To the Editor: Recognition that not all central nervous system lesions present with obvious signs and symptoms, such as headache or weakness, is imperative in clinical neuroscience. The patient described below reminds us that a detailed history and mental status examination can localize a lesion, even when the rest of the neurological and physical exam is normal.
A 74 year-old right-handed man with a distant history of a resected melanoma and squamous cell carcinoma presented with difficulty manipulating familiar objects. He reported that over recent weeks he had noticed difficulty with previously routine tasks. For instance, he described failing at multiple attempts to attach a drain hose to a faucet; he found himself repeatedly placing the hose on the table, instead. He was fully aware of his error, but unable to perform the desired task. Another example occurred while completing his daily wordsearch puzzle. He found that despite being able to identify the words within the boxes of jumbled letters he could not circle them, encircling letters he did not intend.
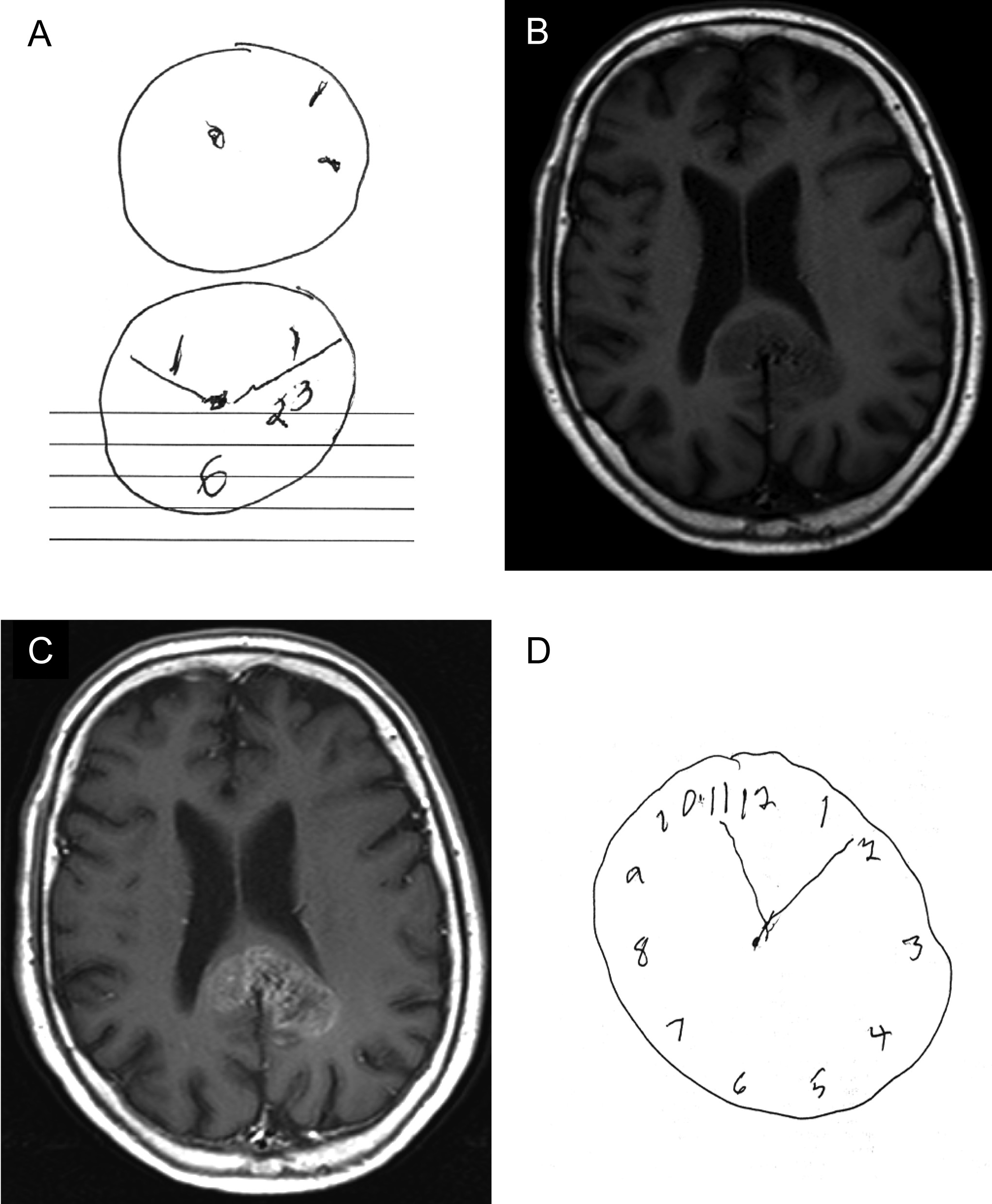
Neurological examination was intact including spatial attention (absence of neglect) and left-right orientation, language, gnosis and orientation. There were no abnormal involuntary movements of the extremities and strength was full throughout. However, as seen in
Figure 1, he failed to complete a clock drawing correctly (panel A: 2 attempts over 4 minutes, provider drew circles) or copy intersecting polygons. Imaging was obtained and an MRI demonstrated a corpus callosum splenial mass with surrounding vasogenic edema (panels B and C). The patient was admitted for further evaluation and given IV methylprednisolone. Within 36 hours of methylprednisolone initiation, his complaints resolved and on repeat testing the clock drawing (panel D: drawn in under 30 seconds, patient drew circle) and intersecting polygons were normal. A brain biopsy was obtained and pathology was consistent with glioblastoma multiforme.
The patient’s symptoms and exam highlight a disconnection syndrome with constructional apraxia. Constructional apraxia is the inability to construct elements in the correct way to form a meaningful whole.
1 It is typically associated with posterior parietal lesions.
2 Constructional apraxia has also been noted in patients with posterior corpus callosum lesions, however it is usually found in conjunction with visuomotor apraxia, alexia and/or dysgraphia.
3, 4 It is likely that the symptoms were the result of tumor associated edema, resolved with methylprednisolone. This demonstrates that repeated neurological testing is sometimes necessary to discern symptoms of a primary tumor from those of the secondary edema. Furthermore, we are reminded that a patient with an intraaxial mass, greater than 3 cm, can have abnormal findings limited to cognitive exam.