Meta-Analysis of the Symptom Structure of Obsessive-Compulsive Disorder
Abstract
Objective:
Method:
Results:
Conclusions:
Method
Search Strategy for Identification of Studies
Selection of Studies
Meta-Analytic Procedure Used
Results
Included Studies
| Author | Year | N | Age | Language | Current Versus Lifetime Symptoms | Symptom Scoring System | Type | Factor Rotation Method | Factor Number | Factors |
|---|---|---|---|---|---|---|---|---|---|---|
| Baer | 1994 | 107 | Adult | English | Current | Symptom severity | Category | Varimax | 3 | Factor 1: Hoarding obsessions and compulsions, repeating, ordering, counting (20.7%) |
| Factor 2: Contamination, cleaning, somatic, checking (16.0%) | ||||||||||
| Factor 3: Aggression, sexual, religious (11.3%) | ||||||||||
| Hantouche and Lancrenon | 1996 | 615 | Adult | Non-English (French) | Current | Present/absent | Both | Varimax | 3 | Factor 1: Hoarding obsessions and compulsions, symmetry, repeating, ordering, and checking |
| Factor 2: Aggressive, sexual, religious, miscellaneous obsessions and compulsions | ||||||||||
| Factor 3: Cleaning, contamination, and somatic obsessions | ||||||||||
| Leckman et al. | 1997 | 292 | Adult | English | Lifetime | Symptom number | Category | Varimax | 4 | Factor 1: Aggression, sexual, religious, somatic, checking (30.1%) |
| Factor 2: Symmetry, ordering, repeating, counting (13.8%) | ||||||||||
| Factor 3: Contamination, cleaning (10.2%) | ||||||||||
| Factor 4: Hoarding obsessions and compulsions (8.5%) | ||||||||||
| Mataix-Cols et al. | 1999 | 354 | Adult | English | Current | Symptom severity | Category | Varimax | 5 | Factor 1: Symmetry, ordering, repeating, counting (19.0%) |
| Factor 2: Hoarding obsessions and compulsions (13.8%) | ||||||||||
| Factor 3: Contamination, cleaning (12.7%) | ||||||||||
| Factor 4: Aggressive, checking (10.4%) | ||||||||||
| Factor 5: Sexual, religious (9.7%) | ||||||||||
| Tek and Ulug | 2001 | 45 | Adult | Non-English (Turkish) | Current | Present/absent | Category | Varimax | 5 | Factor 1: Contamination, cleaning, repeating (17.8%) |
| Factor 2: Symmetry, somatic, ordering (15.2%) | ||||||||||
| Factor 3: Aggressive, counting (13.7%) | ||||||||||
| Factor 4: Sexual, religious (9.7%) | ||||||||||
| Factor 5: Hoarding compulsions and checking (9.2%) | ||||||||||
| Girishchandra and Khanna | 2001 | 202 | Adult | Non-English (India) | Lifetime | Present/absent | Item | Varimax | 5 | Factor 1: Contamination, cleaning (14.3%) |
| Factor 2: Symmetry, ordering, hoarding obsessions and compulsions (6.4%) | ||||||||||
| Factor 3: Harm, checking (5.4%) | ||||||||||
| Factor 4: Superstitious fears, mental rituals, and need to touch, tap, and rub (4.6%) | ||||||||||
| Factor 5: Sexual and religious (4.2%) | ||||||||||
| Mataix-Cols et al. | 2002 | 153 | Adult | English | Current | Present/absent | Category | Varimax | 5 | Factor 1: Aggressive, religious, checking, repeating, and counting (23.3%) |
| Factor 2: Contamination, cleaning (13.3%) | ||||||||||
| Factor 3: Symmetry, ordering, counting (10.9%) | ||||||||||
| Factor 4: Hoarding obsessions and compulsions (8.3%) | ||||||||||
| Factor 5: Sexual, somatic (7.9%) | ||||||||||
| Cavallini et al. | 2002 | 180 | Adult | Non-English (Italian) | Lifetime | Symptom number | Category | Varimax | 5 | Factor 1: Contamination, cleaning (17.0%) |
| Factor 2: Hoarding obsessions and compulsions (13.0%) | ||||||||||
| Factor 3: Aggressive, sexual, somatic, religious, checking, repeating (11.5%) | ||||||||||
| Factor 4: Symmetry, ordering, religious (9.5%) | ||||||||||
| Factor 5: Repeating, counting, symmetry (8.8%) | ||||||||||
| Feinstein et al. | 2003 | 160 | Adult | English | Current | Present/absent | Both | Varimax | 4 | Factor 1: Symmetry, ordering, repeating, counting (14.2%) |
| Factor 2: Contamination, cleaning, aggressive, checking (14.2%) | ||||||||||
| Factor 3: Hoarding obsessions and compulsions (13.9%) | ||||||||||
| Factor 4: Sexual, religious (11.8%) | ||||||||||
| Denys et al. | 2004 | 335 | Adult | Non-English (Dutch) | Current | Symptom severity | Item | Varimax | 5 | Factor 1: Contamination, cleaning (16.4%) |
| Factor 2: Aggressive, sexual, religious (9.8%) | ||||||||||
| Factor 3: Somatic and checking (5.9%) | ||||||||||
| Factor 4: Symmetry, repeating, ordering, counting, hoarding obsessions and compulsions (5.6%) | ||||||||||
| Factor 5: High-risk and checking (4.0%) | ||||||||||
| Hasler et al. | 2005 | 169 | Adult | English | Lifetime | Present/absent | Category | Varimax | 4 | Factor 1: Aggression, sexual, religious, somatic, checking (19.5%) |
| Factor 2: Symmetry, ordering, repeating, counting (18.6%) | ||||||||||
| Factor 3: Contamination, cleaning (13.7%) | ||||||||||
| Factor 4: Hoarding obsessions and compulsions (12.9%) | ||||||||||
| Kim et al. | 2005 | 124 | Adult | Non-English (Korean) | Current | Symptom Severity | Category | Varimax | 4 | Factor 1: Hoarding obsessions and compulsions, repeating, ordering, counting (34.0%) |
| Factor 2: Contamination, cleaning (11.1%) | ||||||||||
| Factor 3: Aggression, sexual (10.0%) | ||||||||||
| Factor 4: Religious, somatic (7.7%) | ||||||||||
| Delorme et al. | 2006 | 73 | Child | Non-English (French) | Current | Symptom number | Category | Varimax | 4 | Factor 1: Symmetry, checking, repeating, ordering (35.2%) |
| Factor 2: Aggressive, sexual, somatic, counting (12.7%) | ||||||||||
| Factor 3: Contamination, religious, cleaning (11%) | ||||||||||
| Factor 4: Hoarding obsessions and compulsions (8.1%) | ||||||||||
| McKay et al. | 2006 | 137 | Child | English | Current | Symptom number | Category | Oblimin | 4 | Factor 1: Cleaning, checking, repeating, counting, ordering, superstitious behaviors, rituals involving others (17.3%) |
| Factor 2: Aggressive, sexual, magical thinking (15.9%) | ||||||||||
| Factor 3: Contamination, aggressive, sexual, magical thoughts, somatic, religious, repeating, counting, symmetry, rituals involving others (12.7%) | ||||||||||
| Factor 4: Hoarding obsessions and compulsions, somatic, counting, ordering (11.9%) | ||||||||||
| Pinto et al. | 2007 | 293 | Adult | English | Current | Symptom number | Category | Varimax | 5 | Factor 1: Symmetry, ordering, repeating, counting (22.5%) |
| Factor 2: Hoarding obsessions and compulsions (13.3%) | ||||||||||
| Factor 3: Pathological doubt, somatic, checking (12.2%) | ||||||||||
| Factor 4: Contamination and cleaning (10.3%) | ||||||||||
| Factor 5: Aggressive, sexual, religious (7.4%) | ||||||||||
| Cullen et al. | 2007 | 221 | Adult | English | Lifetime | Present/absent | Category | Varimax | 4 | Factor 1: Aggressive, sexual, religious, somatic |
| Factor 2: Cleaning, contamination | ||||||||||
| Factor 3: Symmetry obsessions, repeating, ordering, counting, sensory/motor compulsions | ||||||||||
| Factor 4: Hoarding obsessions and compulsions | ||||||||||
| Matsunaga et al. | 2008 | 343 | Adult | Non-English (Japanese) | Lifetime | Symptom number | Category | Varimax | 4 | Factor 1: Cleaning, contamination (21.2%) |
| Factor 2: Hoarding obsessions and compulsions (14.3%) | ||||||||||
| Factor 3: Symmetry, repeating, ordering (11.9%) | ||||||||||
| Factor 4: Aggression, checking (10.3%) | ||||||||||
| Hasler et al. | 2007 | 418 | Adult | English | Lifetime | Symptom number | Category | Promax | 4 | Factor 1: Aggressive, sexual, religious, somatic, and checking (17.7%) |
| Factor 2: Symmetry, repeating, counting, ordering (15.4%) | ||||||||||
| Factor 3: Cleaning, contamination (15.4%) | ||||||||||
| Factor 4: Hoarding obsessions and compulsions (14.2%) | ||||||||||
| Stein et al. | 2007 | 434 | Adult | English and non-English (12 countries) | Current | Symptom severity | Item | Varimax | 5 | Factor 1: Contamination, cleaning |
| Factor 2: Harm, checking | ||||||||||
| Factor 3: Aggression, sexual and religious | ||||||||||
| Factor 4: Symmetry, repeating, ordering, counting, hoarding obsessions and compulsions | ||||||||||
| Factor 5: Somatic | ||||||||||
| Stewart et al. | 2007 | 231 | Child | English | Lifetime | Symptom number | Category | Promax | 4 | Factor 1: Symmetry, ordering, repeating, checking (27.0%) |
| Factor 2: Contamination, cleaning, aggressive, somatic (14.4%) | ||||||||||
| Factor 3: Hoarding obsessions and compulsions (11.1%) | ||||||||||
| Factor 4: Religious, sexual (9.1%) | ||||||||||
| Mataix-Cols et al. | (in press) | 238 | Child | English | Lifetime | Symptom number | Category | Varimax | 4 | Factor 1: Hoarding obsessions and compulsions, checking (14.1%) |
| Factor 2: Aggressive, sexual, religious (13.7%) | ||||||||||
| Factor 3: Contamination, cleaning, somatic (13.6%) | ||||||||||
| Factor 4: Symmetry, ordering, repeating, checking (13.1%) |
Excluded Studies
Factor Analysis Results for Total Sample
| Variable | Aggression | Contamination | Sexual | Hoarding Obsessions | Religion | Symmetry | Somatic | Cleaning | Checking | Repeating | Counting | Ordering | Hoarding Compulsions |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aggression | 4 | 13 | 0 | 13 | 0 | 8 | 2 | 8 | 1 | 2 | 0 | 0 | |
| Contamination | 0.08 | 0 | 0 | 1 | 1 | 4 | 20 | 2 | 2 | 0 | 0 | 0 | |
| Sexual | 0.64 | 0.00 | 0 | 15 | 0 | 7 | 0 | 4 | 0 | 1 | 0 | 0 | |
| Hoarding obsessions | 0.00 | 0.00 | 0.00 | 0 | 5 | 1 | 0 | 3 | 5 | 5 | 7 | 20 | |
| Religion | 0.61 | 0.04 | 0.77 | 0.00 | 1 | 6 | 1 | 5 | 1 | 1 | 0 | 0 | |
| Symmetry | 0.00 | 0.03 | 0.00 | 0.33 | 0.03 | 1 | 0 | 5 | 13 | 12 | 18 | 5 | |
| Somatic | 0.38 | 0.23 | 0.29 | 0.03 | 0.27 | 0.01 | 4 | 7 | 0 | 1 | 2 | 1 | |
| Cleaning | 0.08 | 0.97 | 0.00 | 0.00 | 0.02 | 0.00 | 0.23 | 3 | 2 | 1 | 0 | 0 | |
| Checking | 0.44 | 0.05 | 0.21 | 0.23 | 0.24 | 0.29 | 0.35 | 0.23 | 7 | 6 | 5 | 4 | |
| Repeating | 0.03 | 0.01 | 0.00 | 0.32 | 0.06 | 0.78 | 0.00 | 0.04 | 0.34 | 16 | 15 | 5 | |
| Counting | 0.05 | 0.00 | 0.01 | 0.32 | 0.03 | 0.70 | 0.01 | 0.03 | 0.33 | 0.78 | 13 | 5 | |
| Ordering | 0.00 | 0.00 | 0.00 | 0.38 | 0.00 | 0.89 | 0.04 | 0.00 | 0.29 | 0.80 | 0.72 | 6 | |
| Hoarding compulsions | 0.00 | 0.00 | 0.00 | 0.99 | 0.00 | 0.33 | 0.03 | 0.00 | 0.24 | 0.32 | 0.32 | 0.35 |
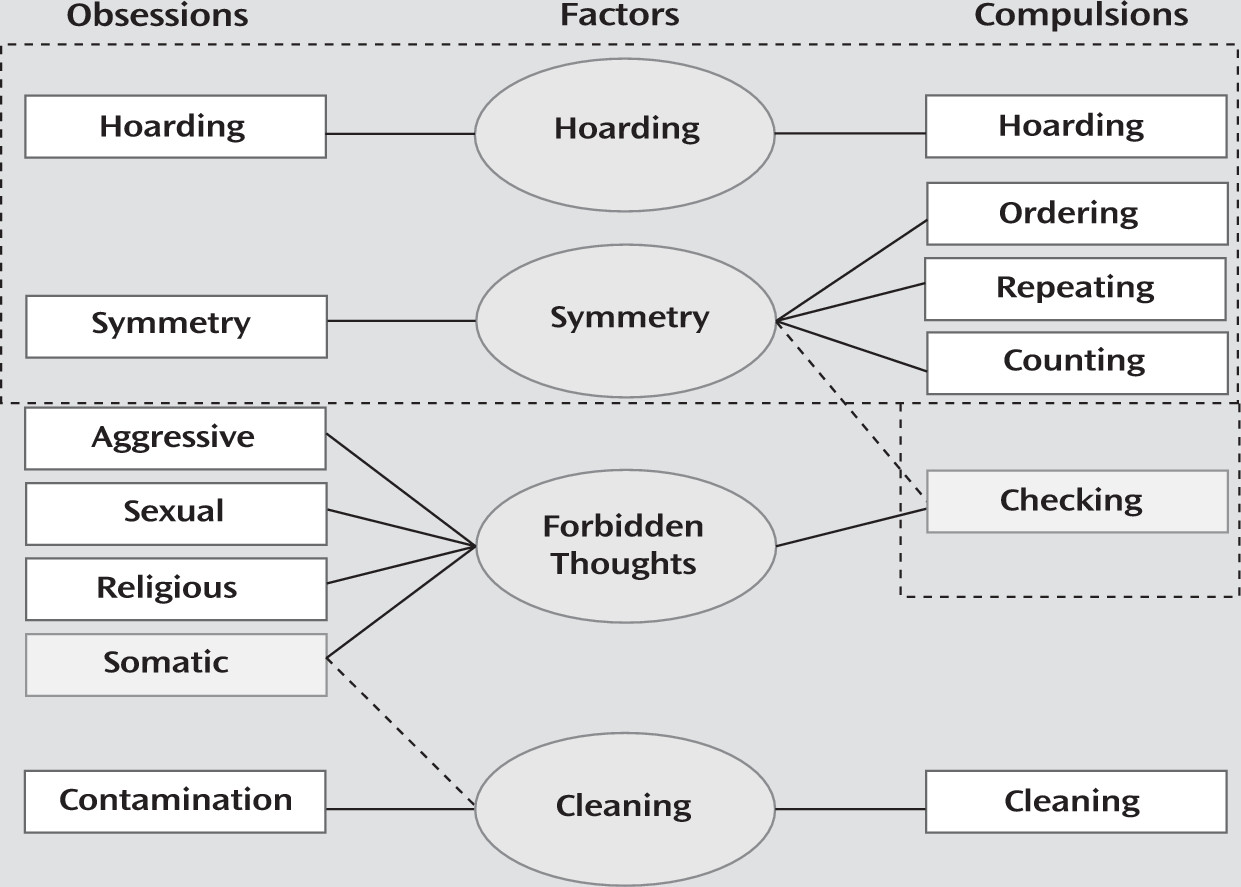
| Symptom Category | Factor | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symmetry | Forbidden Thoughts | Cleaning | Hoarding | |||||||||
| T | A | C | T | A | C | T | A | C | T | A | C | |
| Aggression | 0.01 | 0.01 | −0.01 | 0.86 | 0.87 | 0.72 | 0.05 | 0.00 | 0.40 | −0.01 | −0.01 | 0.00 |
| Contamination | 0.00 | −0.01 | 0.01 | 0.03 | 0.03 | 0.13 | 0.97 | 0.98 | 0.90 | −0.01 | −0.01 | −0.05 |
| Sexual | −0.03 | −0.04 | 0.01 | 0.86 | 0.85 | 0.95 | −0.09 | −0.09 | −0.05 | −0.03 | −0.02 | 0.02 |
| Hoarding obsessions | 0.22 | 0.24 | 0.05 | 0.01 | 0.01 | 0.00 | −0.01 | 0.00 | 0.03 | 0.97 | 0.96 | 0.99 |
| Religious | 0.01 | −0.02 | 0.04 | 0.85 | 0.86 | 0.83 | −0.06 | −0.09 | 0.05 | −0.04 | −0.03 | −0.02 |
| Symmetry | 0.91 | 0.94 | 0.88 | 0.00 | 0.01 | 0.07 | 0.00 | 0.00 | 0.02 | 0.13 | 0.15 | −0.06 |
| Somatic | 0.00 | 0.00 | 0.02 | 0.52 | 0.52 | 0.09 | 0.33 | 0.24 | 0.87 | 0.06 | 0.00 | 0.18 |
| Cleaning | 0.02 | 0.00 | 0.10 | 0.05 | 0.06 | 0.03 | 0.98 | 0.99 | 0.92 | 0.00 | 0.00 | −0.03 |
| Checking | 0.36 | 0.31 | 0.66 | 0.48 | 0.53 | −0.03 | 0.20 | 0.21 | 0.03 | 0.21 | 0.18 | 0.40 |
| Repeating | 0.91 | 0.93 | 0.97 | 0.03 | 0.03 | −0.03 | 0.01 | 0.01 | 0.03 | 0.12 | 0.13 | −0.03 |
| Counting | 0.86 | 0.88 | 0.89 | 0.04 | 0.04 | 0.06 | 0.00 | 0.00 | 0.07 | 0.13 | 0.15 | −0.04 |
| Ordering | 0.92 | 0.95 | 0.87 | 0.00 | 0.00 | −0.02 | −0.01 | 0.00 | 0.02 | 0.17 | 0.18 | 0.06 |
| Hoarding compulsions | 0.22 | 0.24 | 0.01 | 0.01 | 0.01 | 0.00 | 0.00 | 0.00 | 0.04 | 0.97 | 0.96 | 0.99 |
| Percent variance | 26.7% | 26.7% | 28.7% | 21.0% | 21.9% | 16.4% | 15.9% | 15.8% | 19.9% | 15.4% | 15.2% | 16.7% |
Factor Analysis Results for Studies Involving Adults and Children
Factor Analysis Results for Studies Involving English-Speaking and Non-English-Speaking Subjects
Factor Analysis Results for Studies Using Category- Versus Item-Level Symptoms
Factor Analysis Results for Studies Using Current Versus Lifetime Symptoms
Factor Analysis Results for Studies Based on Symptom Scoring
Factor Analysis Results for Studies Based on Rotation Method
Discussion
References
Information & Authors
Information
Published In
History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).