Benzodiazepines have been widely used in clinical practice. Their indications include anxiety, insomnia, and convulsions. They are among the most consumed and prescribed psychotropic agents worldwide (
1–
3). Side effects of abuse of benzodiazepines, especially short-acting benzodiazepines, have been clearly established in recent decades (
4). Furthermore, although the causal relationships are still the subject of debate, a growing body of literature demonstrates that long-term use of benzodiazepines may be associated with cognitive impairment (
5,
6) and an increased incidence of cancer (
7) and mortality (
8,
9). Nonbenzodiazepine hypnotics, such as zopiclone, zolpidem, and zaleplon, have been considered safer than benzodiazepines because they are associated with a lower probability of abuse and dependence (
10). However, compelling evidence suggests that these “z” hypnotics also present a risk of abuse and dependence (
11–
13).
Therefore, it is important to understand the current use of anxiolytics-hypnotics, including benzodiazepines and z hypnotics. The prevalence of anxiolytic-hypnotic use has been investigated in many international epidemiological studies by using clinical interviews. For example, the prevalence of anxiolytic-hypnotic use was 3.5%−3.8% among adults in the United States from 1988 to 2002 (
2), 1.5%−4.3% among the general population of four European countries from 1993 to 1997 (
1), 3.4% in a community sample in Canada in 2000 (
14), and 1.6% among the general population of Thailand in 2007 (
15). A population-based study in Taiwan that used national health insurance claims data indicated that the prevalence of anxiolytic-hypnotic use increased significantly from 1997 (3.0%) to 2004 (7.3%) (
3). However, another study of the same claims data demonstrated a much higher annual prevalence in 2000 (18.6%) (
16). The trend of anxiolytic-hypnotic use may change rapidly, however, and data for the trend in recent years need updating. Moreover, researchers have reported that the likelihood of abuse and toxicity varied between anxiolytics-hypnotic drugs (
17,
18). Nevertheless, none of the previous epidemiological studies investigated the trends in use of individual anxiolytics-hypnotic drugs.
Psychotropic polypharmacy is common in routine psychiatric care (
19,
20) and in the general population as well (
21,
22). Delineating the trend of psychotropic polypharmacy may aid in the evaluation of the risks of adverse effects and drug-drug interactions. A representative survey in the United States found a significant increase in psychotropic polypharmacy by office-based psychiatrists between 1996 and 2006 (
23). This study also suggested that a sedative-hypnotic combination was prescribed less often at Medicare-covered visits than at visits covered by other payers. The risk of adverse effects of this class of drugs, including cognitive impairment and mortality, may be related to their cumulative dose (
24). Thus understanding trends related to anxiolytic-hypnotic polypharmacy is crucial; however, studies investigating this issue are scarce.
The aims of this study were to investigate the trend of prevalence of anxiolytic-hypnotic use in Taiwan between 2002 and 2009 and to determine the trends in use of individual anxiolytics-hypnotic drugs and elucidate the status of anxiolytic-hypnotic polypharmacy during the study period.
Methods
Data source
Data for this study were obtained from the ambulatory claims database of the National Health Insurance Research Database in Taiwan (NHIRD-TW). The National Health Insurance (NHI) program, a compulsory universal health insurance program, was implemented in Taiwan on March 1, 1995. A total of 22.3 million individuals, more than 96% of the population, were enrolled in the NHI program at the end of 2000. Upon the implementation of NHI, the Bureau of NHI became the single payer of health care services. Ninety-three percent of all health care providers have been contracted by the Bureau of NHI. More than 96% of persons enrolled in NHI had used the health care services of contracted hospitals and clinics at least once since 1995. Contracted medical care institutions must submit claim documents for each month’s medical expenses by the 20th day of the following month, if the claims are filed electronically. Information on the electronic claim form includes the patient’s sex, the medical institution visited, diagnostic codes for the prescription, prescription date, drugs prescribed, and medical expense claims.
The institutional review board of Chang Gung Memorial Hospital approved this study. We used a subset of NHIRD-TW, the Longitudinal Health Insurance Database 2000 (LHID2000), which contained the original claims data for one million beneficiaries randomly sampled from the 2000 Registry of Beneficiaries of the NHIRD-TW. Thus the LHID2000 included approximately 5% of the total population. The sex and age distributions in the sample were not significantly different from those in the general population (
19).
Patient selection
We conducted a population-based, random-sample study by using data on anxiolytic or hypnotic drug use between January 1, 2002, and December 31, 2009. Participants received at least one prescription during the study period for any anxiolytic or hypnotic, whether documented as an ambulatory care, pharmacy, or hospital care claim. The amount of drug use was calculated for each calendar year and each season. Drugs were identified as anxiolytics or hypnotics by using the Anatomical Therapeutic Chemical (ATC) classification system (
25). Data are presented for 24 benzodiazepines (alprazolam, bromazepam, brotizolam, chlordiazepoxide, clobazam, clonazepam, clorazepate, cloxazolam, diazepam, estazolam, fludiazepam, flunitrazepam, flurazepam, lorazepam, lormetazepam, medazepam, midazolam, nimetazepam, nitrazepam, nordazepam, oxazepam, oxazolam, prazepam, and triazolam) and three z hypnotic agents (zaleplon, zolpidem, and zopiclone). These medications are classed as restricted drugs by the Bureau of NHI in Taiwan. Restricted drugs are available only with a physician’s assessment and prescription. Therefore, anxiolytics-hypnotics are not available over the counter, and any prescription of these drugs would be documented in NHIRD-TW.
Statistical analyses
This study focused on the temporal changes in the use of anxiolytic-hypnotic agents between 2002 and 2009. We analyzed drugs that were administered orally, intravenously, or intramuscularly. In addition, we analyzed chlordiazepoxide in single and compound form, given that it is a common component of compound drug treatment for gastrointestinal diseases in Taiwan. To determine the proportion of participants with a history of drug use, we divided the number of participants with any record of anxiolytic-hypnotic use by the total number of participants in the study sample during each year and season. Furthermore, we calculated the total sum of days with reported drug use across all individuals (person-days) in order to understand the duration of anxiolytic-hypnotic use. For example, if one patient used two anxiolytic drugs (drug A and drug B) in the same day, we counted one person-day for drug A and one person-day for drug B. To determine the proportion of person-days, we divided the number of person-days of drug use by the total number of person-days in each year. The distribution of polypharmacy was assessed by determining the number of person-days with reported use of a single drug, two drugs, and three or more drugs. The proportion of polypharmacy was defined as the number of person-days with polypharmacy divided by the total number of person-days with any anxiolytic-hypnotic use. We calculated the number of persons, the number of person-days, and the distribution of polypharmacy for each year and season.
In the preliminary analyses, the prevalence rates of brotizolam, clobazam, clorazepate, cloxazolam, flunitrazepam (intramuscular form), lormetazepam, medazepam, nimetazepam, nordazepam, oxazepam, and zaleplon were less than .1% during the entire study period. Thus the data for these drugs were not further analyzed or shown individually. However, the number of users of these drugs and the number of days that these drugs were used were included in calculations of the total count of persons and person-days with any anxiolytic-hypnotic drug use and of the distribution of polypharmacy. Only the data from the remaining 19 drugs, including alprazolam, bromazepam, chlordiazepoxide (single and combination forms), clonazepam, diazepam (oral and intramuscular forms), estazolam, flunitrazepam (oral form), flurazepam, lorazepam (oral and intramuscular forms), midazolam (oral and intramuscular forms), nitrazepam, oxazolam, triazolam, zolpidem, and zopiclone, were included in analyses of individual drugs.
Time-series analysis was performed for each season by using the same parameters (persons, person-days, and distribution of polypharmacy). Linear models were used to assess trends in the prevalence of use of each anxiolytic-hypnotic, including trends related to number of persons, person-days, and frequency of anxiolytic-hypnotic polypharmacy. All statistical analyses were performed by using the Statistical Analysis System, version 9.1. All tests were two-tailed, and the level of significance was p<.05.
Results
The annual prevalence of use of any anxiolytic-hypnotic was 23.5% in 2002 and 22.2% in 2009, and the prevalence did not significantly change over the study period (
Table 1). Drug-specific analyses showed that chlordiazepoxide (combination form) had the highest annual prevalence of use (9.2% in 2002 and 8.4% in 2009), followed by diazepam (oral form) (8.3% and 5.7%). Increases in prevalence from 2002 to 2009 were most significant for clonazepam (.7% and 1.8%, p<.001), zolpidem (2.4% and 4.2%, p<.001), and estazolam (1.3% and 1.7%, p<.001). Decreases in prevalence were most significant for triazolam (.3% and .2%, p<.001), the single form of chlordiazepoxide (.7% and .4%, p<.001), and oxazolam (3.4% and 2.3%, p<.001).
The proportion of person-days of use of any anxiolytic-hypnotic increased significantly from 2002 (4.0%) to 2009 (6.6%) (t=45.14, df=31, p<.001). To avoid the potential influence of natural aging of the population in the claims database, we further analyzed the percentages for the population age nine and older. As a result, the proportion of person-days of use of any anxiolytic-hypnotic still showed a significantly increasing trend (from 4.4% in 2002 to 6.8% in 2009, t=22.80, df=31, p<.001). Twelve of the 19 drugs analyzed showed a significant increasing trend in person-days over the study period (
Table 2). The trend toward increased person-days was most significant for clonazepam (.2% and .6%, p<.001), zolpidem (.5% and 1.5%, p<.001), and alprazolam (.6% and 1.1%, p<.001). The trend toward decreased person-days was most significant for the single form of nitrazepam (.03% and .02%, p<.001), chlordiazepoxide (single form) (.03% and .02%, p<.001), and diazepam (intravenous or intramuscular form) (.01% and .007%, p<.001).
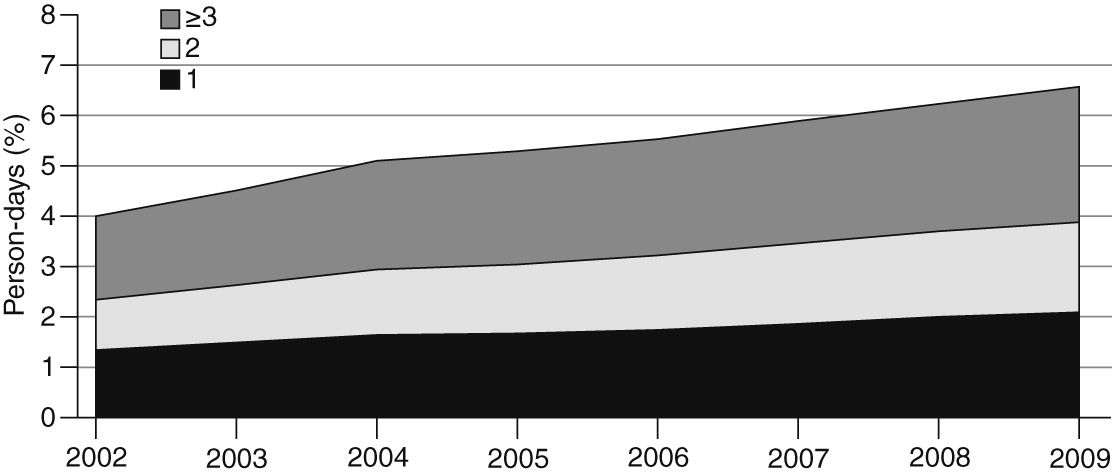
Figure 1 illustrates the proportion of person-days by number of anxiolytics-hypnotics used simultaneously between 2002 and 2009. Person-days of use of one drug (1.3% and 2.1%, p<.001), two drugs (1.0% and 1.8%, p<.001), and three or more drugs (1.7% and 2.7%, p<.001) increased significantly. Approximately 30% of the total person-days during the study period were related to single-drug use. Anxiolytic-hypnotic polypharmacy accounted for the remaining 70% (about 30% related to the use of two drugs and about 40% related to the use of three or more drugs).
Discussion
More than 20% of participants had some record of having used an anxiolytic-hypnotic during the study period. Previous international studies reported a much lower annual prevalence—less than 5% (
1,
2,
14,
15). Notably, these studies determined anxiolytic-hypnotic use by clinical interviews; therefore, the results may be influenced by underestimation and reporting bias. However, two previous investigations in Taiwan also reported prevalence rates lower than those we reported (
3,
16). These discrepancies may be due to variations in the methods. These two studies did not describe details about the anxiolytics-hypnotics used in intravenous, intramuscular, or compound medicines form. We found that the compound form of chlordiazepoxide had the highest prevalence (mean prevalence of more than 8%). Chlordiazepoxide is a component of many compound gastrointestinal drugs in Taiwan. Thus many patients may not know that they are taking a medication containing an anxiolytic-hypnotic. We suspect that data previously reported by other researchers may have underestimated use of anxiolytics-hypnotics because they did not include use of all forms of the drugs. The results of this study suggest that the annual prevalence of any anxiolytic-hypnotic use may be much higher than previously reported if those analyses included all forms of drugs.
The proportion of person-days of any anxiolytic-hypnotic drug use ranged from 4.0% to 6.6% during the study period. Patients do not necessarily use this class of drugs continuously. Thus it is reasonable that the proportion of person-days of anxiolytic-hypnotic use was less than the proportion of persons having any record of anxiolytic-hypnotic use. The proportion of person-days may be a more accurate and suitable index of drug use than the proportion of persons. The results of this study showed a significant increasing trend in the proportion of person-days of anxiolytic-hypnotic use, whereas the proportion of participants with any anxiolytic-hypnotic use did not significantly increase. Possible explanations for this phenomenon include an increase in the prevalence of common mental disorders in Taiwan within the past decade (
26). Therefore, the proportion of the population who required long-term drug use or polypharmacy involving anxiolytics-hypnotics probably increased in recent years. Moreover, previous study of epidemiology had demonstrated that older individuals tended to be long-term regular users of anxiolytics (
27). Population aging, which is a serious public health issue in Taiwan, may also be associated with the increasing trend in the number of person-days with anxiolytic-hypnotic use. However, stratification analysis for age and sex was not performed in this study, and further investigations are warranted to confirm these speculations.
The compound forms of chlordiazepoxide, the oral forms of diazepam and lorazepam, and alprazolam are the most commonly used anxiolytics-hypnotics in Taiwan. Diazepam, lorazepam, and alprazolam are very familiar to the health care providers in Taiwan, and they are the most commonly prescribed drugs among a variety of benzodiazepines. However, there is some evidence that these drugs may be more likely to be abused than other anxiolytics-hypnotics (
18,
28). Clonazepam and zolpidem were associated with the most significant trends toward greater number of users and number of person-days. Clonazepam is widely used for a variety of clinical indications, including insomnia, anxiety, convulsions, and even restless legs syndrome (
29,
30). Furthermore, the use of zolpidem has also rapidly increased, and the proportion of person-days of zolpidem use (1.5%) was greater than the proportion of person-days of all other anxiolytics-hypnotics in 2009. Nevertheless, we did not analyze the indication for the prescription and the optimal dose or duration of anxiolytic-hypnotic use. Therefore, the appropriateness of using these drugs could not yet be fully understood from the information we used.
A review article regarding benzodiazepine dependence indicated that chlordiazepoxide, diazepam, and nitrazepam were the first three drugs in this class introduced in the United Kingdom (
31). The sequence of benzodiazepines’ entry into the market was similar in Taiwan and the United Kingdom. Notably, the results of this study showed that decreases in the trends in person-days were most significant for these three drugs. One possible explanation is that because these drugs have expired patents, they are not promoted by the pharmaceutical companies and are therefore less likely to be prescribed. Another possibility is that chlordiazepoxide, diazepam, and nitrazepam are long-acting benzodiazepines, so they have relatively less potential for dependence and continuous use than other anxiolytics-hypnotics. In addition, antidepressant drugs and second-generation antipsychotics might be treated as substitutes for benzodiazepines in some clinical conditions because of their anxiolytic or hypnotic effects (
2). It is noteworthy that there were significant increasing trends in the rate of treatment with antidepressants and second-generation antipsychotics in the United States over the past years (
23). A similar phenomenon had been also noted in Taiwan (
3). Nevertheless, the trends in the use of other psychotropic drugs were not analyzed in this study. The mechanism by which the consumption of anxiolytics-hypnotics is affected by other psychotropic drugs warrants further clarification.
Previously, polypharmacy was often evaluated by merely counting the number of medications used per person in a certain period (
32). However, delineating the trend of person-days by the number of anxiolytics-hypnotics used simultaneously may render a more complete picture of the status of polypharmacy. In this study, the proportion of person-days of combined anxiolytic-hypnotic use significantly increased from 2002 to 2009. Polypharmacy accounted for almost 70% of the person-days of anxiolytic-hypnotic use. Polypharmacy regimens may be attributed to the physician’s prescription (
23,
33), the patient’s request, or the behavior of shopping for doctors (
34). Nevertheless, the results from this study could not distinguish the source of polypharmacy regimens. Notably, a previous report indicated that addiction to benzodiazepines can occur even when doses are within the clinical range as long as they are taken regularly over six months (
35). Because there is growing concern over the potential risk of anxiolytics-hypnotics, it is important to reduce unnecessary exposure to polypharmacy regimens.
This study had several limitations. First, the findings demonstrate trends only in use of anxiolytics-hypnotics. Important information regarding medications, such as the indications and the providers, was not analyzed. Second, the trend toward increasing anxiolytic-hypnotic use would be associated with a variety of causes, such as increasing incidence of psychiatric disorders; it does not necessarily represent exorbitant use. Similarly, the significant increasing trends in the use of some medications, such as clonazepam and zolpidem, may be due to their greater potential for abuse, better effectiveness, or popularity among physicians. Further investigation of these issues is warranted. Third, this study used a sample randomly selected from the 2000 Registry of Beneficiaries of the NHIRD-TW, so that the distribution of age would naturally increase during the study period. Therefore, the trend toward increased use of anxiolytics-hypnotics might be overestimated.
Fourth, there are differences between the health care system of Taiwan and that of other countries. The NHI program in Taiwan is a compulsory health insurance system with low copayments, and a large percentage of the population is enrolled. This system may encourage more persons to seek treatment, resulting in higher health care services utilization. Moreover, the study design, sampling methods, and definition of anxiolytic-hypnotic use differed among studies investigating similar topics. Direct comparisons with previous international studies may not be feasible. Finally, although anxiolytics-hypnotics are classified as restricted drugs by the Bureau of NHI in Taiwan, where drug compliance is documented, the number of individuals who acquired over-the-counter drugs from the black market or from their family and friends was unavailable for analyses in the NHIRD-TW. These issues might influence the accuracy of estimation in this study.
Despite its limitations, this study had some strengths. First, the nationwide, population-based, random nature of the sample would avoid selection bias. The longitudinal data are reliable for detecting trends and prevalence of drug use, warding off the possibility of recall bias. Second, we analyzed anxiolytic-hypnotic use and polypharmacy by person-days, which more accurately demonstrate the trend than the number of persons who used the drug during a defined period. Furthermore, to our knowledge, we are among the first to contribute evidence about the longitudinal trends in use of individual anxiolytic-hypnotic drugs.