Predicting New-Onset Psychiatric Disorders Throughout the COVID-19 Pandemic: A Machine Learning Approach
Abstract
Objective:
Methods:
Results:
Conclusions:
Methods
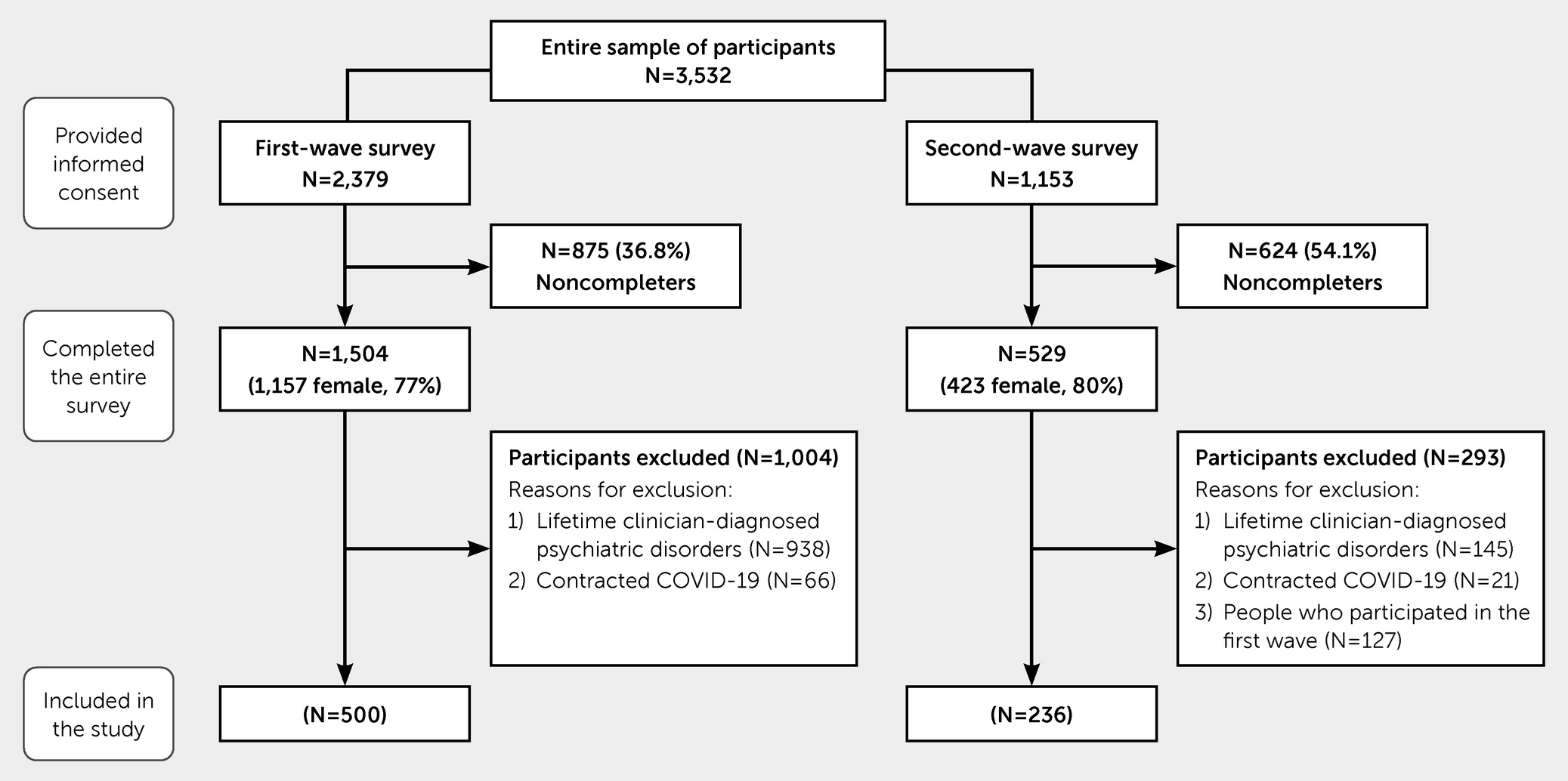
Procedures
Participants
Measures
Patient Health Questionnaire (PHQ).
PTSD Checklist for DSM-5 (PCL-5).
Brief Resilience Scale (BRS).
ML Methodology
| First wave (N=500) ≥1 new-onset PPsyDs | Second wave (N=236) ≥1 new-onset PPsyDs | |||||||
|---|---|---|---|---|---|---|---|---|
| Yes (N=80, 16.0%) | No (N=420, 84%) | Yes (N=44, 18.6%) | No (N=192, 81.4%) | |||||
| Characteristic | N | % | N | % | N | % | N | % |
| Female | 59 | 73.7 | 287 | 68.3 | 35 | 79.5 | 150 | 78.1 |
| Age (mean±SD years) | 37.1 | 14.7 | 47.0 | 15.9 | 31 | 12.4 | 39.2 | 15.0 |
| Education (mean±SD years) | 15.2 | 3.6 | 15.5 | 3.4 | 14.8 | 2.7 | 15.3 | 3.3 |
| Marital status | ||||||||
| Unmarried | 48 | 60.0 | 157 | 37.4 | 33 | 75.0 | 95 | 49.5 |
| Married, common-law, civil union | 27 | 33.8 | 219 | 52.1 | 9 | 20.5 | 81 | 42.2 |
| Separated, divorced, widowed | 5 | 6.3 | 44 | 10.5 | 2 | 4.5 | 16 | 8.3 |
| Living alone (yes) | 12 | 15.0 | 54 | 12.9 | 1 | 2.3 | 15 | 7.8 |
| Number of children | ||||||||
| 0 | 56 | 70.0 | 211 | 50.2 | 34 | 77.3 | 116 | 60.4 |
| 1 | 10 | 12.5 | 104 | 24.8 | 5.0 | 11.4 | 29 | 15.1 |
| >1 | 14 | 17.5 | 105 | 25.0 | 5.0 | 11.4 | 47 | 24.5 |
| Perceived changes in difficulty in looking after children during the pandemic, compared with prepandemic | ||||||||
| Decreased | 2 | 2.5 | 22 | 5.2 | 1 | 2.3 | 6 | 3.1 |
| Remained similar | 6 | 7.5 | 126 | 30.0 | 2 | 4.5 | 40 | 20.1 |
| Increased | 16 | 20.0 | 61 | 14.5 | 7 | 15.9 | 30 | 15.6 |
| Perceived changes in quality of relationship with children during the pandemic, compared with prepandemic | ||||||||
| Improved | 3 | 3.8 | 42 | 10.0 | 1 | 2.3 | 7 | 3.6 |
| Remained similar | 16 | 20.0 | 158 | 37.6 | 7 | 15.9 | 67 | 34.9 |
| Worsened | 5 | 6.3 | 9 | 2.1 | 2 | 4.5 | 2 | 1.0 |
| Employment status | ||||||||
| Unemployed | 3 | 3.8 | 22 | 5.2 | 4 | 9.1 | 4 | 2.1 |
| Retired | 8 | 10.0 | 62 | 14.8 | 1 | 2.3 | 16 | 8.3 |
| Employed | 26 | 32.5 | 174 | 41.4 | 4 | 9.1 | 67 | 34.9 |
| Self-employed | 13 | 16.3 | 92 | 21.9 | 7 | 15.9 | 44 | 22.9 |
| Homemaker | 3 | 3.8 | 17 | 4.0 | 1 | 2.3 | 5 | 2.6 |
| Student (all undergraduate, attending university) | 27 | 33.8 | 53 | 12.6 | 27 | 61.4 | 56 | 29.2 |
| Cause of unemployment | ||||||||
| Due to the pandemic | 0 | 0.0 | 4 | 1.0 | 1 | 2.3 | 1 | 0.5 |
| Preceding the pandemic | 3 | 3.8 | 18 | 4.6 | 3 | 6.8 | 3 | 1.6 |
| Other pandemic-related changes in employment status | ||||||||
| Job changed, compared with previous employment | 0 | 0.0 | 2 | 0.5 | 1 | 2.3 | 0 | 0.0 |
| Previous unemployment that turned into employment | 0 | 0.0 | 1 | 0.2 | 1 | 2.3 | 0 | 0.0 |
| Pandemic-related changes in the workplace | ||||||||
| Continued to work only at one’s own workplace | 4 | 5.3 | 36 | 9.0 | 3 | 7.1 | 62 | 32.8 |
| Worked only remotely | 28 | 36.8 | 151 | 37.9 | 2 | 4.5 | 18 | 9.5 |
| Worked in part at one’s own workplace and in part remotely | 3 | 3.9 | 57 | 14.3 | 4 | 9.1 | 28 | 14.8 |
| Pandemic-related changes in job position (yes) | 0 | 0.0 | 10 | 2.5 | 1 | 2.3 | 8 | 4.2 |
| Pandemic-related changes in work hours, compared with prepandemic | ||||||||
| Increased | 19 | 25.0 | 80 | 20.1 | 2 | 4.5 | 18 | 9.5 |
| Remained similar | 8 | 10.5 | 98 | 24.6 | 7 | 15.9 | 72 | 38.1 |
| Decreased | 8 | 10.5 | 66 | 16.6 | 0 | 0.0 | 18 | 9.5 |
| Pandemic-related changes in work shifts, compared with prepandemic | ||||||||
| Increased | 2 | 2.6 | 16 | 4.0 | 0 | 0.0 | 2 | 1.1 |
| Remained similar | 4 | 5.3 | 43 | 10.8 | 3 | 6.8 | 36 | 19.0 |
| Decreased | 2 | 2.6 | 17 | 4.3 | 0 | 0.0 | 6 | 3.2 |
| Perceived changes in work performance during the pandemic, compared with prepandemic | ||||||||
| Increased | 10 | 13.2 | 61 | 15.3 | 0 | 0.0 | 15 | 7.9 |
| Remained similar | 14 | 18.4 | 129 | 32.4 | 5 | 11.9 | 73 | 38.6 |
| Decreased | 11 | 14.5 | 64 | 13.6 | 4 | 9.5 | 20 | 10.6 |
| Perceived changes in work exertion during the pandemic, compared with prepandemic | ||||||||
| Increased | 23 | 30.3 | 111 | 27.9 | 6 | 14.3 | 51 | 27.0 |
| Remained similar | 6 | 7.9 | 103 | 25.9 | 3 | 7.1 | 51 | 27.0 |
| Decreased | 6 | 7.9 | 30 | 7.5 | 0 | 0.0 | 6 | 3.2 |
| Adequate procedures for preventing the COVID-19 infection put in place in the workplace (judgment of participant) | ||||||||
| Not at all | 0 | 0.0 | 3 | 0.8 | 0 | 0.0 | 2 | 1.1 |
| A little | 5 | 6.6 | 21 | 5.3 | 1 | 2.5 | 8 | 4.6 |
| Significantly | 0 | 0.0 | 28 | 7.0 | 0 | 0.0 | 27 | 15.4 |
| A lot | 2 | 2.6 | 49 | 12.3 | 3 | 7.5 | 29 | 16.6 |
| Very much | 5 | 6.6 | 32 | 8.0 | 3 | 7.5 | 16 | 9.1 |
| One’s own economic status during the pandemic (judgment of participant) | ||||||||
| Improved slightly or significantly | 6 | 7.5 | 41 | 9.8 | 1 | 2.3 | 14 | 7.3 |
| Remained stable | 51 | 63.8 | 246 | 58.6 | 26 | 59.1 | 119 | 62.0 |
| Worsened slightly | 16 | 20.0 | 102 | 24.3 | 13 | 29.5 | 47 | 24.5 |
| Worsened significantly or very much | 7 | 8.8 | 31 | 7.4 | 4 | 9.1 | 12 | 6.3 |
| First wave (N=500) ≥1 new-onset PPsyDs | Second wave (N=236) ≥1 new-onset PPsyDs | |||||||
|---|---|---|---|---|---|---|---|---|
| Yes (N=80, 16.0%) | No (N=420, 84%) | Yes (N=44, 18.6%) | No (N=192, 81.4%) | |||||
| Characteristic | N | % | N | % | N | % | N | % |
| Clinician-diagnosed current medical conditionsb | 34 | 42.5 | 182 | 43.3 | 15 | 34.1 | 56 | 29.2 |
| N of clinician-diagnosed current medical conditions | ||||||||
| 1 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| 2 | 22 | 27.5 | 132 | 31.4 | 11 | 25.0 | 47 | 24.5 |
| 3 | 9 | 11.3 | 37 | 8.8 | 4 | 9.1 | 7 | 3.6 |
| 4 | 2 | 2.5 | 15 | 3.6 | 0 | 0.0 | 3 | 1.6 |
| 5 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| 6 | 1 | 1.3 | 0 | 0.0 | 0 | 0.0 | 0 | 0.0 |
| Using current medications for medical conditions | 25 | 31.3 | 156 | 37.1 | 11 | 25.0 | 46 | 24.0 |
| Smoking habit during the pandemic | ||||||||
| Continued not smoking | 64 | 80.0 | 351 | 83.6 | 27 | 69.2 | 148 | 79.6 |
| Continued or started smoking | 14 | 17.5 | 61 | 14.5 | 11 | 28.2 | 33 | 17.7 |
| Quit smoking | 2 | 2.5 | 8 | 1.9 | 1 | 2.6 | 5 | 2.7 |
| Alcohol use during the pandemic | ||||||||
| Continued not drinking | 31 | 38.8 | 156 | 37.1 | 8 | 20.5 | 65 | 34.9 |
| Continued or started drinking | 46 | 57.5 | 255 | 60.7 | 31 | 79.5 | 119 | 64.0 |
| Quit drinking | 3 | 3.8 | 9 | 2.1 | 0 | 0.0 | 2 | 1.1 |
| Recreational drug use during the pandemicc | ||||||||
| Continued not using | 74 | 92.5 | 411 | 97.9 | 34 | 87.2 | 177 | 95.2 |
| Continued or started using | 4 | 5.0 | 5 | 1.2 | 4 | 10.3 | 8 | 4.3 |
| Quit using | 2 | 2.5 | 4 | 1.0 | 1 | 2.6 | 1 | 0.5 |
| Practicing physical activity during the pandemic | ||||||||
| Continued not practicing | 18 | 22.5 | 72 | 17.1 | 11 | 28.2 | 44 | 23.7 |
| Continued or started practicing | 49 | 61.3 | 326 | 77.6 | 27 | 69.2 | 138 | 74.2 |
| Quit practicing | 13 | 16.3 | 22 | 5.2 | 1 | 2.6 | 4 | 2.2 |
| Satisfaction with usual sleep before the pandemic | ||||||||
| Very satisfied | 9 | 13.3 | 42 | 10.0 | 5 | 12.8 | 27 | 14.5 |
| Satisfied | 11 | 13.8 | 151 | 36.0 | 7 | 17.9 | 55 | 29.6 |
| Neutral | 15 | 18.8 | 74 | 17.6 | 7 | 17.9 | 34 | 18.3 |
| Not very satisfied | 25 | 31.3 | 130 | 31.0 | 14 | 35.9 | 58 | 31.1 |
| Very dissatisfied | 20 | 46.5 | 23 | 53.5 | 6 | 15.4 | 12 | 6.5 |
| Experienced fiduciary isolation or quarantine due to COVID-19–related risk conditionsd | 7 | 9.0 | 24 | 5.9 | 9 | 20.5 | 22 | 11.5 |
| Experienced a loved one's hospitalization due to COVID-19 | 27 | 33.8 | 147 | 35.0 | 11 | 25.0 | 46 | 24.0 |
| Experienced a loved one's death due to COVID-19 | 4 | 5.0 | 38 | 9.0 | 4 | 9.1 | 12 | 6.3 |
| Being scared of transmitting COVID-19 to others | ||||||||
| Not at all | 11 | 13.8 | 99 | 23.6 | 5 | 11.4 | 19 | 10.0 |
| A little | 15 | 18.8 | 163 | 38.8 | 19 | 43.2 | 85 | 44.7 |
| Significantly | 17 | 21.3 | 104 | 24.8 | 11 | 25.0 | 46 | 24.2 |
| A lot | 21 | 26.3 | 36 | 8.6 | 4 | 9.1 | 29 | 15.3 |
| Very much | 16 | 20.0 | 18 | 4.3 | 5 | 11.4 | 11 | 5.8 |
| Being stressed by pandemic-related restrictions on activities and personal movement | ||||||||
| Not at all | 3 | 3.8 | 85 | 20.2 | 10 | 22.7 | 53 | 27.6 |
| A little | 19 | 23.8 | 179 | 42.6 | 18 | 40.9 | 106 | 55.2 |
| Significantly | 26 | 32.5 | 102 | 24.3 | 7 | 15.9 | 18 | 9.4 |
| A lot | 21 | 26.3 | 41 | 9.8 | 3 | 6.8 | 11 | 5.7 |
| Very much | 11 | 13.8 | 13 | 3.2 | 6 | 13.6 | 4 | 2.1 |
| History of trauma before the COVID-19 pandemic (yes) | 20 | 25.0 | 83 | 19.8 | 6 | 13.6 | 29 | 15.1 |
| Distribution of new-onset PPsyDse | ||||||||
| Major depressive disorder | 40 | 8.0 | — | — | 18 | 7.6 | — | — |
| Any anxiety disorder | 56 | 11.2 | — | — | 27 | 11.4 | — | — |
| Panic disorder | 6 | 1.2 | — | — | 7 | 3.0 | — | — |
| Obsessive-compulsive disorder | 31 | 6.2 | — | — | 9 | 3.8 | — | — |
| Posttraumatic stress disorder | 10 | 2.0 | — | — | 8 | 3.4 | — | — |
| First wave (N=500) ≥1 new-onset PPsyDs | Second wave (N=236) ≥1 new-onset PPsyDs | |||||||
|---|---|---|---|---|---|---|---|---|
| Yes (N=80, 16.0%) | No (N=420, 84%) | Yes (N=44, 18.6%) | No (N=192, 81.4%) | |||||
| BRS item | N | % | N | % | N | % | N | % |
| Item 1: I tend to bounce back quickly after hard times | ||||||||
| Strongly disagree | 8 | 10.0 | 6 | 1.4 | 5 | 11.4 | 3 | 1.6 |
| Disagree | 16 | 20.0 | 39 | 9.3 | 10 | 22.7 | 21 | 10.9 |
| Neutral | 19 | 23.8 | 81 | 19.3 | 10 | 22.7 | 38 | 19.8 |
| Agree | 28 | 35.0 | 225 | 53.6 | 16 | 36.4 | 106 | 55.2 |
| Strongly agree | 9 | 11.3 | 69 | 16.4 | 3 | 6.8 | 24 | 12.5 |
| Item 2: I have a hard time making it through stressful events | ||||||||
| Strongly disagree | 11 | 13.8 | 82 | 19.5 | 4 | 9.3 | 28 | 14.8 |
| Disagree | 17 | 21.3 | 192 | 45.7 | 15 | 34.9 | 92 | 48.7 |
| Neutral | 19 | 23.8 | 86 | 20.5 | 9 | 20.9 | 39 | 20.6 |
| Agree | 29 | 36.3 | 56 | 13.3 | 12 | 27.9 | 27 | 14.3 |
| Strongly agree | 4 | 5.0 | 4 | 1 | 3 | 7.0 | 3 | 1.6 |
| Item 3: It does not take me long to recover from a stressful event | ||||||||
| Strongly disagree | 6 | 7.5 | 7 | 1.7 | 4 | 9.3 | 3 | 1.6 |
| Disagree | 26 | 32.5 | 48 | 11.4 | 15 | 34.9 | 32 | 16.9 |
| Neutral | 21 | 26.3 | 89 | 21.2 | 9 | 20.9 | 35 | 18.5 |
| Agree | 22 | 27.5 | 220 | 52.4 | 13 | 30.2 | 101 | 53.4 |
| Strongly agree | 5 | 6.3 | 56 | 13.3 | 2 | 4.7 | 18 | 9.5 |
| Item 4: It is hard for me to snap back when something bad happens | ||||||||
| Strongly disagree | 8 | 10.0 | 83 | 19.8 | 5 | 11.6 | 21 | 11.1 |
| Disagree | 25 | 31.3 | 188 | 44.8 | 13 | 30.2 | 91 | 48.1 |
| Neutral | 17 | 21.3 | 83 | 19.8 | 8 | 18.6 | 40 | 21.1 |
| Agree | 24 | 30.0 | 60 | 14.3 | 13 | 30.2 | 34 | 18.0 |
| Strongly agree | 6 | 7.5 | 6 | 1.4 | 4 | 9.3 | 3 | 1.6 |
| Item 5: I usually come through difficult times with little trouble | ||||||||
| Strongly disagree | 10 | 12.5 | 4 | 1 | 4 | 9.3 | 4 | 2.1 |
| Disagree | 33 | 41.3 | 95 | 22.6 | 17 | 39.5 | 45 | 23.8 |
| Neutral | 14 | 17.5 | 118 | 28.1 | 14 | 32.6 | 56 | 29.6 |
| Agree | 20 | 25.0 | 162 | 38.6 | 7 | 16.3 | 69 | 36.5 |
| Strongly agree | 3 | 3.8 | 41 | 9.8 | 1 | 2.3 | 15 | 7.9 |
| Item 6: I tend to take a long time to get over setbacks in my life | ||||||||
| Strongly disagree | 7 | 8.8 | 70 | 16.7 | 5 | 11.6 | 26 | 13.8 |
| Disagree | 22 | 27.5 | 201 | 47.9 | 11 | 25.6 | 96 | 50.8 |
| Neutral | 21 | 26.3 | 92 | 21.9 | 12 | 27.9 | 45 | 23.8 |
| Agree | 24 | 30.0 | 51 | 12.1 | 11 | 25.6 | 20 | 10.6 |
| Strongly agree | 6 | 7.5 | 6 | 1.4 | 4 | 9.3 | 2 | 1.1 |
| Global resilience (total score)b | ||||||||
| Low | 36 | 46.0 | 62 | 14.8 | 21 | 47.7 | 33 | 18.2 |
| Normal | 39 | 48.8 | 283 | 67.4 | 20 | 45.5 | 133 | 69.3 |
| High | 5 | 6.3 | 75 | 17.9 | 3 | 6.8 | 24 | 12.5 |
| First wave (N=500) ≥1 new-onset PPsyDs | Second wave (N=236) ≥1 new-onset PPsyDs | |||||||
|---|---|---|---|---|---|---|---|---|
| Yes (N=80, 16.0%) | No (N=420, 84%) | Yes (N=44, 18.6%) | No (N=192, 81.4%) | |||||
| Characteristica | N | % | N | % | N | % | N | % |
| Perception of being supported by relatives or household members when facing difficulties | ||||||||
| Strongly disagree | 7 | 8.8 | 8 | 1.9 | 8 | 18.6 | 7 | 3.7 |
| Disagree | 8 | 10.0 | 30 | 7.1 | 3 | 7.0 | 15 | 7.9 |
| Neutral | 23 | 28.8 | 93 | 22.1 | 12 | 27.9 | 32 | 16.9 |
| Agree | 26 | 32.5 | 205 | 48.8 | 12 | 27.9 | 89 | 47.1 |
| Strongly agree | 16 | 20.0 | 84 | 20 | 8 | 18.6 | 46 | 24.3 |
| Perception of being supported by friends or colleagues when facing difficulties | ||||||||
| Strongly disagree | 1 | 1.3 | 11 | 2.6 | 4 | 9.3 | 8 | 4.2 |
| Disagree | 9 | 11.3 | 35 | 8.3 | 4 | 9.3 | 8 | 4.2 |
| Neutral | 28 | 35.0 | 132 | 31.4 | 9 | 20.9 | 45 | 23.8 |
| Agree | 35 | 43.8 | 201 | 47.9 | 18 | 41.9 | 106 | 56.1 |
| Strongly agree | 7 | 8.8 | 41 | 9.8 | 8 | 18.6 | 22 | 11.6 |
| Perception of being supported by religious convictions when facing difficulties | ||||||||
| Strongly disagree | 33 | 41.3 | 108 | 25.7 | 23 | 53.5 | 63 | 33.3 |
| Disagree | 8 | 10.0 | 49 | 11.7 | 2 | 4.7 | 22 | 11.6 |
| Neutral | 17 | 21.3 | 122 | 29 | 10 | 23.3 | 58 | 30.7 |
| Agree | 15 | 18.8 | 104 | 24.8 | 7 | 16.3 | 29 | 15.3 |
| Strongly agree | 7 | 8.8 | 37 | 8.8 | 1 | 2.3 | 17 | 9.0 |
| Disposition to trusting one's own capacities | ||||||||
| Strongly disagree | 5 | 6.3 | 4 | 1 | 2 | 4.8 | 4 | 2.1 |
| Disagree | 16 | 20.0 | 29 | 6.9 | 8 | 19 | 22 | 11.8 |
| Neutral | 15 | 18.8 | 70 | 16.7 | 6 | 14.3 | 25 | 13.4 |
| Agree | 30 | 37.5 | 227 | 54 | 21 | 50 | 111 | 59.4 |
| Strongly agree | 14 | 17.5 | 90 | 21.4 | 5 | 11.9 | 25 | 13.4 |
| Disposition to planning work activities efficiently | ||||||||
| Strongly disagree | 4 | 5.0 | 5 | 1.2 | 1 | 2.4 | 3 | 1.6 |
| Disagree | 9 | 11.3 | 25 | 6 | 9 | 21.4 | 18 | 9.6 |
| Neutral | 12 | 15.0 | 45 | 10.7 | 4 | 9.5 | 23 | 12.3 |
| Agree | 41 | 51.3 | 247 | 58.8 | 21 | 50 | 110 | 58.8 |
| Strongly agree | 14 | 17.5 | 98 | 23.3 | 7 | 16.7 | 33 | 17.6 |
| Disposition to socializing easily | ||||||||
| Strongly disagree | 2 | 2.5 | 2 | 5 | 3 | 7.1 | 4 | 2.1 |
| Disagree | 19 | 23.8 | 43 | 10.2 | 5 | 11.9 | 22 | 11.8 |
| Neutral | 20 | 25.0 | 87 | 20.7 | 8 | 19 | 35 | 18.7 |
| Agree | 27 | 33.8 | 181 | 43.1 | 16 | 38.1 | 100 | 53.5 |
| Strongly agree | 12 | 15.0 | 107 | 25.5 | 10 | 23.8 | 26 | 13.9 |
Training and testing protocol.
Estimating the importance of predictive variables.
Results
Performance of ML Algorithm
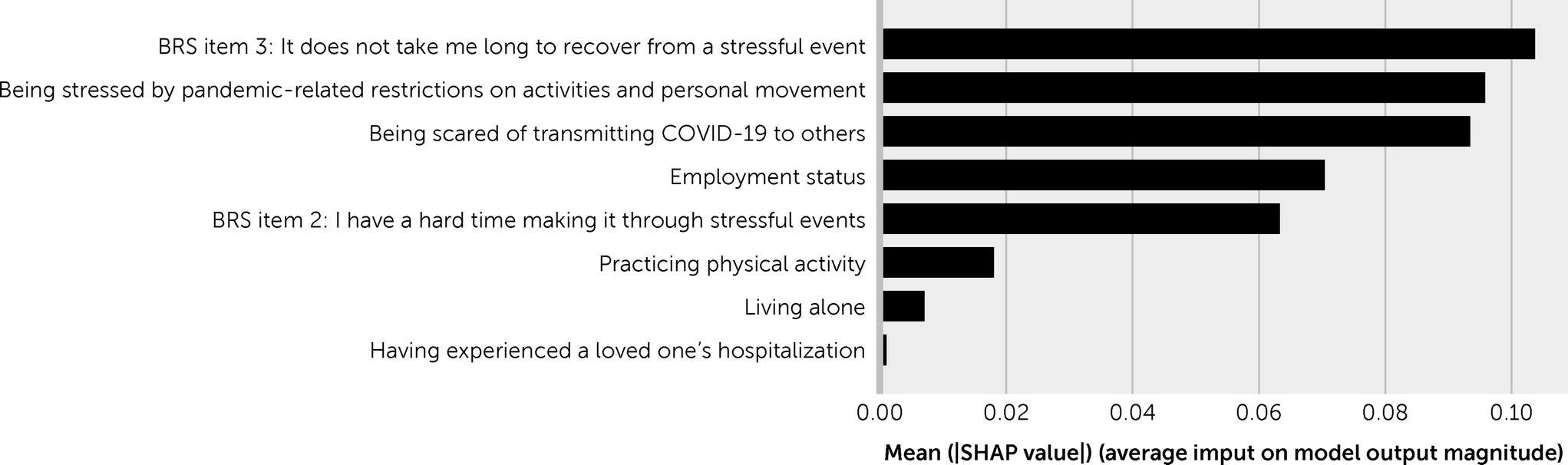
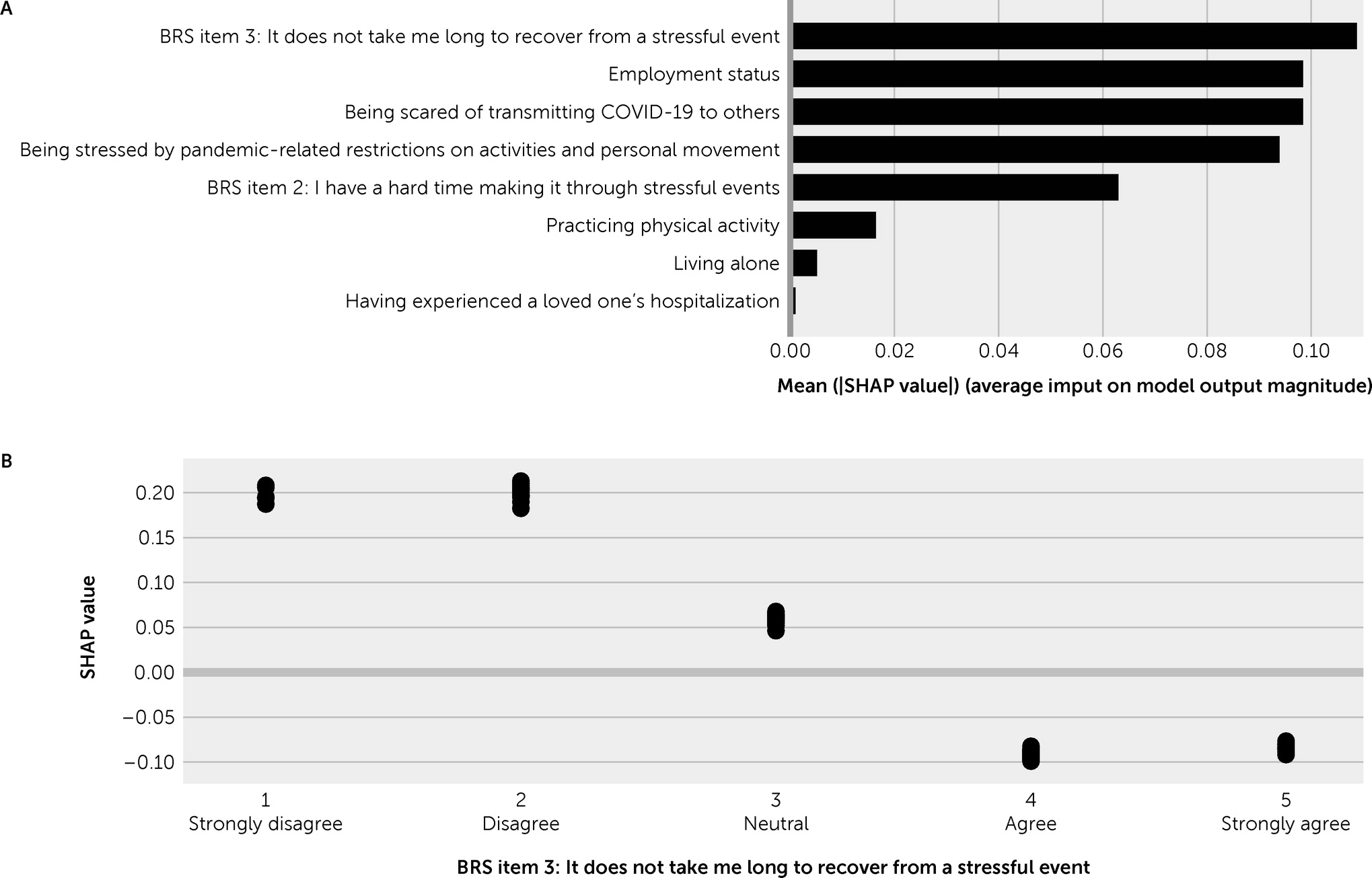
Importance of Predictive Variables
Discussion
New-Onset PPsyDs
ML Predictive Model
Conclusions
Supplementary Material
- View/Download
- 167.27 KB
References
Information & Authors
Information
Published In
History
Keywords
Authors
Funding Information
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).