U.S. veterans from the Iraq and Afghanistan conflicts have high rates of psychiatric morbidity. A national study found that 37% of this veteran group received at least one psychiatric diagnosis, and 62% of these received two or more (
1). Pain, posttraumatic stress disorder (PTSD), and depression are particularly prevalent in this group, and rates of alcohol misuse, anxiety disorders, and aggressive behaviors are elevated (
1–
3). Furthermore, psychiatric diagnoses are associated with higher prevalence of general medical diseases and greater use of medical services (
4).
Despite the need for treatment among veterans returning from Iraq and Afghanistan, 70% of those with diagnoses do not obtain adequate mental health care (defined as more than eight mental health care visits in one year) (
5). Therefore, identifying correlates of mental health care utilization is essential. Most research has focused on correlates of use of specialty outpatient mental health care, but veterans may also seek mental health care in other treatment settings (such as primary care settings, emergency departments, and inpatient psychiatric settings). Little is known about which psychiatric symptoms are associated with treatment seeking in each setting, particularly after adjustment for comorbid psychiatric symptoms. This study investigated the unique associations of symptoms of distress (PTSD, depression, panic, and pain) and high-risk behaviors (alcohol misuse and aggression) with two-year prospective treatment utilization in VA treatment settings among Iraq and Afghanistan veterans.
Methods
The sample consisted of veterans returning from Iraq and Afghanistan who were assessed at intake (2005–2008) at the U.S. Department of Veterans Affairs (VA) Puget Sound Health Care System, Seattle Division (VAPSHCS). The VAPSHCS Institutional Review Board approved this study of clinic data for research purposes, waiving the need to obtain informed consent. Of 653 veterans who completed a self-report assessment, we included the 618 (95%) who had prospective health care utilization data. Most were male (N=565, 91%) and employed (N=380, 62%). Most had attended some college (N=417, 68%), had an annual income of less than $25,000 (N=321, 52%), had served in the Army (N=396, 64%), and were on active duty rather than reserve status (N=369, 60%). Nearly half were married or partnered (N=276, 45%). The mean±SD age was 30.8±8.1 years. Most (N=468, 76%) reported elevated psychiatric symptoms (that is, they screened positive for panic disorder or alcohol misuse or for at least mild symptoms of PTSD or depression) (
6,
7). Data for more than 5% of veterans in the sample were missing on race-ethnicity (N=52, 8%) and on college education (N=58, 9%). Missing data for race-ethnicity was associated with greater reported pain (p<.05); missing data for college education and other demographic variables had no significant associations with symptoms or behaviors. The sample included 406 Caucasians (66%), 54 African-Americans (9%), 15 American Indians (2%), 59 Asian or Pacific Islanders (8%), 34 Hispanics (6%), and eight “other” race or ethnicity (1%).
We used dimensional measures for most symptoms and behaviors to include subthreshold symptoms related to important clinical outcomes (
6). Depression, panic disorder, and alcohol misuse were assessed with the Patient Health Questionnaire (PHQ) (
7). PTSD was measured with the PTSD Checklist-Military Version (
8). Aggression was measured with five items adapted from the National Vietnam Adjustment Study (
9). Pain was assessed with a single item from the Short-Form Health Survey-12 (SF-12) (
10). The PHQ panic and alcohol use scales were designed as dichotomous screeners (
7), whereas all other scales were continuous. Prospective two-year data on treatment utilization were obtained from VA medical records for the following settings: primary care, mental health within primary care, outpatient mental health, emergency room, and inpatient psychiatric hospital.
Negative binomial regressions (appropriate for count outcome variables) were conducted in SPSS 16.0. We conducted single-predictor analyses in which each symptom or behavior predicted each treatment venue, as well as multivariate analyses that adjusted for comorbidity by including all significant predictors of each treatment venue. Analyses of variance or correlations were run for each demographic control variable listed above with each treatment setting. Control variables with significant associations with a treatment setting were included in subsequent analyses (p<.05).
Results
On the PHQ, the mean score for depression was 9.8±7.5 (indicating moderate depression). On the PTSD Checklist-Military Version, the mean score for PTSD was 42.2±19.1 (elevated but subclinical). The mean aggression score on the five items from the National Vietnam Adjustment Study was .6±1.0 (less than one aggressive act). The mean pain score on the single item from the SF-12 was 2.6±1.2 (moderate pain). A total of 109 veterans (18%) screened positive for panic, and 135 (22%) screened positive for alcohol misuse. Correlations ranged from −.01 (for alcohol misuse and pain) to .81 (for depression and PTSD) (median correlation=.25).
The mean numbers of treatment visits over two years were as follows: primary care, 3.9±3.5; mental health within primary care, 3.3±6.6; outpatient mental health, 7.6±26.7; emergency room, .9±1.7; and inpatient psychiatric hospitalization, .1±.5. Among veterans with elevated psychiatric symptoms, the mean numbers were similar (for example, mean outpatient mental health visits=8.8±25.6).
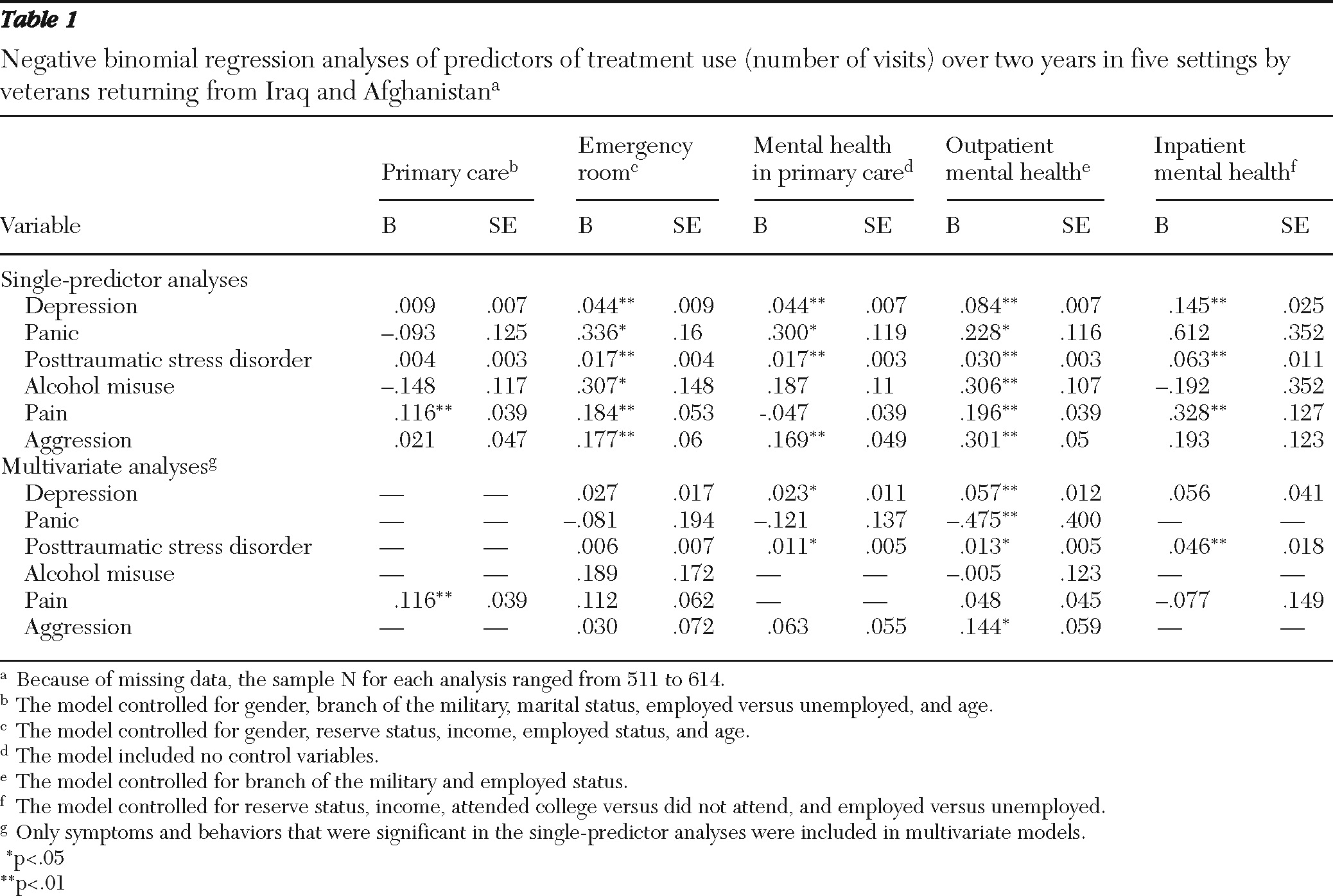
In single-predictor analyses (
Table 1), only pain was associated with use of primary care, whereas depression and PTSD were associated with use of care in all four of the other settings. Alcohol misuse was associated with emergency room and outpatient mental health utilization. Panic was associated with emergency room, mental health within primary care, and outpatient mental health utilization. In addition to use of primary care, pain was associated with use of the emergency room, outpatient mental health care, and inpatient care. Aggression was associated with use of the emergency room, mental health within primary care, and outpatient mental health care.
Multivariate analyses adjusting for comorbidity were conducted with significant predictors from the single-predictor analyses (
Table 1). Pain was associated with use of primary care. Depression and PTSD were associated with use of mental health care within primary care. Depression, PTSD, and aggression and the absence of panic were associated with outpatient mental health utilization. Only PTSD was associated with inpatient mental health utilization. Use of the emergency room was not significantly associated with any specific symptoms or behaviors, suggesting that overlap among symptoms drove emergency room utilization.
Discussion
This study is the first to examine a broad range of symptoms and high-risk behaviors as predictors of utilization of various mental health and general medical treatment settings among Iraq and Afghanistan veterans, while controlling for comorbidity. This study is distinguished by use of self-report measures. Previous studies (
4,
11) used diagnoses given by providers, which may be inconsistently recorded and which do not include subthreshold symptoms and are more removed from the subjective distress that propels treatment seeking. When the analysis adjusted for comorbid symptoms, PTSD and depression were the symptoms or behaviors most often associated with treatment utilization across settings. Aggression was associated with use of outpatient mental health care, above and beyond the symptoms of distress that were measured; given the high rates of aggression in this population (
2), this result underscores the need for provider education regarding treatment of aggressive behaviors.
It is important to consider whether patients are receiving treatment in the appropriate setting given their symptoms (
12). The results of the single-symptom analyses suggest that symptoms typically matched services provided in each setting. However, emergency room utilization was broadly associated with psychiatric symptoms that may not require emergency treatment and may be best treated in a specialty mental health setting; outreach and education may help facilitate specialty care engagement. Among veterans who were seen in the emergency room and who reported elevated psychiatric symptoms (N=139), only 36% (N=50) had more than eight specialty mental health visits during the same year. Consistent with prior research (
5), this finding suggests underutilization of specialty mental health services, as do the overall low utilization rates among those with elevated psychiatric symptoms (for example, the mean number of outpatient mental health visits over two years was 8.8).
This study has several strengths, including a clinical sample of veterans enrolled in VA care and a prospective design for assessing symptoms and high-risk behaviors and subsequent treatment utilization. Our sample was limited to veterans receiving treatment at the VAPSHCS or affiliated centers, and the results may not generalize to those not enrolled in VA care or in another VA with different treatment options. In addition, we did not assess for clinical levels of symptoms via diagnoses, and the assessment of pain was limited to a single item.
Conclusions
Various symptoms and high-risk behaviors were differentially associated with treatment utilization across settings. PTSD and depression were the most frequent predictors of utilization. Although veterans largely received care in appropriate treatment settings, they may have been overutilizing the emergency room for mental health concerns and underutilizing specialty mental health services. This study should be replicated at other VA medical centers with different treatment offerings, and future studies should examine characteristics of high treatment utilizers and assess potential moderators (such as gender and deployment status).
Acknowledgments and disclosures
This report is the result of work supported by the VA Puget Sound Health Care System, Seattle.
The authors report no competing interests.