To the Editor: Pathologic laughing is associated with brain damage seen in a variety of disorders, which occurs as a result of lesions in various diseases and is often seen associated with prefrontal or brainstem lesions.
1,2 Neuromyelitis optica (NMO) is an uncommon inflammatory disease of the central nervous system characterized by optic neuritis and myelitis, and also develops brain lesions.
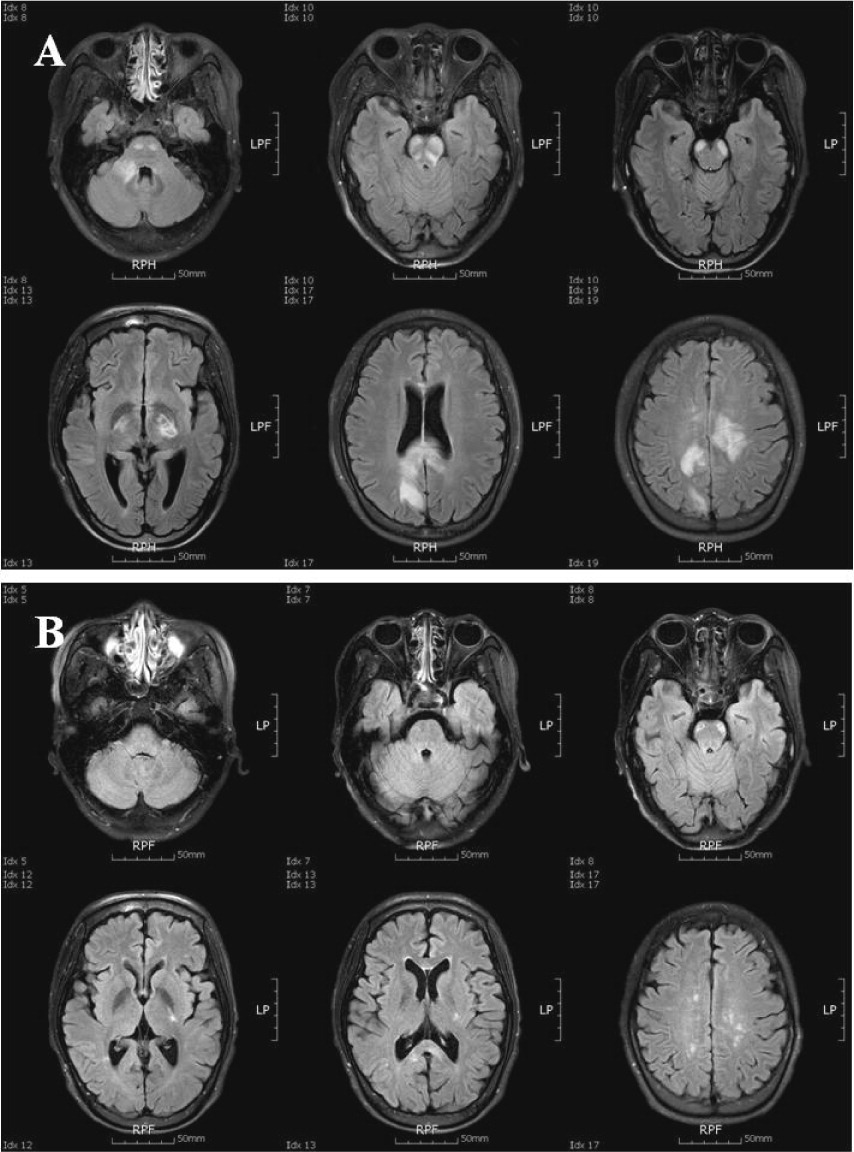
3 We report a young woman with NMO showing the pathologic laughing as an initial manifestation and remarkably improved by plasmapheresis. A 27-year-old woman presented to our hospital with quadriparesis and decreased mentality. In her past medical history, from the time she was 17 years old, she had experienced several episodes of myelitis and optic neuritis, and had been treated with oral steroid and immune-suppressants for NMO. On admission, interestingly, she frequently laughed in response to stimuli that normally would not trigger laughing, which was consistent with pathologic laughing. Brain MRI revealed inflammatory lesions involving internal capsule, corpus callosum, white matters, brainstem, and cerebellar peduncle (
Figure 1, A). CSF analysis revealed increase white blood cell (120) and protein (352.8 mg/dL) without oligoclonal band. In serologic analysis, the antiaquaporin-4 antibody was positive. Initially, the patient was initially treated for consecutive 5 days with a high dose of intravenous methylprednisolone (1 g/day), followed by a high dose of oral prednisolone (60 mg/day). In spite of the high-dose steroid therapy, her neurological symptoms did not improve. For further treatment, she was alternately treated with seven courses of plasmapheresis for 14 days. Treatment of plasmapheresis showed remarkable improvement in motor power, mentality, and severity and occurrence of pathologic laughing. The MRI scan taken 2 months later showed regression of the initial inflammatory lesions (
Figure 1, B). According to numerous reports, the discovery of a specific autoantibody against aquaporin-4 (AQP4), clinical and experimental evidence has shown that NMO has a humoral immune mechanism and brain lesions in NMO are preferentially observed in regions where AQP4 is abundantly present, such as the bilateral diencephalic regions adjacent to the third ventricles, the pontine tegmentum and cerebellum surrounding the fourth ventricles, and the periventricular white matter adjacent to the lateral ventricles.
3,4 Our NMO patient also showed characteristic brain lesions of NMO and pathologic laughing. The pathophysiology of the pathological laughing has been described as the dysfunction in the cerebro-pontocerebellar circuits that involve the pontine base in brainstem nuclei and the cerebellum, which is consistent with the inflammatory lesion in our patient.
1,2 Previously, in the multiple sclerosis (MS), the pathologic laughing have been described and steroid pulse therapy was effective for pathological laughing.
5 In contrast with MS, our NMO patient showed improvement of the pathologic laughing only after treatment by plasmapheresis. In this case, the patient’s motor weakness and pathologic laughing did not improve in spite of consecutive high dose-corticosteroid for 2 weeks, but remarkably improved after plasmapheresis therapy. Our finding on the effectiveness of the plasmapheresis therapy is very significant, because the pathologic laughing of the patient with NMO will be properly treated with the plasmapheresis, instead of conventional treatments of high-dose steroid.