Diagnosing Adolescent Substance Use and Co‐Occurring Disorders Using the Global Appraisal of Individual Needs Quick Version‐4
Publication: Psychiatric Research and Clinical Practice
Abstract
Objective
Early identification of substance use during adolescence is imperative to reduce the risk of morbidity and mortality. The aim of this study was to determine the utility of the Global Appraisal of Individual Needs‐Quick Version 4 (GAIN‐Q4) at diagnosing substance use disorders (SUDs) in adolescents.
Methods
The GAIN‐Q4 was developed from the GAIN‐Quick Version 3 by adding items from the original measure (GAIN‐I) to diagnose SUDs and provide level of care recommendations. Prevalence, sensitivity (SE), specificity, Cohen's kappa, and percent agreement between the GAIN‐I and GAIN‐Q4 were calculated for substance use and mental health (MH) diagnoses. The GAIN‐I was administered to adolescents aged 12–17 and adults across levels of care and service settings from 2002 to 2018. The sample included 101,897 adolescents (71.50% male; average age 15.59, SD = 1.25 years) and 204,711 adults aged 18 and older (61.72% male; average age 34.24; SD = 11.67).
Results
Nearly half of adolescents (43%) had at least one SUD and one MH diagnosis based on the GAIN‐Q4. The sensitivity and specificity of the GAIN‐Q4 for diagnosing any SUD in adolescents was 89% and 93%, respectively. There was 90% agreement between the GAIN‐Q4 and GAIN‐I for any SUD (Cohen's kappa of 0.80). Sensitivities for all SUD subtypes were >90%.
Conclusions
The GAIN‐Q4 is excellent at identifying adolescents with problems related to co‐occurring MH and SUDs (SE = 97%). The GAIN‐Q4 is a reliable instrument for the diagnosis of SUDs in adolescents and has the potential to facilitate appropriate allocation of treatment resources.
Trial registration
ClinicalTrials.gov Identifier: NCT05001399.
HIGHLIGHTS
•
There is considerable variation in the frequency and use of evidence‐based screening and diagnostic tools among clinicians targeting adolescent substance use.
•
This study determines the utility of the Global Appraisal of Individual Needs‐Quick Version 4 (GAIN‐Q4) at diagnosing substance use disorders (SUDs) and co‐occurring mental health disorders in adolescents.
•
Results support the utility of the GAIN‐Q4 in diagnosing SUDs in adolescents given the strong sensitivity (89%), specificity (93%), Cohen's kappa (0.80), and percent agreement (90%) for any SUD diagnosis.
•
The GAIN‐Q4 was able to detect problems associated with co‐occurring diagnoses in adolescents with excellent sensitivity (97%).
•
The reliability of the GAIN‐Q4 as a diagnostic measure should allow providers to feel comfortable using this abbreviated instrument to provide rapid and accurate diagnosis of SUDs and co‐occurring disorders in the adolescent population.
Substance use disorders (SUDs) are associated with significant morbidity and mortality in the adolescent population. Recent estimates indicate approximately 8.5% or 2.2 million adolescents, aged 12–17 in the U.S. met DSM‐5 criteria for a SUD in the past year, based on individual self‐report (1). Early exposure to substances can have detrimental effects, increasing the risk of developing SUDs, mood disorders, and the transition to other forms of substance use later in life (2, 3, 4). Adolescents who use substances are at higher risk of victimization, bullying, and high‐risk sexual behaviors (5, 6, 7). Higher rates of suicidality and overdose are also observed in this patient population (8, 9). Timely recognition and diagnosis of SUDs is necessary to decrease the risk of future health consequences.
There is considerable variation in the frequency and use of evidence‐based screening tools among clinicians targeting adolescent substance use, often influenced by barriers such as limited time, training, and familiarity with standardization (10, 11, 12). Proper SUD diagnosis is critical as positive screens are often insufficient in eliciting appropriate intervention (12). The majority of adolescents who need specialty substance use treatment do not receive it, even after an overdose event (1, 13). Those who are able to be enrolled in care often require efficient treatment planning given the scarcity of adolescent‐tailored resources (14). Processes that streamline the receipt of accurate SUD diagnosis to treatment placement are needed to connect adolescents with timely care.
The Global Appraisal of Individual Needs‐Initial (GAIN‐I) is an assessment tool used to diagnose and develop treatment plans for mental health (MH) disorders and SUDs using patient self‐report for adolescents and adults (15). The GAIN‐Quick Version 3 (GAIN‐Q3) was developed from the original, lengthier version to screen for substance use, MH and associated problems in a shorter period of time, while assessing an individual's level of current functioning or impairment (16). The Global Appraisal of Individual Needs‐Quick Version 4 (GAIN‐Q4) is an adaptation of the GAIN‐Q3 and integrates additional validated items from the GAIN‐I to further address diagnostic criteria for SUDs and co‐occurring MH disorders. The aim of this study is to investigate the utility of the GAIN‐Q4 as a diagnostic tool for SUDs and co‐occurring MH disorders in adolescents ages 12–17.
METHODS
Participants & Procedures
Participants were assessed using the GAIN‐I software during in‐person clinical interviews, which took on average 95 min to administer (SD = 134.7 min). Interviews occurred between 2002 and 2018 across various institutional settings, but primarily took place at treatment facilities (65%). Other settings included child protective services, employee or student assistance programs, and justice agencies. This study uses data collected from individuals (N = 306,608) aged 12 or older (33% adolescents and 67% adults) gathered at 519 sites from 43 states in the U.S. by 5599 staff members (17). Funding for data collection came from a variety of sources throughout the 16‐year collection timespan, including the Substance Abuse and Mental Health Services Administration's Center for Substance Abuse Treatment (CSAT), the National Institute on Alcohol and Alcoholism, National Institute on Drug Abuse, and the Robert Wood Johnson Foundation, the Interventions Foundation. Additional behavioral health care funding was received from multiple states, county, system (e.g., Department of Public Health) or individual human service agencies (16). The development and evaluation of the GAIN‐Q4 was jointly funded by the Connecticut Department of Children and Family (DCF) and Chestnut Health Systems.
All data was gathered from clinical practice or specific research projects after voluntary consent was obtained and/or Institutional Review Boards requirements were met (16, 17). All patient information was de‐identified prior to analysis (17). A subset of the data was created to include only individuals aged 12–17 (N = 101,897) for comparative analysis.
Measures
The GAIN‐I is a biopsychosocial, semi‐structured assessment tool created to diagnose and aid in treatment planning of MH and SUDs for individuals 12 and older in treatment settings (15, 18). The original instrument, which takes 90–120 min for administration, uses self‐report to diagnose disorders using criteria from the DSM‐5 and the International Classification of Diseases and creates recommendations for treatment planning and level of care placement (16, 18). The GAIN‐I's classical scales and summative indices are combined to generate a hierarchical system that provides information about severity, clinically‐orientated subscales, sources of variation, and item levels for safety planning, such as suicide risk (15). Primary SUDs diagnosed by the GAIN include alcohol, cannabis, opioids, stimulants, and other drugs (19). The GAIN and its subsets are reliable tools across various patient populations including adolescents, pregnant/postpartum women, and other demographic groups (16, 20, 21, 22, 23, 24). The GAIN‐I's major scales have shown internal consistency (alpha over 0.90 on main scales, 0.70 on subscales) (16). Test‐retest reliability (rho over 0.70 on number of days and problem counts, kappa over 0.60 on categorical measures) is strong in adolescent and adult populations (16).
The GAIN‐Q3 is a brief assessment tool developed using a subset of items from the GAIN‐I to quickly evaluate common clinical problem areas within 15–45 min (16, 18). The GAIN‐Q3 utilizes separate measures to identify School Problems (4 problems), Work Problems (4 items), Physical Health (4 items), Sources of Stress (8 items), Risk Behaviors (10 items), Internalizing Disorders (6 items), Externalizing Disorders (7 items), Substance Disorders (5 items), and Crime and Violence (5 items) (16). Items within each GAIN‐Q3 screener capture problem recency by quantifying symptoms for past month, past 90 days, past 12 months, lifetime, and by quantifying duration of remission (16). Using data collected from GAIN‐I, the GAIN‐Q3 has demonstrated convergent and discriminate validity relative to the full‐length GAIN‐I (16). The Total Disorder Screener on the GAIN‐Q3 achieves internal consistency (α = 0.90) for adolescent and adult populations (16). The GAIN‐Q4 was developed from the validated GAIN‐Q3 in order to encapsulate diagnosis, treatment planning, and placement (25). The GAIN‐Q4 includes the minimum required items from the GAIN‐I to predict American Society of Addiction Medicine (ASAM) treatment placement and create an ASAM summary section within the GAIN‐Q4 Recommendation and Referral Summary (Q4RRS) report (25). Other modifications include requiring responses to readiness to change items, adding questions to capture recency and lifetime diagnoses, and creating sections addressing prior diagnoses and disability measures (25). The following items and sections were added to the GAIN‐Q3 to create the modified GAIN‐Q4:
•
ASAM summary section.
•
Sex at birth, identity, and pronouns.
•
Client feelings over the past month involving components of satisfaction, happiness, community, and purpose.
•
Physical and emotional symptoms that may be associated with withdrawal.
•
Problems or limitations that may restrict physical abilities including wearing prescription glasses or contacts, a hearing aid, artificial limbs, and other mobility aids.
•
Treatment for mental, emotional, behavioral, or psychological problems including past statements from clinicians and problems they may have asked about.
•
Reasons for substance use, current treatment, and other use.
•
Safety in the home, comradery, closeness, and nature of interactions between family members.
The GAIN‐I versions 5.1–5.7 and the GAIN‐Q3 versions 3.0–3.2 were used to evaluate patient characteristics, substance use, and comorbidity during intake. The entirety of the data was collected within the scope of general clinical practice, or during research studies after voluntary consent was given. For more information on the items that are used to generate diagnostic impressions, please see the GAIN‐Q4 Diagnoses Descriptions Memo in Table A1.
Data Analysis
Various iterations of item combinations from the component sets used by the GAIN‐I to make specific diagnoses were analyzed. Each version's ability to make a formal diagnosis was compared to the GAIN‐I by assessing sensitivity, specificity and kappa values. The most optimized version was used in the development of the new GAIN‐Q4. This was replicated for each MH and substance diagnosis in the GAIN‐Q4.
When comparing adolescent and adults' characteristics on dichotomous measures, we used logistic regression. Given the large sample size, we focused on those that were both statistically (p < 0.05) and clinically significant with odds ratios (OR). Reported confidence intervals that do not encompass a value of 1.0 indicate statistical significance. Due to large sample sizes, we report confidence intervals rather than p values for its greater depth of explanatory detail. We interpret a characteristic as more likely for adolescents when the OR is 1.2 or more. We interpret a characteristic as less likely for adolescents when the OR is 0.8 or less. For multi‐level placement, we compare adolescents and adults using a chi‐square test.
Sensitivity, specificity, Cohen's kappa, and actual agreement for each substance use and MH diagnosis was calculated by using the GAIN‐I as the “gold standard” for diagnosis and the modified version of the GAIN‐Q3 (GAIN‐Q4) as the “test measure” in the adolescent sample. The predictive validity of the GAIN‐Q4 for each substance use and MH diagnosis were analyzed by examining the percent of exact agreement between the GAIN‐I and GAIN‐Q4, as well as with Kappa. Kappa adjusts the rate of agreement for prevalence and chance; we interpret kappa between the short and full measures of 0.4–0.59 as fair, 0.6–0.79 as good, and 0.8 or more as excellent agreement. In real data, we want to see the kappa at 0.6 (good) or more and consider 0.8 or more to be a near perfect match. All analytics were performed using IBM® Statistical Package for Social Sciences® (SPSS) Version 29 (26). For this study, sensitivities, specificities, and actual agreement percentages of 70% are considered fair, 80% are good, and 90% are excellent, in line with previous GAIN literature (16).
RESULTS
Sample Characteristics
Table 1 describes characteristics of the sample, including 101,897 adolescents aged 12–17 (71.50% male; average age 15.59, SD = 1.25 years). Table A1 includes prevalence by treatment setting. Adolescents were compared to a sample of 204,711 adults aged 18 and older (61.72% male; average age 34.23; SD = 11.67). Both populations used were racially diverse, had similar levels of involvement in the criminal justice system, and were majority male. Adolescents were more likely to report cannabis use in the last 90 days, while adults had higher rates of stimulant, opioid, and needle use. Both groups had similar levels of alcohol and other drug use. Adolescents were more likely to have a history of attention‐deficit/hyperactivity, conduct, and oppositional defiant disorders. Adults had a higher prevalence of prior diagnoses of alcohol or drug use disorders, anxiety or phobia disorder, major depression and other mood disorders, intellectual disabilities, pathologic gambling, post or acute traumatic stress disorders, somatoform disorders, schizophrenia or psychotic disorders, and other cognitive and mental diagnoses.
| Characteristics | Adolescents (12–17) | Adults (18 +) | OR (95% CI) |
|---|---|---|---|
| N = 101,897 | N = 204,711 | ||
| Age‐ mean (SD) | 15.6 (1.25) | 34.2 (11.67) | n/a |
| Male (%) | 71.5% | 61.7% | 1.56 (1.53–1.58) |
| Race/ethnicity | |||
| Non‐Hispanic African American (%) | 24.0% | 16.5% | 1.6 (1.58–1.63) |
| Non‐Hispanic Caucasian (%) | 47.8% | 65.7% | 0.48 (0.47–0.49) |
| Hispanic (%) | 26.7% | 14.7% | 2.12 (2.08–2.16) |
| Mixed/other (%) | 13.1% | 7.3% | 1.91 (1.86–1.95) |
| Assessment setting | |||
| Legal system | 9.3% | 15.8% | 0.55 (0.54–0.56) |
| Treatment | 53.7% | 70.8% | 0.48 (0.47–0.49) |
| Home/office | 19.1% | 3.0% | 7.7 (7.47–7.93) |
| Other | 10.5% | 3.9% | 2.87 (2.79–2.96) |
| Unknown | 7.3% | 6.5% | 1.13 (1.1–1.17) |
| Past 90‐day use of alcohol (%) | 50.3% | 49.3% | 1.04 (1.03–1.06) |
| Past 90‐day use of cannabis (%) | 73.5% | 35.0% | 5.14 (5.05–5.23) |
| Past 90‐day use of stimulants (%) | 12.4% | 30.7% | 0.32 (0.31–0.33) |
| Past 90‐day use of opioids (%) | 10.1% | 25.4% | 0.33 (0.32–0.34) |
| Past 90‐day use of other (%) | 16.7% | 14.2% | 1.21 (1.18–1.23) |
| Any past year needle use (%) | 1.7% | 20.5% | 0.07 (0.06–0.07) |
| Current involvement in legal system (%) | 67.8% | 67.9% | 0.99 (0.98–1.01) |
| Any prior diagnoses (%) | 37.3% | 51.3% | 0.57 (0.56–0.58) |
| Alcohol or drug use disorders (%) | 2.7% | 10.2% | 0.24 (0.23–0.25) |
| Attention‐deficit/hyperactivity disorder (%) | 21.5% | 13.8% | 1.71 (1.67–1.74) |
| Antisocial personality disorder (%) | 0.2% | 1.2% | 0.18 (0.16–0.21) |
| Anxiety or phobia disorder (%) | 6.8% | 20.6% | 0.28 (0.27–0.29) |
| Borderline personality disorder (%) | 0.5% | 2.5% | 0.18 (0.16–0.2) |
| Conduct disorder (%) | 1.0% | 0.6% | 1.74 (1.59–1.91) |
| Major depression disorder (%) | 6.4% | 16.0% | 0.36 (0.35–0.37) |
| Other depression, bipolar or mood disorder (%) | 12.1% | 24.7% | 0.42 (0.41–0.43) |
| Intellectual disabilities (%) | 0.2% | 0.4% | 0.5 (0.42–0.59) |
| Oppositional defiant disorder (%) | 2.1% | 0.6% | 3.83 (3.56–4.13) |
| Pathological gambling (%) | 0.0% | 0.0% | 0.24 (0.12–0.46) |
| Post or acute traumatic stress disorder (%) | 2.6% | 9.5% | 0.25 (0.24–0.26) |
| Somatoform, pain, sleep, eating or body disorder (%) | 0.7% | 1.1% | 0.65 (0.59–0.71) |
| Other cognitive disorder (%) | 0.0% | 0.1% | 0.34 (0.24–0.48) |
| Other mental breakdown, nerves, or stress (%) | 0.2% | 0.7% | 0.28 (0.24–0.33) |
| Other personality disorder (%) | 0.5% | 2.4% | 0.22 (0.2–0.25) |
| Other schizophrenia or psychotic disorder (%) | 0.4% | 3.6% | 0.12 (0.11–0.13) |
| Other (%) | 2.1% | 2.3% | 0.94 (0.89–0.99) |
a
The significance of bold values is p ≤ 0.001.
Prevalence
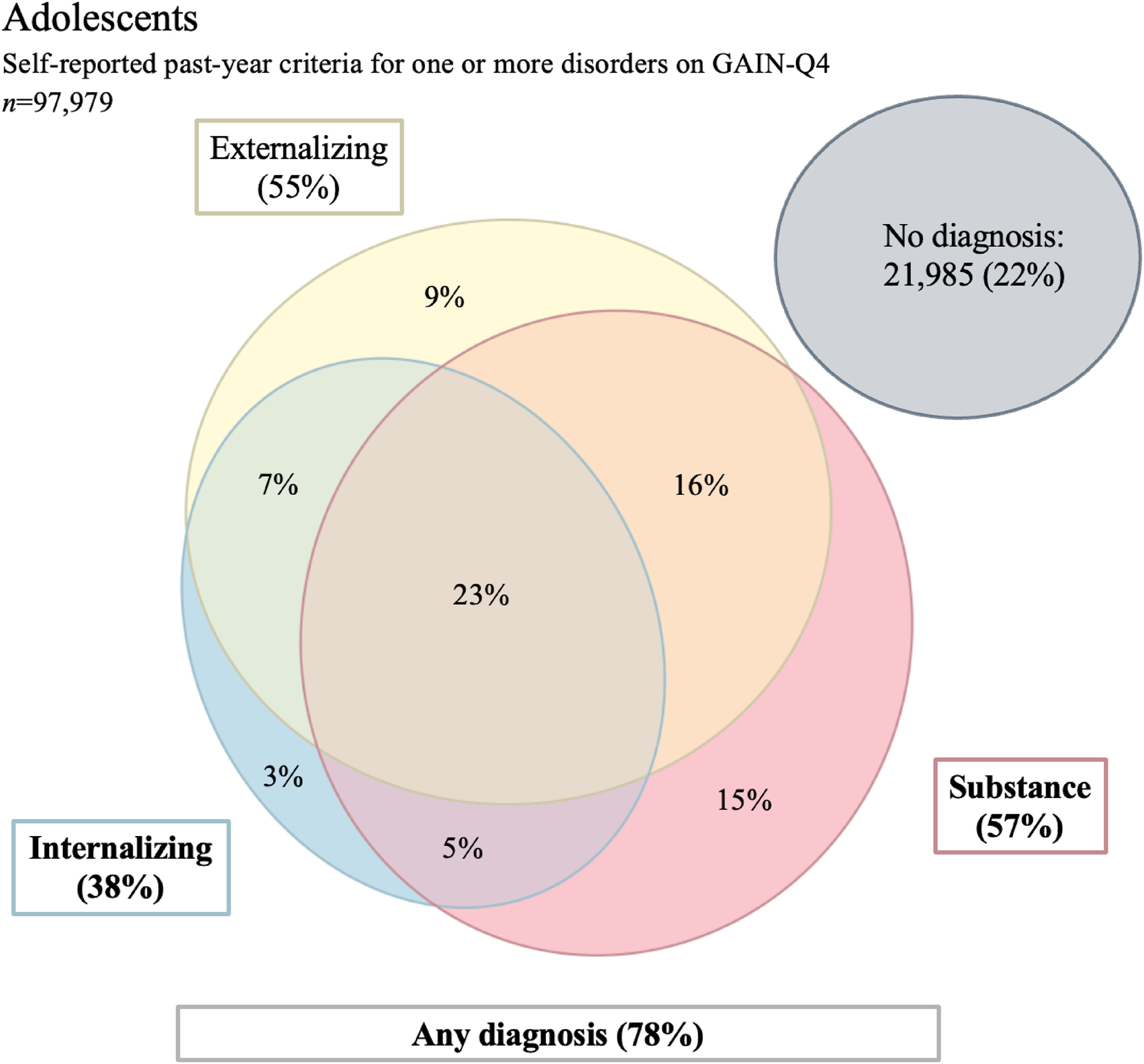
Table 2 displays the prevalence of 17 MH and substance use diagnoses included the GAIN‐Q4 and the GAIN‐I. SUDs were identified as the most common diagnoses in this sample for both the GAIN‐Q4 (58%) and GAIN‐I (61%), with cannabis use disorder as the most common subtype (Q4 = 54%, I = 50%). The prevalence of externalizing mental health (EMH) disorders was 55% from the GAIN‐Q4 and 51% from the GAIN‐I, followed by internalizing mental health (IMH) disorders (GAIN‐Q4 = 38%; GAIN‐I = 37%). Both the GAIN‐I and GAIN‐Q4 predicted high prevalence of 3 or more problems associated with the MH and SUDs analyzed (GAIN‐Q4 = 69%; GAIN‐I = 53%). Figure 1 demonstrates the prevalence of co‐occurring disorders in this sample. Of the adolescents sampled, 23% had a SUD, an IMH and an EMH. Combinations of two of these diagnoses were common, and the prevalence of having a SUD and at least an IMH or an EMH was 44%.
| Past year mental health diagnosis | Prevalence GAIN Q‐4 | Prevalence GAIN‐I | N of yes | Kappa | Sensitivity | Specificity | Percent agreement |
|---|---|---|---|---|---|---|---|
| Substance use disorder probable diagnosis | 58% | 61% | 57,945 | 0.80 | 89% | 93% | 90% |
| Cannabis | 54% | 50% | 53,887 | 0.71 | 91% | 80% | 85% |
| Alcohol | 46% | 17% | 45,984 | 0.33 | 92% | 63% | 68% |
| Stimulant | 17% | 7% | 16,768 | 0.48 | 93% | 89% | 89% |
| Opioid | 15% | 4% | 15,126 | 0.34 | 97% | 88% | 88% |
| Other drug | 22% | 5% | 22,146 | 0.31 | 95% | 82% | 82% |
| Internalizing mental health probable diagnosis | 38% | 37% | 37,853 | 0.74 | 85% | 89% | 88% |
| Mood | 27% | 30% | 26,789 | 0.68 | 73% | 93% | 87% |
| Anxiety | 26% | 10% | 26,235 | 0.50 | 99% | 83% | 85% |
| Trauma | 25% | 22% | 24,926 | 0.76 | 85% | 93% | 91% |
| Suicide | 11% | 12% | 11,285 | 0.97 | 95% | 100% | 99% |
| Possible psychosis | 7% | 7% | 6640 | 1.00 | 100% | 100% | 100% |
| Externalizing mental health probable diagnosis | 55% | 51% | 54,388 | 0.72 | 90% | 82% | 86% |
| Conduct | 45% | 42% | 45,119 | 0.68 | 85% | 84% | 84% |
| ADHD (Attention‐ deficit/hyperacticity disorder) | 52% | 32% | 51,781 | 0.59 | 96% | 72% | 80% |
| Gambling | 1% | 1% | 1160 | 0.41 | 73% | 99% | 99% |
| 3+ of above problems | 69% | 53% | 70,560 | 0.59 | 97% | 62% | 80% |
a
GAIN Q‐4, Global Appraisal of Individual Needs‐Quick Version 4; MH, mental health.
Sensitivity and Specificity
Table 2 highlights the sensitivity (SE) and specificity (SP) for each MH and substance use diagnosis. Results demonstrated the GAIN‐Q4 could identify any SUD in adolescents with accuracy considered good based on sensitivity and specificity (SE = 89%; SP = 93%). All specific SUDs had sensitivities and specificities >80% except for alcohol use disorder (SE 92%; SP = 63%) indicating good accuracy. All subtypes of SUDs had sensitivities >90%, indicating excellent sensitivity. Mental health diagnoses also demonstrate sensitivities and specificities over 70% representing fair accuracy. The possible psychosis category had excellent sensitivity and specificity values of 100%. The sensitivity of the GAIN‐Q4 regarding identifying three or more problems associated with co‐occurring diagnoses was excellent (97%). Specificity for this category was 62%.
Agreement
Table 2 displays the agreement for each substance use and MH diagnosis between the GAIN‐Q4 and GAIN‐I as Cohen's kappa and percent agreement. The agreement for any SUD diagnoses in adolescents was substantial based on kappa values (0.80) and excellent based on percent agreement (90%). All specific SUD diagnoses had percent agreements >80% except for alcohol use disorder (68%), still indicating good agreement. Kappa values for cannabis use and stimulant use disorders were above 0.41, representing moderate agreement between the GAIN‐Q4 and GAIN‐I. All other specific SUD diagnoses (alcohol, opioid and other) had kappa values above 0.21, indicating fair agreement between tools. The agreement for both IMH and EMH diagnoses and subtypes was moderate based on kappa (≥0.41) and good based on percent agreement (≥80%). Agreement for recognizing three or more problems associated with co‐occurring diagnoses was similar (κ = 0.59; percent agreement = 80%).
The nine diagnoses in Table 2 that demonstrated substantial agreement between measures included any SUD (0.80), and cannabis disorder (0.71), any IMH disorder (0.74), trauma (0.76), suicide (0.97), possible psychoses (1.00), and any EMH disorder (0.72). The kappa values for alcohol use disorder (0.33), opioid use disorder (0.34), and other drug use disorder (0.31) represent fair agreement between measures.
DISCUSSION
This study evaluates the reliability of the GAIN‐Q4 as a diagnostic tool for SUDs in adolescents. Results demonstrate the ability of the GAIN‐Q4 to diagnose any SUD with good sensitivity (89%), excellent specificity (93%), substantial kappa (0.80) and excellent percent agreement (90%). The GAIN‐Q4's ability to diagnose specific SUDs (cannabis, alcohol, stimulant, opioid and other) in this population is highlighted by excellent sensitivity values (>90%) across all diagnoses and good percent agreements (>80%) excluding alcohol use disorder (68%). Results from this study also emphasize the GAIN‐Q4's ability to detect problems associated with co‐occurring diagnoses in adolescents with excellent sensitivity (97%).
The GAIN‐Q4 performed similarly to the well‐established GAIN‐I measure (16, 20, 21, 22), and provides a single instrument that can quickly and reliably diagnose SUDs and co‐occurring disorders in adolescents. Failure to recognize and treat SUDs in adolescence increases the risk of negative consequences throughout adulthood. Earlier onset of substance use is associated with higher rates of future health problems and risk behaviors, including development of mood disorders and transition to use of other types of substances with more severe consequences, such as opioids (3, 27). Current screening instruments for substance use in adolescents are limited by their inability to provide diagnoses and subsequently encourage appropriate treatment intervention (28, 29). Results of this study indicate that the GAIN‐Q4 can offer accurate diagnosis of any SUD in a timely manner, thus providing a valuable clinical instrument for use in this population.
The GAIN‐Q4 performed well when identifying adolescents with specific SUDs, displayed by its high sensitivities (>90%) across all substances analyzed in this study. The agreement between the GAIN‐Q4 and its parental counterpart for diagnosing specific SUDs was fair based on Cohen's kappa (>0.3) and good based on percent agreement (>80%) except for alcohol use. This could be explained by the GAIN‐Q4's overestimation of specific SUD prevalence compared to the GAIN‐I presented in Table 1. We suspect that part of the challenge was the high prevalence of alcohol use (potentially in more frequent but lower amounts) with other drug use and disorders. But this study was not designed to address this hypothesis. From a clinical perspective, identification of any concerning substance use is critical, so individuals can quickly initiate therapy and treatment that can then be tailored for specific or multiple SUDs. Additionally, substance use items may cross over frequently due to the high prevalence of co‐morbid SUDs. The results of this study demonstrate that the GAIN‐Q4 can quickly recognize SUD patterns in adolescents to efficiently facilitate treatment initiation.
In addition to identifying general substance use and specific SUDs in adolescents, the GAIN‐Q4 can simultaneously recognize other psychiatric diagnoses. Co‐occurring MH disorders and SUDs are common in the adolescent population (1, 30). In this sample, nearly half of the adolescents had an IMH or an EMH in addition to a SUD diagnosis (44%) and almost a quarter had co‐occurring SUD, EMH and IMH diagnoses (23%). The utility of the GAIN‐Q4 in adolescents is displayed by its ability to recognize problems associated with multiple psychiatric diagnoses (SE = 97%) in a short period of time unlike many diagnostic tools (15, 31, 32). Identification and treatment of co‐occurring diagnoses is imperative, as the presence of multiple psychiatric disorders intensifies disease sequelae including academic problems, HIV risk behaviors, and suicide attempts (33, 34). Outcomes for adolescents with co‐occurring disorders are poor despite receiving treatment at higher rates than those with an individual diagnosis (30). Appropriate recognition and treatment planning tailored to an individual's diagnoses is critical in a population with high prevalence of co‐occurring disorders. The GAIN‐Q4 performed particularly well at identifying possible psychosis (SE = 100%, SP = 100%) and suicide attempts (SE = 95%, SP = 100%) both of which are important risk factors for future suicidal behavior (35).
This study had numerous strengths, including a large sample, offering strong statistical power (16). Additionally, the GAIN‐Q4 is based on a reliable, full‐length diagnostic tool (GAIN‐I) (16), and provides users with treatment recommendations rooted in evidence‐based ASAM criteria in a shorter format than the GAIN‐I. Clinicians often struggle with management of care for adolescents dealing with substance use (36). The GAIN‐Q4 alleviates this issue by offering a bridge from diagnosis directly to treatment planning. One limitation of this study was the use of self‐reported data. Results have the potential to be inflated due to the use of a subset of items in the GAIN‐Q4 scale to predict all the items typically reflected in the GAIN‐I (16), with the goal of increasing efficiency. Lastly, the generalizability of results is reduced by a few factors. The sample used was diverse, but predominantly white (48%) and male (72%). Moreover, most participants were enrolled in specialized SUD, justice‐involved treatment, and MH care which potentially diminishes the applicability of these findings in other settings (16). Future studies could include validating the reliability of the GAIN‐Q4 in other clinical environments, such as primary care offices, in order to strengthen the generalizability of the instrument. Future work should determine the effectiveness of these suggestions at initiating treatment for SUDs among adolescents. It should also be noted that the development and validation of the GAIN Q4 is just one component of a multiyear process being conducted in conjunction with the Connecticut DCF. Starting in 2024 the department and its network of providers is implementing the recommendations made by the GAIN‐Q4 in order to evaluate its impact on actual treatment and patient outcomes.
The results of this study support the utility of the GAIN‐Q4 in diagnosing SUDs in adolescents given the strong sensitivity (89%), specificity (93%), Cohen's kappa (0.80), and percent agreement (90%) for any SUD diagnosis. The GAIN‐Q4 also has the ability to identify the co‐occurring MH and SUD diagnoses common in the adolescent population (1, 30). The reliability of the GAIN‐Q4 as a diagnostic measure should allow providers to feel comfortable using this abbreviated instrument to provide rapid and accurate diagnosis of SUDs in the adolescent population.
Footnotes
The opinions expressed here are those of the authors and do not represent positions of the programs, state, or others. Dr. Welsh has received consulting fees received from Applied Clinical Intelligence LLC (ACI Clinical). Ms. Modisette, Ms. Estrada, and Dr. Dennis are employed by Chestnut Health Systems, which produces the family of GAIN measures. Ms. Sitar and Dr. Durham have no disclosures to report.
These funding sources had no role in design and conduct of the study; collection, management, analysis, interpretation of data; preparation, review, approval of the manuscript; and in the decision to submit this manuscript for publication.
Thank you to Casey C. Sarapas, Ph.D., for creating Figure 1 of this manuscript.
This work was supported by the National Institute on Drug Abuse (NIDA; R21 DA046738, R01DA011323) and the Connecticut Department of Children and Family. Funding for data collection was provided by Chestnut Health Systems, and the Connecticut Department of Children and Families. Data collected by Chestnut has been funded by a number of sources over the past 16 years, including the Substance Abuse and Mental Health Services Administration's Center for Substance Abuse Treatment (CSAT), the National Institute on Alcohol Abuse and Alcoholism, the National Institute on Drug Abuse, the Interventions Foundation, the Robert Wood Johnson Foundation, and from several human service agencies at the system (i.e., Department of Public Health), state, county and individual levels. Development and evaluation of the GAIN‐Q4 was funded by the Connecticut Department of Children and Family.
To obtain data from the GAIN Coordinating Center, the appropriate Data Sharing Agreement must be signed. A small fee will be assessed for each data request. This fee allows us to assist in determining the feasibility of the proposed analyses, gathering necessary grantee permissions, preparing the data set, and providing customer service throughout this process.
Supplementary Material
Table S1
- Download
- 18.12 KB
REFERENCES
1.
Substance Abuse and Mental Health Services Administration . Key substance use and mental health indicators in the United States: results from the 2021 National Survey on Drug Use and Health (HHS Publication No. PEP22‐07‐01‐005, NSDUH Series H‐57) [Internet]. Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration; 2022 [cited 2023 Apr 9]. Available from: https://www.samhsa.gov/data/report/2021‐nsduh‐annual‐national‐report
2.
Stanis JJ, Andersen SL. Reducing substance use during adolescence: a translational framework for prevention. Psychopharmacology (Berl). 2014;231(8):1437–1453. https://doi.org/10.1007/s00213-013-3393-1
3.
Shanahan L, Hill SN, Bechtiger L, Steinhoff A, Godwin J, Gaydosh LM, et al. Prevalence and childhood precursors of opioid use in the early decades of life. JAMA Pediatr. 2021;175(3):276–285. https://doi.org/10.1001/jamapediatrics.2020.5205
4.
Steinfeld MR, Torregrossa MM. Consequences of adolescent drug use. Transl Psychiatry. 2023;13(1):313. https://doi.org/10.1038/s41398-023-02590-4
5.
Spencer CM, Anders KM, Toews ML, Emanuels SK. Risk markers for physical teen dating violence victimization in the United States: a meta‐analysis. J Youth Adolesc. 2020;49(3):575–589. https://doi.org/10.1007/s10964-020-01194-1
6.
Clayton HB, Bohm MK, Lowry R, Ashley C, Ethier KA. Prescription opioid misuse associated with risk behaviors among adolescents. Am J Prev Med. 2019;57(4):533–539. https://doi.org/10.1016/j.amepre.2019.05.017
7.
Chawla N, Sarkar S. Defining “high‐risk sexual behavior” in the context of substance use. J Psychosexual Health [Internet]. 2019 ;1(1):26–31. https://doi.org/10.1177/2631831818822015
8.
CDC WONDER, Multiple Cause of Death (Detailed Mortality) . National drug overdose (OD) deaths, 1999‐2021 [Internet]. Centers for Disease Control and Prevention; 2023 [cited 2023 Mar 13]. Available from: https://nida.nih.gov/research‐topics/trends‐statistics/overdose‐death‐rates
9.
Rioux C, Huet AS, Castellanos‐Ryan N, Fortier L, Le Blanc M, Hamaoui S, et al. Substance use disorders and suicidality in youth: a systematic review and meta‐analysis with a focus on the direction of the association. PLoS One. 2021;16(8):e0255799. https://doi.org/10.1371/journal.pone.0255799
10.
Levy SJL, Williams JF, Ryan SA, Ryan SA, Gonzalez PK, Patrick SW, et al. Substance use screening, brief intervention, and referral to treatment. Pediatrics. 2016;138(1):e20161211. https://doi.org/10.1542/peds.2016-1210
11.
Ridenour TA, Murray DW, Hinde J, Glasheen C, Wilkinson A, Rackers H, et al. Addressing barriers to primary care screening and referral to prevention for youth risky health behaviors: evidence regarding potential cost‐savings and provider concerns. Prev Sci. 2022;23(2):212–223. https://doi.org/10.1007/s11121-021-01321-9
12.
Palmer A, Karakus M, Mark T. Barriers faced by physicians in screening for substance use disorders among adolescents. Psychiatr Serv [Internet]. 2019;70(5):409–412. https://doi.org/10.1176/appi.ps.201800427
13.
Alinsky RH, Zima BT, Rodean J, Matson PA, Larochelle MR, Adger H Jr, et al. Receipt of addiction treatment after opioid overdose among Medicaid‐enrolled adolescents and young adults. JAMA Pediatr. 2020;174(3):e195183. https://doi.org/10.1001/jamapediatrics.2019.5183
14.
National Survey of Substance Abuse Treatment Services . 2020 National Survey of Substance Abuse Treatment Services (N‐SSATS) state profiles [Internet]. 2022 [cited 2023 Apr 9]. Available from: https://www.samhsa.gov/data/report/2020‐national‐survey‐substance‐abuse‐treatment‐services‐n‐ssats‐state‐profiles
15.
Dennis ML, White M, Titus JC, Unsicker J, Chestnut Health Systems . GAIN: global appraisal of individual needs: administration guide for the GAIN and related measures (Version 5); 2008.
16.
Dennis ML, Davis JP. Screening for more with less: validation of the Global Appraisal of Individual Needs Quick v3 (GAIN‐Q3) screeners. J Subst Abuse Treat. 2021;126:108414. https://doi.org/10.1016/j.jsat.2021.108414
17.
GAIN Coordinating Center, Modisette, KC, Dennis, ML. Norms, characteristics, and psychometrics using the GAIN 2018 Data Set [Internet]. Normal, IL: Chestnut Health Systems; 2022. Available from: https://chestnut.box.com/v/Norms‐2018
18.
GAIN Coordinating Center [Internet] . Gain instruments. [cited 2023 Mar 21]. Available from: https://gaincc.org/instruments/
19.
Welsh JW, Sitar SI, Dennis ML. Utility of the global appraisal of individual needs recommendation and referral report for substance use diagnosis, treatment planning, and placement. J Addiction Med. 2022;17(3):353–355. https://doi.org/10.1097/adm.0000000000001108
20.
Coleman‐Cowger VH, Dennis ML, Funk RR, Godley SH, Lennox RD. Comparison of the Addiction Severity Index (ASI) and the Global Appraisal of Individual Needs (GAIN) in predicting the effectiveness of drug treatment programs for pregnant and postpartum women. J Subst Abuse Treat. 2013;44(1):34–41. https://doi.org/10.1016/j.jsat.2012.02.002
21.
Dennis ML, Funk R, Godley SH, Godley MD, Waldron H. Cross‐validation of the alcohol and cannabis use measures in the Global Appraisal of Individual Needs (GAIN) and Timeline Followback (TLFB; Form 90) among adolescents in substance abuse treatment. Addiction. 2004;99(s2):120–128. https://doi.org/10.1111/j.1360-0443.2004.00859.x
22.
McDonell MG, Comtois KA, Voss WD, Morgan AH, Ries RK. Global appraisal of individual needs short screener (GSS): psychometric properties and performance as a screening measure in adolescents. Am J Drug Alcohol Abuse. 2009;35(3):157–160. https://doi.org/10.1080/00952990902825421
23.
Dennis M, Titus JC, Diamond G, Donaldson J, Godley SH, Tims FM, et al. The Cannabis Youth Treatment (CYT) experiment: rationale, study design and analysis plans. Addiction. 2002;97(Suppl 1):16–34. https://doi.org/10.1046/j.1360-0443.97.s01.2.x
24.
McDermeit MLD, Dawud Noursi S, Muck RD, McDermeit M. The need for developing and evaluating adolescent treatment models. In: Adolescent substance abuse treatment in the United States. Routledge; 2003.
25.
Dennis ML, Dawud‐Noursi S, Muck RD, McDermeit, M. The need for developing and evaluating adolescent treatment models. In: Stevens SJ, Morral AR, editors. Adolescent substance abuse treatment in the United States: Exemplary models from a national evaluation study. Haworth Press; 2003. pp. 3–34.
26.
IRB Corp . IBM SPSS statistics for windows version 29.0. Armonk, NY: IRB Corp; 2023.
27.
Kenneson A, Funderburk JS, Maisto SA. Substance use disorders increase the odds of subsequent mood disorders. Drug Alcohol Depend. 2013;133(2):338–343. https://doi.org/10.1016/j.drugalcdep.2013.06.011
28.
Sterling S, Valkanoff T, Hinman A, Weisner C. Integrating substance use treatment into adolescent health care. Curr Psychiatr Rep. 2012;14(5):453–461. https://doi.org/10.1007/s11920-012-0304-9
29.
Hassan A, Harris SK, Sherritt L, Van Hook S, Brooks T, Carey P, et al. Primary care follow‐up plans for adolescents with substance use problems. Pediatrics. 2009;124(1):144–150. https://doi.org/10.1542/peds.2008-2979
30.
Couwenbergh C, van den Brink W, Zwart K, Vreugdenhil C, van Wijngaarden‐Cremers P, van der Gaag RJ. Comorbid psychopathology in adolescents and young adults treated for substance use disorders: a review. Eur Child Adolesc Psychiatr. 2006;15(6):319–328. https://doi.org/10.1007/s00787-006-0535-6
31.
McLellan AT, Kushner H, Metzger D, Peters R, Smith I, Grissom G, et al. The fifth edition of the Addiction Severity Index. J Subst Abuse Treat. 1992;9(3):199–213. https://doi.org/10.1016/0740-5472(92)90062-s
32.
Robins LN, Helzer JE, Croughan J, Ratcliff KS. National Institute of Mental Health diagnostic interview schedule. Its history, characteristics, and validity. Arch Gen Psychiatr. 1981;38(4):381–389. https://doi.org/10.1001/archpsyc.1981.01780290015001
33.
Teplin LA, Elkington KS, McClelland GM, Abram KM, Mericle AA, Washburn JJ. Major mental disorders, substance use disorders, comorbidity, and HIV‐AIDS risk behaviors in juvenile detainees. Psychiatr Serv. 2005;56(7):823–828. https://doi.org/10.1176/appi.ps.56.7.823
34.
Lewinsohn PM, Rohde P, Seeley JR. Adolescent psychopathology: III. The clinical consequences of comorbidity. J Am Acad Child Adolesc Psychiatry. 1995;34(4):510–519. https://doi.org/10.1097/00004583-199504000-00018
35.
Shain B, Braverman PK, Braverman PK, Adelman WP, Alderman EM, Breuner CC, et al. Suicide and suicide attempts in adolescents. Pediatrics [Internet]. 2016;138(1):e20161420. https://doi.org/10.1542/peds.2016-1420
36.
Sterling S, Weisner C, Hinman A, Parthasarathy S. Access to treatment for adolescents with substance use and co‐occurring disorders: challenges and opportunities. J Am Acad Child Adolesc Psychiatry. 2010;49(7):637–646, quiz 725–6. https://doi.org/10.1016/j.jaac.2010.03.019
Information & Authors
Information
Published In
History
Received: 12 December 2023
Revision received: 24 May 2024
Accepted: 29 May 2024
Published online: 28 June 2024
Published in print: Winter 2024
Authors
Funding Information
Connecticut Department of Children and Family
National Institute on Drug Abuse: R21 DA046738, R01DA011323
Center for Substance Abuse Treatment
National Institute on Alcohol Abuse and Alcoholism
Interventions Foundation
Robert Wood Johnson Foundation
Chestnut Health Systems
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBFigures
Tables
Media
References
References
1.
Substance Abuse and Mental Health Services Administration . Key substance use and mental health indicators in the United States: results from the 2021 National Survey on Drug Use and Health (HHS Publication No. PEP22‐07‐01‐005, NSDUH Series H‐57) [Internet]. Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration; 2022 [cited 2023 Apr 9]. Available from: https://www.samhsa.gov/data/report/2021‐nsduh‐annual‐national‐report
2.
Stanis JJ, Andersen SL. Reducing substance use during adolescence: a translational framework for prevention. Psychopharmacology (Berl). 2014;231(8):1437–1453. https://doi.org/10.1007/s00213-013-3393-1
3.
Shanahan L, Hill SN, Bechtiger L, Steinhoff A, Godwin J, Gaydosh LM, et al. Prevalence and childhood precursors of opioid use in the early decades of life. JAMA Pediatr. 2021;175(3):276–285. https://doi.org/10.1001/jamapediatrics.2020.5205
4.
Steinfeld MR, Torregrossa MM. Consequences of adolescent drug use. Transl Psychiatry. 2023;13(1):313. https://doi.org/10.1038/s41398-023-02590-4
5.
Spencer CM, Anders KM, Toews ML, Emanuels SK. Risk markers for physical teen dating violence victimization in the United States: a meta‐analysis. J Youth Adolesc. 2020;49(3):575–589. https://doi.org/10.1007/s10964-020-01194-1
6.
Clayton HB, Bohm MK, Lowry R, Ashley C, Ethier KA. Prescription opioid misuse associated with risk behaviors among adolescents. Am J Prev Med. 2019;57(4):533–539. https://doi.org/10.1016/j.amepre.2019.05.017
7.
Chawla N, Sarkar S. Defining “high‐risk sexual behavior” in the context of substance use. J Psychosexual Health [Internet]. 2019 ;1(1):26–31. https://doi.org/10.1177/2631831818822015
8.
CDC WONDER, Multiple Cause of Death (Detailed Mortality) . National drug overdose (OD) deaths, 1999‐2021 [Internet]. Centers for Disease Control and Prevention; 2023 [cited 2023 Mar 13]. Available from: https://nida.nih.gov/research‐topics/trends‐statistics/overdose‐death‐rates
9.
Rioux C, Huet AS, Castellanos‐Ryan N, Fortier L, Le Blanc M, Hamaoui S, et al. Substance use disorders and suicidality in youth: a systematic review and meta‐analysis with a focus on the direction of the association. PLoS One. 2021;16(8):e0255799. https://doi.org/10.1371/journal.pone.0255799
10.
Levy SJL, Williams JF, Ryan SA, Ryan SA, Gonzalez PK, Patrick SW, et al. Substance use screening, brief intervention, and referral to treatment. Pediatrics. 2016;138(1):e20161211. https://doi.org/10.1542/peds.2016-1210
11.
Ridenour TA, Murray DW, Hinde J, Glasheen C, Wilkinson A, Rackers H, et al. Addressing barriers to primary care screening and referral to prevention for youth risky health behaviors: evidence regarding potential cost‐savings and provider concerns. Prev Sci. 2022;23(2):212–223. https://doi.org/10.1007/s11121-021-01321-9
12.
Palmer A, Karakus M, Mark T. Barriers faced by physicians in screening for substance use disorders among adolescents. Psychiatr Serv [Internet]. 2019;70(5):409–412. https://doi.org/10.1176/appi.ps.201800427
13.
Alinsky RH, Zima BT, Rodean J, Matson PA, Larochelle MR, Adger H Jr, et al. Receipt of addiction treatment after opioid overdose among Medicaid‐enrolled adolescents and young adults. JAMA Pediatr. 2020;174(3):e195183. https://doi.org/10.1001/jamapediatrics.2019.5183
14.
National Survey of Substance Abuse Treatment Services . 2020 National Survey of Substance Abuse Treatment Services (N‐SSATS) state profiles [Internet]. 2022 [cited 2023 Apr 9]. Available from: https://www.samhsa.gov/data/report/2020‐national‐survey‐substance‐abuse‐treatment‐services‐n‐ssats‐state‐profiles
15.
Dennis ML, White M, Titus JC, Unsicker J, Chestnut Health Systems . GAIN: global appraisal of individual needs: administration guide for the GAIN and related measures (Version 5); 2008.
16.
Dennis ML, Davis JP. Screening for more with less: validation of the Global Appraisal of Individual Needs Quick v3 (GAIN‐Q3) screeners. J Subst Abuse Treat. 2021;126:108414. https://doi.org/10.1016/j.jsat.2021.108414
17.
GAIN Coordinating Center, Modisette, KC, Dennis, ML. Norms, characteristics, and psychometrics using the GAIN 2018 Data Set [Internet]. Normal, IL: Chestnut Health Systems; 2022. Available from: https://chestnut.box.com/v/Norms‐2018
18.
GAIN Coordinating Center [Internet] . Gain instruments. [cited 2023 Mar 21]. Available from: https://gaincc.org/instruments/
19.
Welsh JW, Sitar SI, Dennis ML. Utility of the global appraisal of individual needs recommendation and referral report for substance use diagnosis, treatment planning, and placement. J Addiction Med. 2022;17(3):353–355. https://doi.org/10.1097/adm.0000000000001108
20.
Coleman‐Cowger VH, Dennis ML, Funk RR, Godley SH, Lennox RD. Comparison of the Addiction Severity Index (ASI) and the Global Appraisal of Individual Needs (GAIN) in predicting the effectiveness of drug treatment programs for pregnant and postpartum women. J Subst Abuse Treat. 2013;44(1):34–41. https://doi.org/10.1016/j.jsat.2012.02.002
21.
Dennis ML, Funk R, Godley SH, Godley MD, Waldron H. Cross‐validation of the alcohol and cannabis use measures in the Global Appraisal of Individual Needs (GAIN) and Timeline Followback (TLFB; Form 90) among adolescents in substance abuse treatment. Addiction. 2004;99(s2):120–128. https://doi.org/10.1111/j.1360-0443.2004.00859.x
22.
McDonell MG, Comtois KA, Voss WD, Morgan AH, Ries RK. Global appraisal of individual needs short screener (GSS): psychometric properties and performance as a screening measure in adolescents. Am J Drug Alcohol Abuse. 2009;35(3):157–160. https://doi.org/10.1080/00952990902825421
23.
Dennis M, Titus JC, Diamond G, Donaldson J, Godley SH, Tims FM, et al. The Cannabis Youth Treatment (CYT) experiment: rationale, study design and analysis plans. Addiction. 2002;97(Suppl 1):16–34. https://doi.org/10.1046/j.1360-0443.97.s01.2.x
24.
McDermeit MLD, Dawud Noursi S, Muck RD, McDermeit M. The need for developing and evaluating adolescent treatment models. In: Adolescent substance abuse treatment in the United States. Routledge; 2003.
25.
Dennis ML, Dawud‐Noursi S, Muck RD, McDermeit, M. The need for developing and evaluating adolescent treatment models. In: Stevens SJ, Morral AR, editors. Adolescent substance abuse treatment in the United States: Exemplary models from a national evaluation study. Haworth Press; 2003. pp. 3–34.
26.
IRB Corp . IBM SPSS statistics for windows version 29.0. Armonk, NY: IRB Corp; 2023.
27.
Kenneson A, Funderburk JS, Maisto SA. Substance use disorders increase the odds of subsequent mood disorders. Drug Alcohol Depend. 2013;133(2):338–343. https://doi.org/10.1016/j.drugalcdep.2013.06.011
28.
Sterling S, Valkanoff T, Hinman A, Weisner C. Integrating substance use treatment into adolescent health care. Curr Psychiatr Rep. 2012;14(5):453–461. https://doi.org/10.1007/s11920-012-0304-9
29.
Hassan A, Harris SK, Sherritt L, Van Hook S, Brooks T, Carey P, et al. Primary care follow‐up plans for adolescents with substance use problems. Pediatrics. 2009;124(1):144–150. https://doi.org/10.1542/peds.2008-2979
30.
Couwenbergh C, van den Brink W, Zwart K, Vreugdenhil C, van Wijngaarden‐Cremers P, van der Gaag RJ. Comorbid psychopathology in adolescents and young adults treated for substance use disorders: a review. Eur Child Adolesc Psychiatr. 2006;15(6):319–328. https://doi.org/10.1007/s00787-006-0535-6
31.
McLellan AT, Kushner H, Metzger D, Peters R, Smith I, Grissom G, et al. The fifth edition of the Addiction Severity Index. J Subst Abuse Treat. 1992;9(3):199–213. https://doi.org/10.1016/0740-5472(92)90062-s
32.
Robins LN, Helzer JE, Croughan J, Ratcliff KS. National Institute of Mental Health diagnostic interview schedule. Its history, characteristics, and validity. Arch Gen Psychiatr. 1981;38(4):381–389. https://doi.org/10.1001/archpsyc.1981.01780290015001
33.
Teplin LA, Elkington KS, McClelland GM, Abram KM, Mericle AA, Washburn JJ. Major mental disorders, substance use disorders, comorbidity, and HIV‐AIDS risk behaviors in juvenile detainees. Psychiatr Serv. 2005;56(7):823–828. https://doi.org/10.1176/appi.ps.56.7.823
34.
Lewinsohn PM, Rohde P, Seeley JR. Adolescent psychopathology: III. The clinical consequences of comorbidity. J Am Acad Child Adolesc Psychiatry. 1995;34(4):510–519. https://doi.org/10.1097/00004583-199504000-00018
35.
Shain B, Braverman PK, Braverman PK, Adelman WP, Alderman EM, Breuner CC, et al. Suicide and suicide attempts in adolescents. Pediatrics [Internet]. 2016;138(1):e20161420. https://doi.org/10.1542/peds.2016-1420
36.
Sterling S, Weisner C, Hinman A, Parthasarathy S. Access to treatment for adolescents with substance use and co‐occurring disorders: challenges and opportunities. J Am Acad Child Adolesc Psychiatry. 2010;49(7):637–646, quiz 725–6. https://doi.org/10.1016/j.jaac.2010.03.019