A Multiple-City RCT of Housing First With Assertive Community Treatment for Homeless Canadians With Serious Mental Illness
Abstract
Objective:
Methods:
Results:
Conclusions:
Methods
Study Design
Study Population
Study Interventions
Housing First.
Treatment as usual.
Randomization
Study Outcomes
Sample Size and Statistical Analysis
Results
Study Participants
| Housing First (N=469) | Treatment as usual (N=481) | Total (N=950) | ||||
|---|---|---|---|---|---|---|
| Characteristic | N | % | N | % | N | % |
| Age (M±SD) | 38.93±10.81 | 39.86±11.22 | 39.40±11.03 | |||
| Male | 319 | 68 | 329 | 68 | 648 | 68 |
| Member of racial or ethnic minority group | 95 | 20 | 103 | 21 | 198 | 21 |
| Aboriginal | 91 | 19 | 90 | 19 | 181 | 19 |
| Never married | 342 | 73 | 356 | 74 | 698 | 73 |
| Not a high school graduate | 272 | 58 | 289 | 60 | 561 | 59 |
| >24 months lifetime homelessness | 191 | 60 | 200 | 58 | 391 | 59 |
| Longest period homeless >1 year | 240 | 51 | 242 | 50 | 482 | 51 |
| Current psychiatric conditionb | ||||||
| Major depressive episode | 204 | 42 | 208 | 44 | 412 | 43 |
| Mania or hypomania episode | 78 | 16 | 75 | 16 | 153 | 16 |
| Posttraumatic stress disorder | 122 | 25 | 134 | 29 | 256 | 27 |
| Panic disorder | 94 | 20 | 109 | 23 | 203 | 21 |
| Mood disorder with psychotic features | 94 | 20 | 100 | 21 | 194 | 20 |
| Psychotic disorder | 242 | 50 | 250 | 53 | 492 | 52 |
| Substance-related problems | 333 | 71 | 359 | 75 | 692 | 73 |
| Chronic health conditions (M±SD) | 4.80±3.67 | 4.99±3.74 | 4.89±3.70 | |||
| ≥2 hospitalizations for mental illness in past 5 years | 238 | 51 | 261 | 54 | 499 | 53 |
| Past-year arrest | 151 | 32 | 160 | 33 | 311 | 33 |
| Victimization in past 6 months | 268 | 57 | 289 | 60 | 557 | 59 |
Primary Outcomes
| Housing First (N=320–469) | Treatment as usual (N=178–481) | |||
|---|---|---|---|---|
| Outcome | M | SD | M | SD |
| Days to moving into first housing | 72.92 | 95.99 | 219.70 | 193.32 |
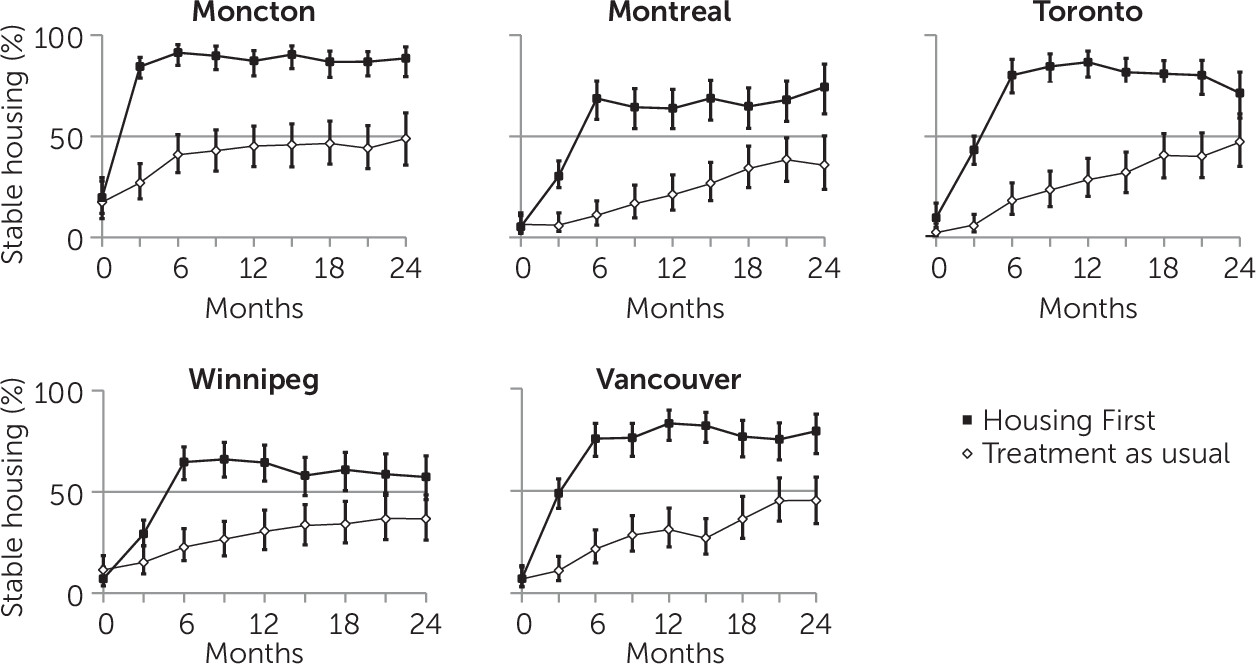
| Percentage of time housed in previous 3 months | ||||
| Baseline | 10.78 | 27.16 | 8.64 | 25.03 |
| 3 months | 47.76 | 37.53 | 12.81 | 29.68 |
| 6 months | 76.07 | 37.98 | 22.56 | 38.07 |
| 9 months | 76.43 | 38.81 | 27.34 | 41.80 |
| 12 months | 77.23 | 37.93 | 30.69 | 43.55 |
| 15 months | 76.59 | 39.11 | 32.45 | 44.45 |
| 18 months | 74.23 | 40.81 | 37.87 | 45.88 |
| 21 months | 73.85 | 41.04 | 45.88 | 46.99 |
| Final follow-up | 72.60 | 42.81 | 41.79 | 47.61 |
| Days housed at final interview | 280.74 | 278.92 | 115.33 | 191.43 |
| Perceived housing qualitya | ||||
| 6 months | 20.21 | 4.30 | 17.20 | 5.57 |
| 12 months | 20.55 | 3.97 | 17.96 | 5.05 |
| 18 months | 19.76 | 4.21 | 19.06 | 4.51 |
| 21 or 24 months | 19.97 | 4.26 | 18.99 | 4.77 |
| MCAS community functioningb | ||||
| Baseline | 54.43 | 7.38 | 54.21 | 7.21 |
| 6 months | 60.97 | 8.76 | 59.07 | 8.82 |
| 12 months | 62.46 | 8.66 | 60.34 | 9.09 |
| 18 months | 62.53 | 8.86 | 60.74 | 9.59 |
| 21 or 24 months | 62.53 | 9.29 | 61.04 | 9.75 |
Secondary Outcomes
| Housing First (N=354–467) | Treatment as usual (N=312–481) | |||
|---|---|---|---|---|
| Outcome | M | SD | M | SD |
| QoLI-20 quality of lifea | ||||
| Baseline | 73.99 | 22.71 | 72.39 | 23.84 |
| 21 or 24 months | 89.38 | 22.45 | 87.16 | 22.57 |
| Community Integration Scale | ||||
| Physical integrationb | ||||
| Baseline | 1.95 | 1.71 | 1.97 | 1.68 |
| 21 or 24 months | 1.81 | 1.60 | 2.00 | 1.74 |
| Psychological integrationc | ||||
| Baseline | 10.89 | 3.79 | 10.76 | 3.87 |
| 21 or 24 months | 12.85 | 3.34 | 12.75 | 3.60 |
| EQ-5D health statusd | ||||
| Baseline | 0.64 | .24 | 0.62 | .24 |
| 21 or 24 months | 0.70 | .24 | 0.72 | .24 |
| CSI mental health symptomse | ||||
| Baseline | 39.87 | 12.89 | 40.81 | 12.62 |
| 21 or 24 months | 32.57 | 11.79 | 31.49 | 12.54 |
| GAIN substance use problems (symptoms)f | ||||
| Baseline | 1.93 | 1.88 | 1.95 | 1.89 |
| 21 or 24 months | 1.47 | 1.78 | 1.31 | 1.73 |
Costs
Discussion
Conclusions
Acknowledgments
Footnotes
Supplementary Material
- View/Download
- 77.06 KB
References
Information & Authors
Information
Published In
Cover: Bowl, by Louis Comfort Tiffany, circa 1908. Favrile glass. Gift of Louis Comfort Tiffany Foundation, 1951 (51.121.13). Metropolitan Museum of Art, New York City. Image copyright © The Metropolitan Museum of Art. Image source: Art Resource, New York City.
History
Authors
Competing Interests
Funding Information
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
PDF/EPUB
View PDF/EPUBLogin options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).