Risk of Hospitalization and Use of First- Versus Second-Generation Antipsychotics Among Nursing Home Residents
Abstract
Objective
Methods
Results
Conclusions
Methods
Data sources
Study design and sample
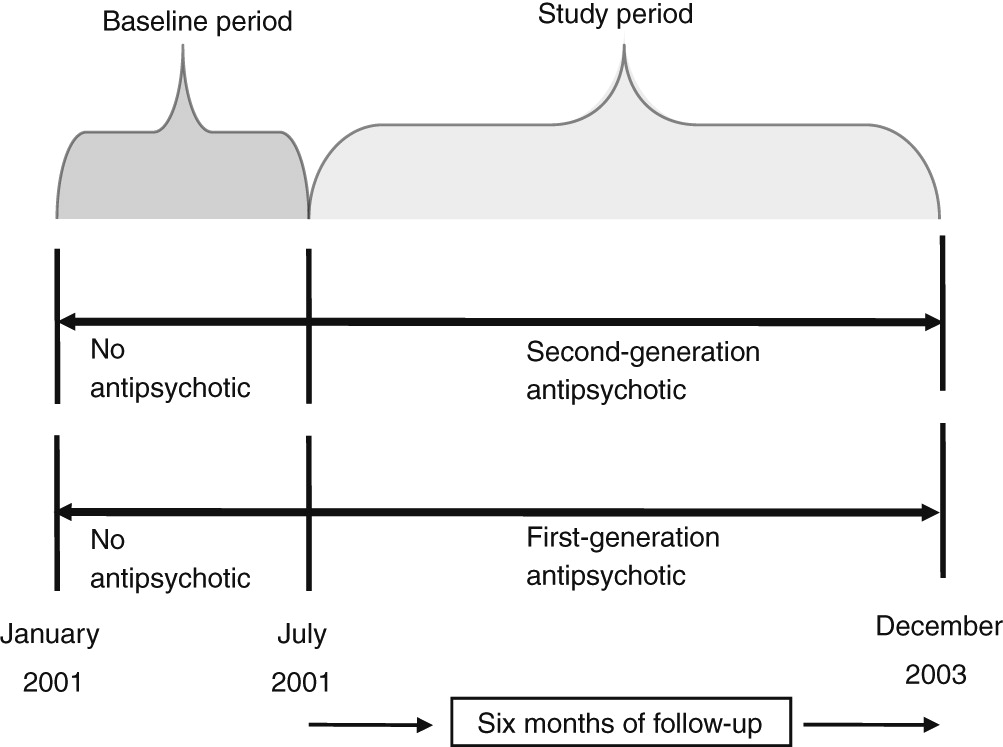
Exposure and outcome definitions
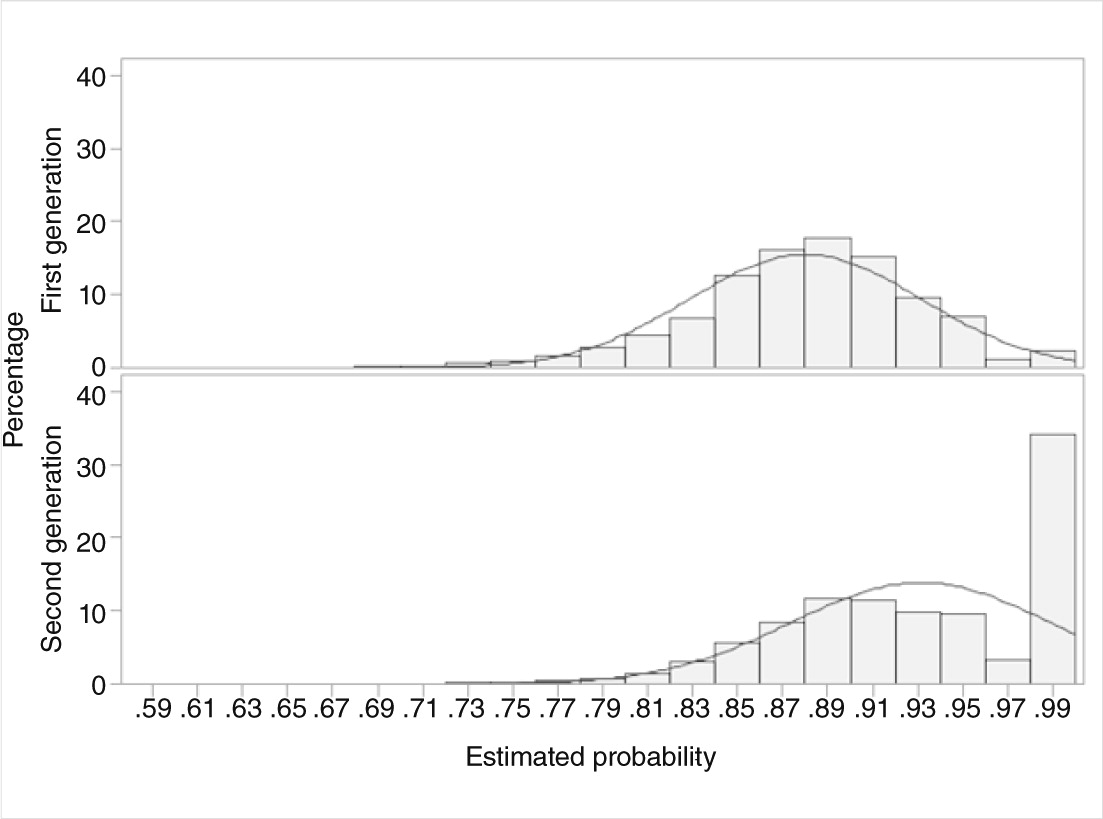
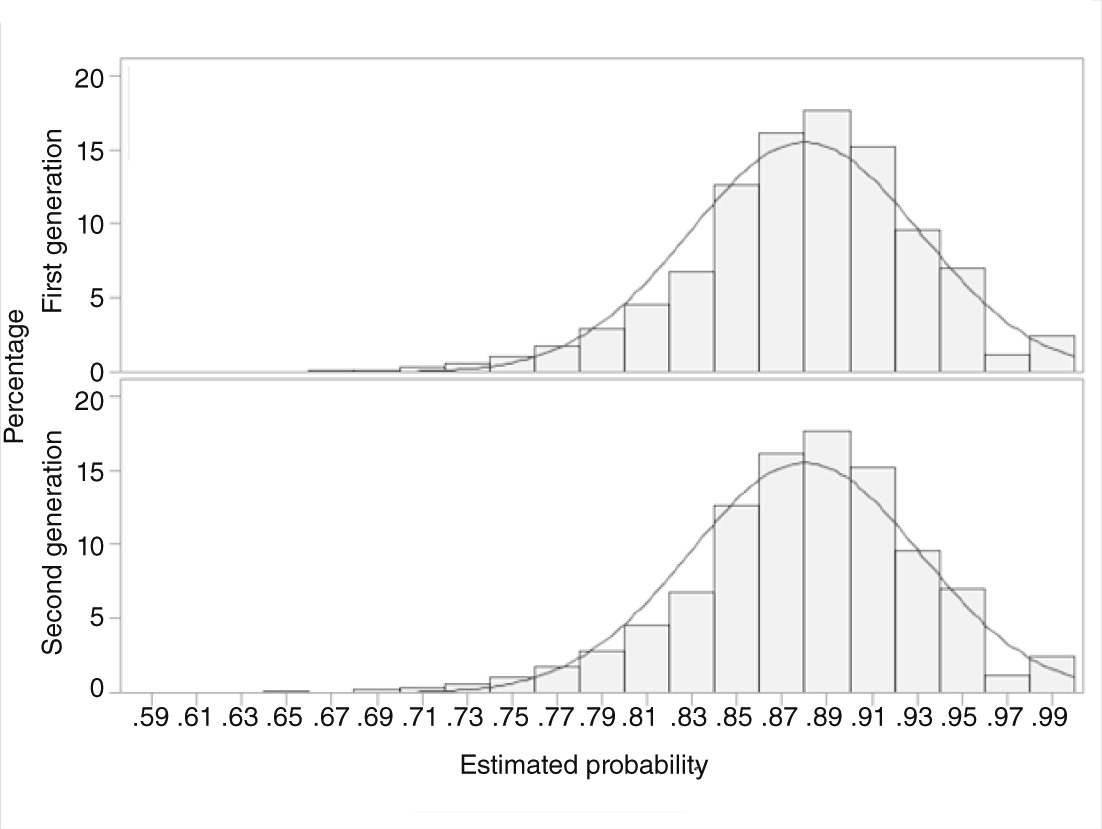
Propensity-score matching
Statistical analysis
Results
Matching process and patient characteristics
| Unmatched (N=49,904) | Matched (N=7,218) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Secondgeneration(N=46,293) | Firstgeneration(N=3,611) | Secondgeneration(N=3,609) | Firstgeneration(N=3,609) | |||||||
| Characteristic | N | % | N | % | p | N | % | N | % | p |
| Age (M±SD) | 83.57±8.0 | 83.06±8.3 | <.001 | 82.97±8.3 | 83.05±8.3 | .71 | ||||
| Gender | <.001 | .98 | ||||||||
| Male | 13,048 | 28.2 | 1,267 | 35.1 | 1,267 | 35.1 | 1,266 | 35.1 | ||
| Female | 33,245 | 71.8 | 2,344 | 64.9 | 2,342 | 64.9 | 2,343 | 64.9 | ||
| Race | <.001 | .64 | ||||||||
| White | 31,207 | 67.4 | 2,264 | 62.7 | 2,223 | 61.6 | 2,262 | 62.7 | ||
| Black | 5,161 | 11.2 | 535 | 14.8 | 550 | 15.2 | 535 | 14.8 | ||
| Others | 9,925 | 21.4 | 812 | 22.5 | 836 | 23.2 | 812 | 22.5 | ||
| Hospitalization | <.001 | .86 | ||||||||
| Yes | 10,990 | 23.7 | 1,047 | 29.0 | 1,040 | 28.8 | 1,047 | 29.0 | ||
| No | 35,303 | 76.3 | 2,564 | 71.0 | 2,569 | 71.2 | 2,562 | 71.0 | ||
| Region | <.001 | |||||||||
| New York | 15,772 | 34.1 | 88 | 2.4 | 88 | 2.4 | 88 | 2.4 | ||
| Florida | 7,810 | 16.9 | 1,447 | 40.1 | 1,387 | 38.3 | 1,445 | 40.4 | ||
| California | 9,816 | 21.2 | 473 | 13.1 | 482 | 13.4 | 473 | 13.1 | ||
| Texas | 12,895 | 27.9 | 1,603 | 44.4 | 1,659 | 45.9 | 1,603 | 44.4 | ||
| Year of cohort entry | <.001 | .48 | ||||||||
| 2001 | 34,337 | 74.2 | 2,902 | 80.4 | 2,867 | 79.4 | 2,900 | 80.4 | ||
| 2002 | 10,963 | 23.7 | 647 | 17.9 | 669 | 18.5 | 647 | 17.9 | ||
| 2003 | 993 | 2.2 | 62 | 1.8 | 73 | 2.0 | 62 | 1.0 | ||
| Medical history | ||||||||||
| Hypertension | 10,660 | 23.0 | 1,061 | 29.4 | <.001 | 1,099 | 30.5 | 1,061 | 29.4 | .32 |
| Coronary heart disease | 3,832 | 8.3 | 321 | 8.9 | <.001 | 336 | 9.3 | 321 | 8.9 | .54 |
| Congestive heart failure | 6,373 | 13.8 | 668 | 18.5 | <.001 | 685 | 19.0 | 668 | 18.5 | .61 |
| Acute myocardial infarction | 708 | 1.5 | 76 | 2.1 | .007 | 75 | 2.1 | 76 | 2.1 | .93 |
| Cardiac arrhythmias | 3,258 | 7.0 | 305 | 8.5 | .001 | 302 | 8.4 | 305 | 8.5 | .97 |
| Circulatory disorder | 2,220 | 4.8 | 203 | 5.6 | .03 | 196 | 5.4 | 203 | 5.6 | .72 |
| Thromboembolic disorder | 569 | 1.2 | 47 | 1.3 | .70 | 41 | 1.1 | 47 | 1.3 | .52 |
| Diabetes | 5,541 | 12.0 | 535 | 14.8 | <.001 | 574 | 15.9 | 535 | 14.8 | .20 |
| Cerebrovascular disease | 5,356 | 11.6 | 589 | 16.3 | <.001 | 580 | 15.5 | 589 | 16.3 | .35 |
| Hip or femur fracture | 2,099 | 4.5 | 163 | 4.5 | .95 | 165 | 4.6 | 163 | 4.5 | .91 |
| Chronic obstructive pulmonary disorder | 3,766 | 8.1 | 382 | 10.6 | <.001 | 355 | 9.8 | 382 | 10.6 | .30 |
| Falls | 131 | .3 | 16 | .4 | .08 | 15 | .4 | 16 | .4 | .86 |
| Thyroid disorder | 4,841 | 10.1 | 482 | 13.4 | <.001 | 502 | 13.9 | 480 | 13.3 | .45 |
| Renal failure | 1,235 | 2.7 | 155 | 4.3 | <.001 | 164 | 4.5 | 155 | 4.3 | .60 |
| Other renal disorder | 4,970 | 10.7 | 468 | <.001 | 459 | 12.7 | 468 | 13.0 | .75 | |
| Liver disorder | 486 | 1.1 | 42 | 1.2 | .52 | 40 | 1.1 | 42 | 1.2 | .82 |
| Gastric disorder | 5,903 | 12.8 | 585 | 16.2 | <.001 | 557 | 15.4 | 585 | 16.2 | .37 |
| Ulcers | 1,748 | 3.8 | 171 | 4.7 | .004 | 180 | 5.0 | 171 | 4.7 | .62 |
| Cancer (any type) | 1,250 | 2.7 | 144 | 4.0 | <.001 | 146 | 4.1 | 144 | 4.0 | .90 |
| Cataract | 138 | .3 | 9 | .3 | .60 | 9 | .3 | 9 | .3 | .99 |
| Glaucoma | 525 | 1.1 | 44 | 1.2 | .65 | 48 | 1.3 | 44 | 1.2 | .68 |
| Anemia | 3,097 | 6.7 | 292 | 8.1 | .001 | 296 | 8.2 | 292 | 8.1 | .86 |
| Osteoporosis | 1,418 | 3.1 | 115 | 3.2 | .68 | 115 | 3.2 | 115 | 3.2 | .99 |
| Rheumatoid arthritis | 231 | .5 | 14 | .4 | .36 | 17 | .5 | 14 | .4 | .59 |
| Back pain | 628 | 1.4 | 47 | 1.3 | .79 | 45 | 1.3 | 47 | 1.3 | .83 |
| Dyslipidemia | 832 | 1.8 | 75 | 2.1 | .23 | 72 | 2.0 | 72 | 2.0 | .80 |
| Obesity | 188 | .4 | 21 | .6 | .12 | 21 | .6 | 21 | .6 | .99 |
| HIV infection | 21 | .1 | 2 | .1 | .68 | 4 | .1 | 2 | .1 | .68 |
| Pneumonia | 2,905 | 6.3 | 323 | 8.9 | <.001 | 308 | 8.5 | 323 | 8.9 | .53 |
| Parkinson’s disease | 1,212 | 2.6 | 82 | 2.3 | .21 | 86 | 2.4 | 82 | 2.3 | .75 |
| Endocarditis | 366 | .8 | 41 | 1.1 | .03 | 26 | .7 | 41 | 1.1 | .06 |
| Substance use disorder | 530 | 1.1 | 51 | 1.4 | .15 | 50 | 1.4 | 51 | 1.4 | .92 |
| Extrapyramidal symptoms | 103 | .2 | 13 | .4 | .10 | 8 | .2 | 13 | .4 | .27 |
| Dementia | 10,568 | 22.8 | 923 | 25.6 | <.001 | 968 | 26.8 | 923 | 25.6 | .23 |
| Schizophrenia | 2,447 | 5.3 | 206 | 5.7 | .28 | 210 | 5.8 | 206 | 5.7 | .84 |
| Anxiety disorder | 1,293 | 2.8 | 122 | 3.4 | .04 | 112 | 3.1 | 122 | 3.4 | .51 |
| Conduct disorder | 60 | .1 | 2 | .1 | .32 | 3 | .1 | 2 | .1 | .99 |
| Mood disorder | 4,377 | 9.5 | 319 | 8.8 | .22 | 321 | 8.9 | 319 | 8.8 | .93 |
| Other mental disorders | 805 | 1.7 | 86 | 2.4 | .005 | 89 | 2.4 | 86 | 2.4 | .82 |
| Other drugs used | ||||||||||
| Cardiovascular | 19,689 | 42.5 | 2,095 | 58.0 | <.001 | 2,119 | 58.7 | 2,094 | 58.0 | .55 |
| Antidiabetics | 6,399 | 13.8 | 737 | 20.4 | <.001 | 773 | 21.4 | 737 | 20.4 | .30 |
| Analgesic | 13,331 | 28.8 | 1,420 | 39.3 | <.001 | 1,414 | 39.2 | 1,419 | 39.3 | .90 |
| Estrogen | 1,679 | 3.6 | 150 | 4.2 | .10 | 139 | 3.9 | 150 | 4.2 | .51 |
| Antihistamine | 5,066 | 10.9 | 609 | 16.9 | <.001 | 588 | 16.3 | 609 | 16.9 | .51 |
| Antiasthmatics | 4,580 | 9.9 | 582 | 16.1 | <.001 | 549 | 15.2 | 582 | 16.1 | .29 |
| Anti-infective | 15,457 | 33.4 | 1,724 | 47.7 | <.001 | 1,786 | 49.5 | 1,723 | 47.7 | .14 |
| Diuretic | 10,961 | 23.7 | 1,183 | 32.8 | <.001 | 1,226 | 34.0 | 1,182 | 32.8 | .27 |
| Anticancer | 2,843 | 6.1 | 310 | 8.6 | <.001 | 319 | 8.8 | 310 | 8.6 | .71 |
| Anticholinergic | 2,407 | 5.2 | 332 | 9.2 | <.001 | 298 | 8.3 | 332 | 9.2 | .16 |
| Ophthalmic | 6,140 | 13.3 | 687 | 19.0 | <.001 | 697 | 19.3 | 686 | 19.0 | .74 |
| Antithyroid | 4,841 | 9.7 | 482 | 13.4 | <.001 | 502 | 13.9 | 480 | 13.3 | .45 |
| Antismoking | 23 | .1 | 1 | .0 | .99 | 3 | .1 | 1 | .0 | .62 |
| Endocrine and metabolic agent | 178 | .4 | 19 | .5 | .19 | 19 | .5 | 19 | .5 | .99 |
| Hypnotic | 4,788 | 10.3 | 471 | 13.0 | <.001 | 453 | 12.6 | 471 | 13.1 | .53 |
| Antidepressant | 14,631 | 31.6 | 1,264 | 35.0 | <.001 | 1,322 | 36.6 | 1,262 | 35.0 | .15 |
| Anticonvulsant | 5,955 | 12.9 | 539 | 14.9 | <.001 | 548 | 15.2 | 539 | 14.9 | .77 |
| Lithium | 105 | .2 | 7 | .2 | .69 | 10 | .3 | 7 | .2 | .46 |
| Antianxiety | 7,983 | 17.2 | 866 | 24.0 | <.001 | 885 | 24.5 | 865 | 24.0 | .58 |
| Stimulant | 131 | .3 | 6 | .2 | .25 | 12 | .3 | 6 | .2 | .24 |
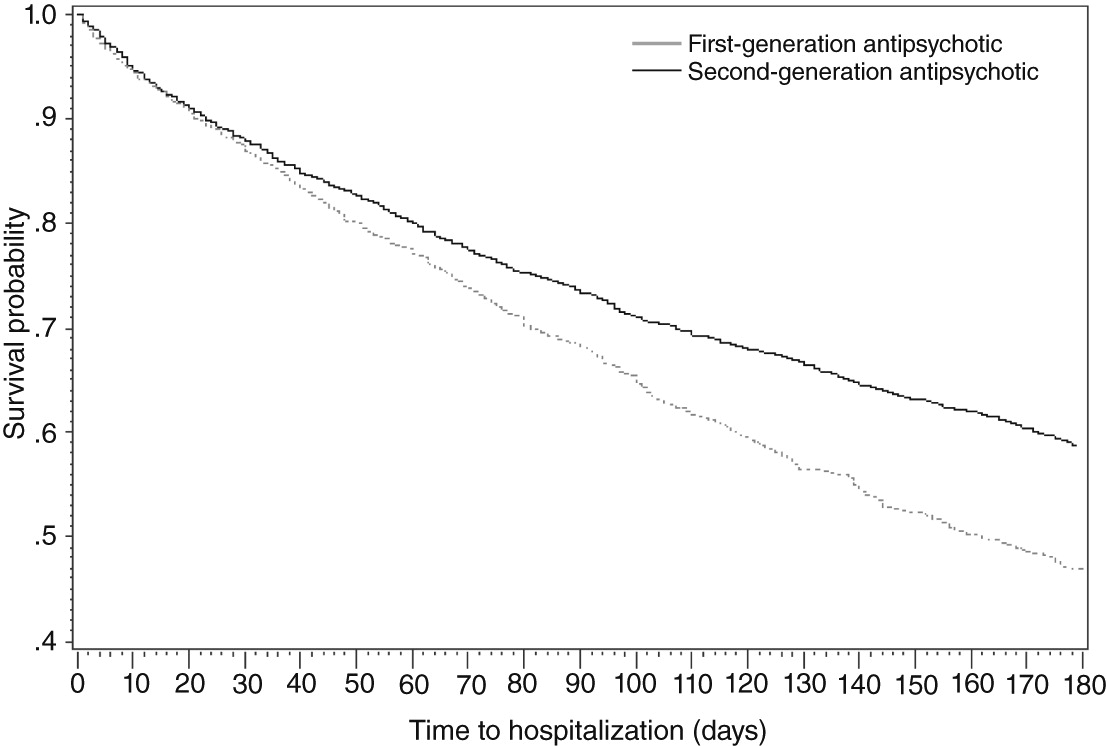
Risk of all-cause hospitalization
Discussion
Conclusions
Acknowledgments and disclosures
Supplementary Material
- View/Download
- 37.04 KB
References
Information & Authors
Information
Published In


Cover: Griselda, by Maxfield Parrish. © Copyright 2014 National Museum of American Illustration™, Newport, Rhode Island. Photos courtesy of Archives of the American Illustrators Gallery™, New York City.
History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).