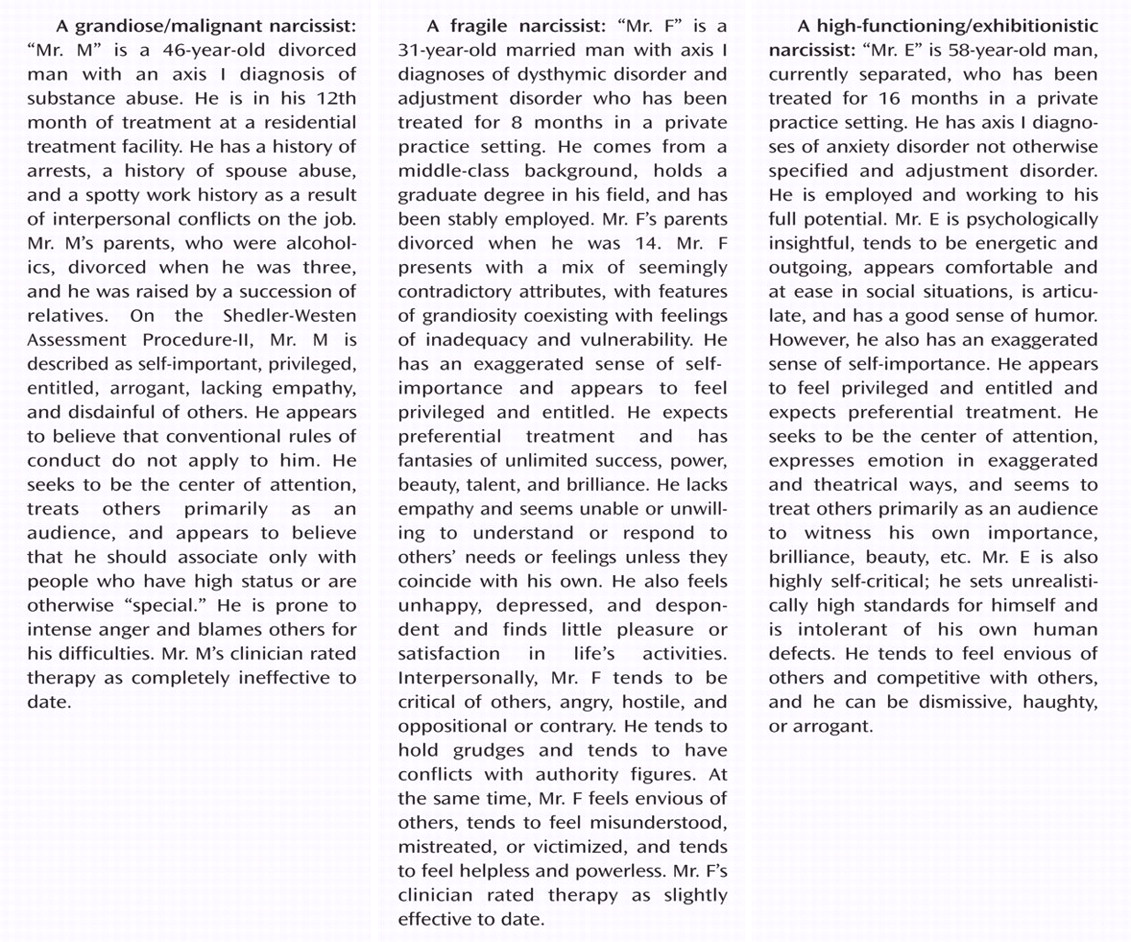
Figure 1 provides a case vignette for each subtype, to better illustrate the syndromes.
While Q-factor analysis is purely empirical and therefore theory blind, it is noteworthy that the subtypes correspond to subtypes of narcissistic personality described in the Psychodynamic Diagnostic Manual
(24), which distinguishes between “arrogant/entitled” and “depressed/depleted” variants of narcissism. The Psychodynamic Diagnostic Manual also notes that each personality disorder has a less disturbed variant that may be considered a personality pattern or style rather than a disorder.
Treatment data are as yet unavailable, but these subtypes likely have different treatment implications. Grandiose/malignant narcissists likely have the poorest prognosis. They do not experience the kind of emotional pain that would motivate them to work in psychotherapy, and they would likely seek to manipulate the clinician or establish a “one-up” position. Fragile narcissists may respond best to empathic understanding and interventions that acknowledge underlying pain, insecurity, and vulnerability. These patients would require the clinician’s help to tolerate feelings of vulnerability without resorting to grandiosity or devaluation of others. High-functioning/exhibitionistic narcissists might benefit from an interpretive, insight-oriented approach (e.g., to increase awareness of how narcissistic defenses erode possibilities for more meaningful attachments).
Although our analyses identified clear subtypes of narcissistic personality disorder, this does not imply that personality syndromes must be diagnosed categorically, as either present or absent. Instead, we view composite personality descriptions as diagnostic prototypes that represent personality syndromes in their ideal or pure form. A given patient may approximate or match the prototype to a greater or lesser extent and can therefore be diagnosed on a continuum based on the degree of resemblance or match with the prototype (see references
13,
25,
26) .
Limitations
The primary limitation of this study is its exclusive reliance on clinician-consultants as informants. Ideally, patients would have been diagnosed by one observer and assessed using the SWAP-II by another. However, most published personality disorder studies also rely on a single informant—the patient (e.g., via self-report questionnaires or responses to structured interview questions). The quantified observations of experienced psychiatrists and clinical psychologists (with an average of 19.8 years of practice experience and 17.3 months of contact with the patient assessed) are no less credible than the self-descriptions of patients with personality pathology. In fact, self-report measures of narcissism show virtually no correlation with informant reports, suggesting considerable biases in the self-descriptions of narcissistic individuals
(27) . In contrast, SWAP-II scale scores provided by treating clinicians correlate highly (on average, r=0.80) with the same scales assessed by independent interviewers
(28,
29) . The findings are also unrelated to theoretical orientation or other aspects of professional training
(30,
31) . If clinician biases exist, they appear to account for little variance in SWAP-II ratings.