Catatonia is a neuropsychiatric syndrome that is associated with many general medical and psychiatric conditions.
1–3 Catatonia was historically described in persons in depressive and manic states, but throughout the 20th century it became linked with schizophrenia.
4 More recent studies clarified catatonia’s link to affective disorders in a majority of cases, and called attention to the fact that between 21% and 46% of cases are secondary to an underlying general medical condition (GMC).
2,5,6Current psychiatric nosology reflects this history. The DSM-5 differentiates between catatonia due to a mental disorder and catatonia due to another GMC, although it still classifies catatonia in the chapter of psychotic disorders.
7 The label of unspecified catatonia refers to cases where the cause is unknown (i.e., idiopathic) or the required number of catatonic signs is not met.
7The prevalence of catatonia due to a GMC is not clearly defined. One retrospective review of 95 patients diagnosed with catatonia
2 identified the prevalence of catatonia due to GMC, psychotic disorder, or mood disorder to be 21%, 23% and 56%, respectively. A prospective study of older patients in a general hospital found catatonia to be present in 8.9% of those evaluated by the psychiatry consultation team.
8 Catatonia has also been described in 3.8% of cases in the intensive care unit (ICU),
9 with all cases attributed to a GMC.
10 Overall, the distribution of underlying causes of catatonia varies based on care setting (psychiatric hospital, general hospital, ICU) and the degree to which a diagnostic workup was undertaken.
11Many general medical etiologies of catatonia are identified in the literature,
1,3,12 and are diagnosable with commonly available tests. A variety of neurologic insults causing catatonia has been reported including stroke, neoplasms, hydrocephalus, hemorrhages, neurodegenerative and autoimmune conditions, as well as posterior reversible encephalopathy syndrome, all of which can be identified with neuroimaging.
1–3,13,14 The utility of electroencephalography (EEG) in catatonia is widely acknowledged, particularly to exclude seizures and nonconvulsive status epilepticus.
15 Even in cases of catatonia attributed to psychiatric conditions, EEGs are abnormal in more than 50% of cases.
2,16 Deficiencies of vitamin B12
17–19and folate
20 have been linked to catatonia. Hypo- and hyperthyroidism have been reported to cause catatonia, and treatment with thyroid hormone or antithyroid drugs may reverse the catatonic states.
21,22 Additionally, catatonia has been linked to other endocrinopathies, infections, drug intoxication or withdrawal states, lithium or tacrolimus intoxication, among other causes.
3,23–25 Data from case series show that catatonic signs exist in up to 88% of patients with anti-
N-methyl-D-aspartate receptor (aNMDAR) encephalitis, a condition diagnosed through analysis of cerebrospinal fluid.
26Recent studies have shown that catatonia is frequent in patients with delirium,
27,28 a condition for which further diagnostic workup may be indicated. Cocaine or stimulant intoxication, alcohol withdrawal, traumatic brain injury and manic states can present with both delirium and catatonic features.
29,30 Despite these observations, DSM-5 nosology precludes the diagnosis of catatonia due to GMC if it occurs exclusively in the course of delirium.
Given the lengthy differential diagnosis, clinicians are faced with a difficult task when evaluating a patient with catatonic signs. Expert recommendations for a rational diagnostic approach to catatonia exist,
9,14,31,32 and include laboratory studies, neuroimaging, and EEG, and more extensive workup based on clinical suspicion. Some authors recommend lumbar puncture in all cases,
33 and others have advocated for an extensive workup to rule out general medical etiologies before attributing the cause of catatonia to a psychiatric disorder.
12 The lack of systematic data on the rates of general medical etiologies of catatonia makes generating evidence-based workup recommendations difficult. While studies have reported the range of causes of catatonia, none have systematically applied a standardized diagnostic workup so that the pretest probability of abnormal findings for each test could be known. Currently, there is no accepted standard for ruling out GMCs as the etiology of catatonia, or ruling in a psychiatric etiology.
A methodical diagnostic approach to catatonia is important because effective treatment for catatonia begins with correcting the underlying cause. Treating the catatonic state itself is essential to prevent further complications, including dehydration, malnutrition, exhaustion, injuries, acute renal failure, deep venous thrombosis, pulmonary embolism and pressure ulcers.
34 In general, lorazepam and electroconvulsive therapy (ECT) are highly effective in treating catatonia regardless of its underlying etiology,
35,36 although there is some evidence suggesting that ECT may be less effective or have increased risk of side effects in some neurological conditions.
37,38 These risks may be lowered through careful pre-ECT evaluation and optimal ECT technique.
39The aim of this study was to describe the diagnostic evaluations completed in cases of catatonia in one general medical hospital and the clinical factors associated with greater diagnostic evaluations, likelihood of receiving treatment, and response to treatment. Our hypotheses included: 1) Cases of catatonia attributed to a psychiatric disorder receive less diagnostic workup than cases attributed to a GMC; 2) Catatonia due to GMC is commonly associated with suspected delirium; and 3) Improvement with lorazepam occurs in catatonia regardless of the underlying etiology.
Methods
With approval from the Institutional Review Board at the University of Chicago, we performed a retrospective chart review of adult general hospital inpatients at the University of Chicago Medical Center from January 2011 to December 2013. No psychiatric inpatients were included. Cases were identified by searching medical records for the words “catatonia” or “catatonic” in provider notes. Charts were then screened to clarify which cases had been diagnosed with catatonia. Only cases that had documented evidence of catatonia during the hospitalization were included. Demographic and clinical data, including diagnostics and treatment, were extracted from all cases that met inclusion criteria.
To be included in the study, a consensus opinion of all reviewers regarding catatonic signs and etiological factors was required. All reviewers used the same chart review instructions to classify cases. Confirmed cases of catatonia were classified by reviewers into three etiological groups following DSM-5 criteria: catatonia due to GMC, catatonia due to a psychiatric disorder, or unspecified catatonia. Cases meeting criteria for catatonia due to a GMC with suspected co-occurring delirium were included. The treating clinicians may have used DSM-IV, DSM-5, or other criteria for making the clinical diagnosis of catatonia, but only those meeting retrospective DSM-5 criteria, modified as above, were included in the sample.
Statistical Analysis
All analyses were conducted using SAS software, Version 9.3 (SAS Institute, Cary, N.C.). For our primary research question, each diagnostic test was coded as a binary variable, with 1=test ordered and 0=no test ordered. Pearson correlations were used to describe intercorrelations among tests. The number of individual tests was then summed to create a total number of tests ordered, ranging from a possible 0 to 17. The continuous summary variable was normally distributed (median=8.00, mean=7.59, SD=3.24, range=3–14, skewness=0.12). A series of regression analyses examined factors that predicted the total number of tests ordered, including age, gender (0=male, 1=female), binary variables for first episode of catatonia, past history of other psychiatric illness, suspected delirium, and dopamine D2 receptor antagonist exposure, as well as the total number of catatonic symptoms (as a continuous measure). To examine factors associated with treatment, the use of lorazepam was coded as a 0=no and 1=yes, and logistic regression analysis was used to predict the likelihood of treatment, using the same factors as above. For examination of group differences, such as differences in treatment response rates across groups, results from simple chi-square tests for binary data and t tests for continuous measures are reported. Given the large number of individual diagnostic tests, any post hoc comparisons of group differences in diagnostic tests were conducted using a conservative p<0.01 threshold.
Results
Sample
A total of 170 charts were identified and reviewed, and 54 cases were diagnosed as catatonia and included in our analysis. They included 36 female adults and 18 male adults aged 18–80 (median age=53.50 years). Most cases (N=43, 79.63%) were African American. All cases represent unique patients except one patient with schizophrenia with three distinct presentations, a different patient with schizophrenia who presented twice, and one patient with hyponatremia who presented twice.
Descriptive Information
Table 1 shows the clinical features of the sample. Most cases presented with a first-known episode of catatonia. Approximately 40% of the sample had a past history of other psychiatric illness and/or a family history of psychiatric illness. Just over half of cases had suspected delirium. Catatonia was preceded by dopamine D2 receptor antagonist exposure in nearly 60% of cases. In this sample, dopamine D2 receptor antagonists to which patients were exposed included (alone or in combination) haloperidol, fluphenazine, risperidone, olanzapine, ziprasidone, metoclopramide, quetiapine, and clozapine. The average number of DSM-5 clinical symptoms in this sample was 4.39 (SD=1.50; range=3–9).
Diagnostic Workup and Results
Table 2 describes the diagnostic tests obtained for this sample. The average number of tests obtained was 7.59 (SD=3.24) and ranged from 3 to 14. No case received all 17 tests. The use of urine drug screens was inversely related to the use of other medical tests, and these negative correlations were significant for tests of liver function, thyrotropin, B12, folate, iron levels, and EEG. In general, intercorrelations between the other 16 tests were positive and significant. Exceptions were CBC, creatine kinase (which was only correlated with liver function), and the four tests that were ordered among fewer than 10 cases (paraneoplastic panel, lithium level, aNMDAR antibodies, and tacrolimus level).
In univariate models, older age (b=0.08, SE=0.02, t52=3.53, p<0.001), first episode of catatonia (b=3.52, SE=1.45, t52=2.42, p=0.019), and suspected delirium (b=5.35, SE=0.49, t52=10.81, p<0.001) were all associated with a greater number of tests. There was no association between total number of tests with gender (b=−0.44, SE=0.94, t52=–0.47, p=0.639), past history of psychiatric illness (b=−1.09, SE=0.89, t52=–1.23, p=0.225), dopamine D2 receptor antagonist exposure (b=0.85, SE=0.90, t52=0.94, p=0.350), or total number of catatonia symptoms (b=−0.11, SE=0.30, t52=–0.38, p=0.707). In a multiple regression, only suspected delirium remained significant (b=5.14, SE=0.73, t46=7.08, p<0.001). The average number of tests obtained for cases with suspected delirium (N=29, mean=10.07, SD=1.91) was more than double the number of tests ordered for cases without suspected delirium (N=25, mean=4.72, SD=1.70). In addition, only two cases without suspected delirium received more than seven tests. In contrast, all but one case with suspected delirium received eight or more tests.
Post hoc chi-square statistics for individual tests (excluding BMP and CBC) revealed significantly higher rates of tests (p<0.010) among cases with suspected delirium for all tests except paraneoplastic panel (p=0.069), lithium level (p=0.767), aNMDAR antibodies (p=0.029), and tacrolimus level (p=0.098). The only test more likely to be obtained in cases without suspected delirium was urine drug screening (34% versus 80%, p<0.001).
Table 3 characterizes the abnormal results across all cases of catatonia.
Table 4 lists the abnormalities found on EEG and imaging. Overall, test results led to a diagnosis of GMC etiology for 29 cases. Twenty cases were attributed to a psychiatric condition, and five cases could not be assigned either a GMC or a psychiatric etiology. Cases assigned a psychiatric etiology received significantly fewer diagnostic tests (mean=5.00, SD=2.20) compared with cases with a GMC etiology (mean=9.07, SD=2.67, t
51=3.40, p=0.001) and to cases with unknown etiology (mean=9.40, SD=3.51, t
51=5.41, p<0.001). However, cases with a psychiatric etiology were also significantly less likely to have suspected delirium (10.00% psychiatric; 79.31% GMC; 80.00% unknown etiology; χ
2=24.40, df=2, p<0.001).
Table 5 lists the general medical and psychiatric etiologies of catatonia. Thirty-two cases were preceded by administration of dopamine D2 receptor antagonist exposure, including three that received metoclopramide. In only one case was the dopamine D2 receptor antagonist regarded as the sole etiology, a case of haloperidol-induced neuroleptic malignant syndrome (NMS).
Treatment Effects
There were no cases where ECT was recommended or used as a treatment. Lorazepam was administered during the catatonic episode in 29 (53.70%) cases. One additional case received and responded to clonazepam but was not included in the analyses. There were no differences in rates of administration of lorazepam between the GMC (17/28; 60.71%), psychiatric (10/20; 50.00%), and unknown etiology (2/5; 40.00%) groups (χ2=1.02, df=2, p=0.600) or between cases of suspected delirium (17/29; 58.62%) or not (12/24; 50.00%) (χ2=0.39, df=1, p=0.530). Additional multiple logistic regression revealed that only the total number of catatonic symptoms was associated with likelihood of receiving lorazepam (odds ratio=1.84; 95% CI: 1.10—3.09, p=0.021). Age, gender, first episode of catatonia, history of other psychiatric illness, dopamine D2 receptor antagonist exposure, and suspected delirium were not associated with likelihood of receiving lorazepam (all p values >0.100).
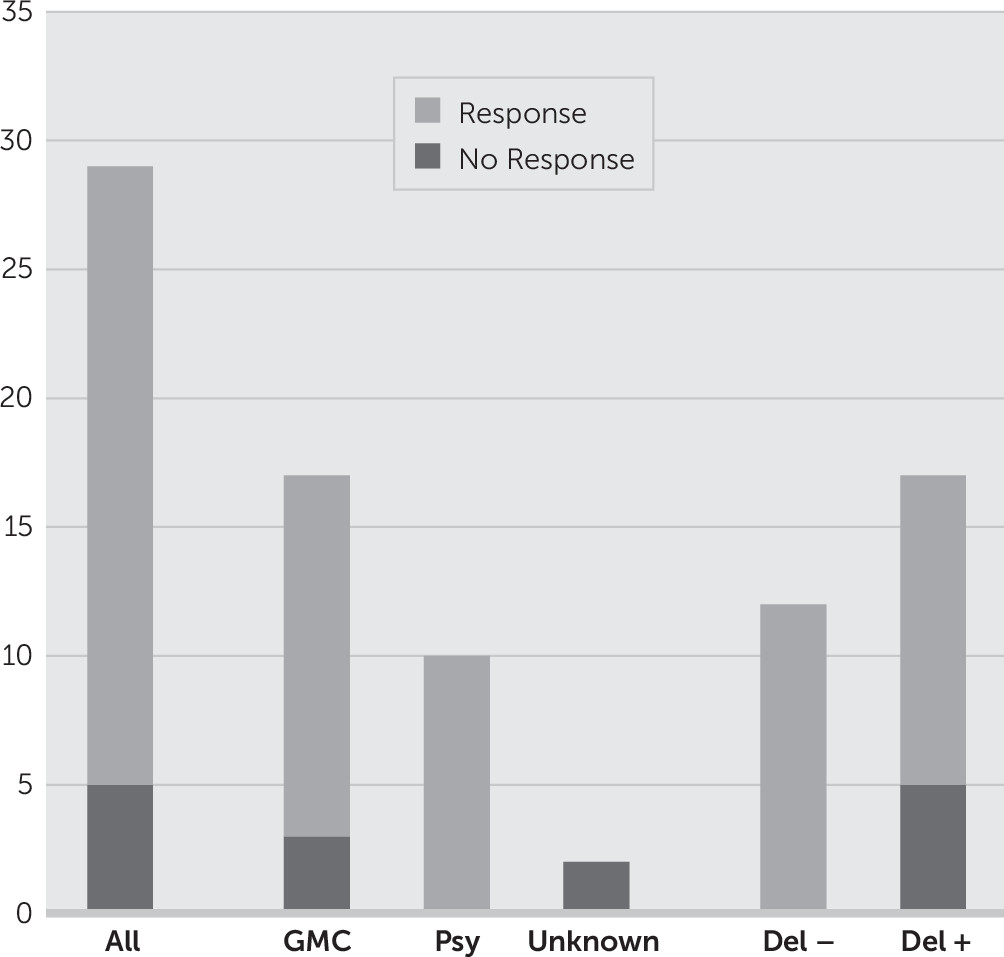
Of the 29 cases that received lorazepam, the majority (24; 82.76%) responded to treatment (
Figure 1). There was no difference in treatment response between cases with a GMC etiology (14/17; 82.35%) and cases with a psychiatric etiology (10/10; 100.00%; χ
2=1.99, df=1, p=0.159); however, neither of the cases with unknown etiology (0/2) responded to treatment (χ
2=11.69, df=2, p=0.003). Cases with suspected delirium were less likely to respond to lorazepam (12/17; 70.59%) than cases without suspected delirium (12/12; 100.00%; χ
2=4.26, df=1, p=0.039).
Discussion
The results from this study demonstrate an association between the clinical suspicion of delirium and an increased search for general medical conditions in catatonia.
Cases of catatonia attributed to psychiatric etiologies had delirium suspected rarely, and received significantly less diagnostic workup. The term delirium implies a general medical etiology, whereas catatonia may not carry that association for many clinicians. This finding raises the question about whether the determination of a psychiatric etiology for catatonia was made in the absence of a complete diagnostic workup excluding other general medical causes, or whether a more limited diagnostic workup was clinically appropriate given the history and examination. Our retrospective design does not allow us to clarify if a more thorough workup would have uncovered GMC etiologies in the cases of catatonia attributed to psychiatric conditions. There may be additional factors not captured by our study design, such as additional general medical comorbidities, which could have influenced the clinical decision to obtain more or less workup. Urine drug screen was the only test inversely related to suspicion of delirium, which was likely related to the fact that in our hospital patients require a urine drug screen prior to psychiatric hospitalization.
The tests that were more useful in identifying a GMC in our sample were complete blood count (leukocytosis), basic metabolic panel (hyponatremia, uremia), CSF analysis, urine drug screening, serum lithium level, and EEG. The completion of these six tests detected the underlying cause in 24 out of 29 cases of cases with catatonia due to GMC (83%). Many of the abnormalities seen may be a result of the catatonic state rather than the etiology. When neuroimaging and EEG were done, abnormal results were frequently identified, consistent with previous studies on catatonia.
2,16,40 Most of the imaging and EEG abnormalities were considered nonspecific. For instance, small vessel disease (SVD) was found in 17 of 40 cases with imaging, and was significantly associated with age (mean age with SVD 65.2 years versus 45.9 years without SVD, p<0.001), but SVD was not implicated as the cause of catatonia in any cases. Overall, nearly all of the GMC etiologies in our series are conditions amenable to or fully reversible with treatment (
Table 5). The high rates of detecting a GMC in catatonia seen in our series highlight the need for a thorough evaluation in all catatonic patients to exclude a general medical etiology, particularly in the general hospital.
In just over half of the cases in our sample, clinical teams raised suspicion for delirium. Prior studies of catatonia have excluded patients with delirium,
2 which is consistent with DSM-IV and DSM-5 criteria. However, other studies show that delirium and catatonia can co-occur.
27–30 Thus, we did not exclude delirium from our sample. We propose that this exclusion criterion is difficult to operationalize in clinical practice, particularly in catatonia secondary to GMCs. Our data support the idea that delirium comorbid with catatonia may drive clinical reasoning, and thus this relationship warrants further study.
The majority of cases (82%) that documented the effects of lorazepam demonstrated at least some benefit. It is noteworthy that lorazepam was useful in 100% of cases without suspected delirium. Even in suspected delirium, a response rate of 71% to lorazepam indicates a treatment worthy of consideration. Moreover, treatment with lorazepam was related to the total number of catatonic signs present, which is a marker of possible severity, and not related to the suspicion of delirium. Since lorazepam may worsen delirium, these data support the idea that catatonia may often supersede delirium in the consideration of treatment options. Our retrospective data cannot adequately test this hypothesis. A recent case series study found that ECT was an effective treatment for 5 patients with persistent delirium in the ICU, at least one of whom was catatonic.
41 However, our study did not use a standardized method to detect or rule out delirium and cases with documented suspected delirium may not have had that diagnosis.
The main limitation of our study is its retrospective design which 1) prevented the use of validated instruments for diagnosing catatonia or delirium; 2) creates a bias whereby clinicians may have documented differently in cases of catatonia or where the cases received the workup that was felt necessary by the clinical team based on the history and exam; and 3) means that unaccounted for differences between the groups may have influenced the results. Notwithstanding these limitations, our sample represents the clinical decision making related to presentations of catatonia in one general hospital setting.
Conclusions
Our findings reflect the variation in diagnostic evaluation of catatonia that has been previously described, and indicate that suspicion of comorbid delirium may drive a significant portion of this variation. Future studies are needed to prospectively workup all cases of catatonia in a standardized manner, regardless of suspected etiology, to help determine the rates of general medical etiologies of catatonia. Such data can help guide clinicians to adequately exclude general medical causes, or identify which clinical factors should trigger additional workup, before making a determination of a psychiatric etiology.
The comorbidity between catatonia, particularly catatonia due to a GMC, and delirium is an important but inadequately understood clinical phenomena. The DSM-5 criteria for catatonia might be insufficient regarding diagnosis in cases of co-occurring delirium and catatonia. Further studies are needed to investigate the safety and utility of treatments for catatonia, such as benzodiazepines and ECT, in these patients.
Acknowledgments
The authors thank Paige Marnell and Anya Piotrowski for their contributions to the research.