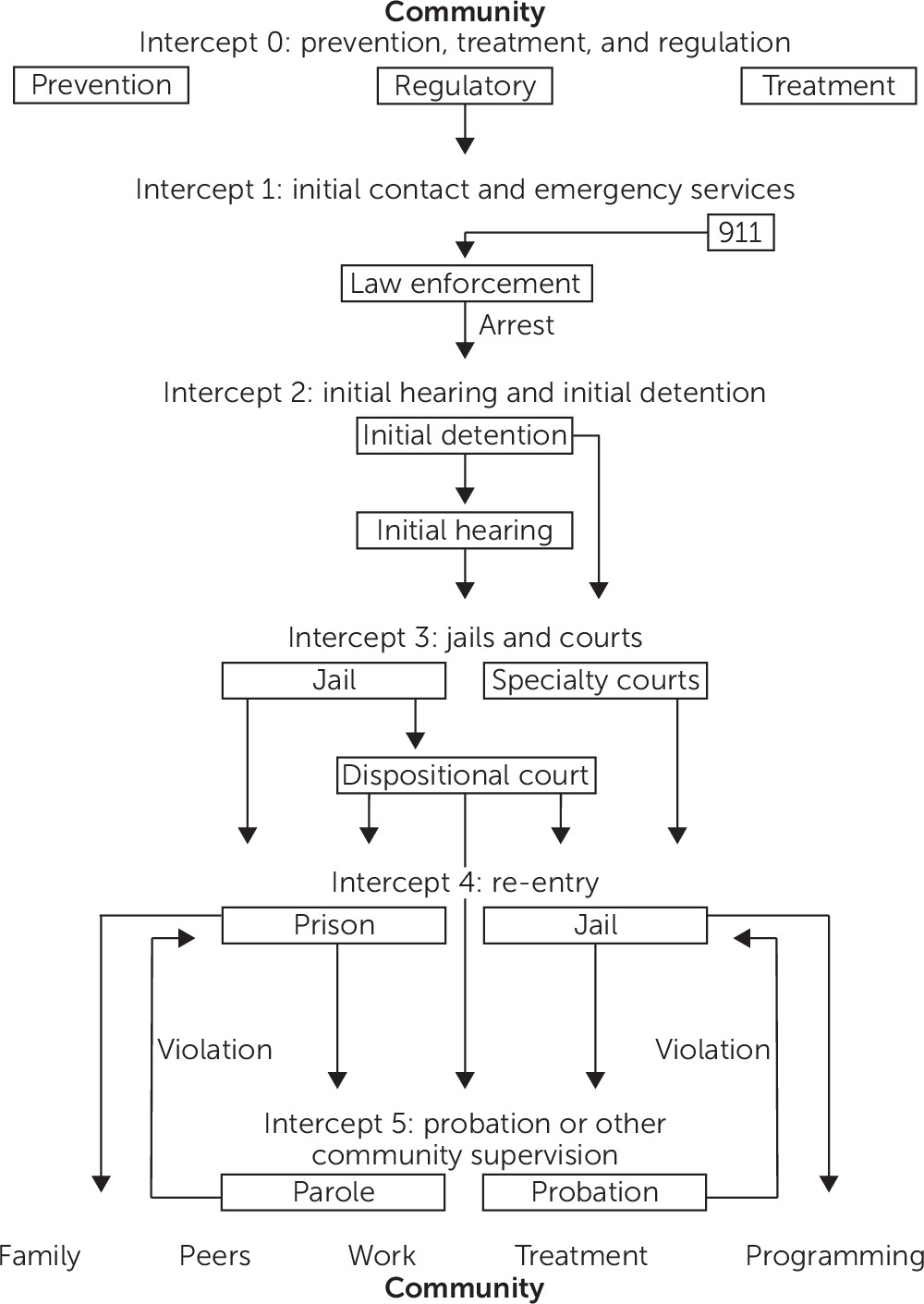
The sequential intercept model is a systems-level framework for criminal justice, mental health, and addictions stakeholders to divert adults with serious mental illness from the criminal justice system to community mental health and addictions services. This framework identifies points where individuals with serious mental illness move through the criminal justice system, each of which offer diversion opportunities (
1). These intercept points include crisis services and law enforcement (intercept 1), detainment and initial hearing (intercept 2), jail and court-based programs (intercept 3), re-entry (intercept 4), and community supervision and support (intercept 5). The goal is that people with mental illness will be intercepted at the earliest point in the criminal justice system and diverted to needed community-based services. An accessible, effective and comprehensive mental health system is the “ultimate intercept” that can keep people with mental illness from entering the justice system (
1).
One application of the sequential intercept model is the Sequential Intercept Mapping and Taking Action for Change workshop. Developed by Policy Research Associates, the workshop is a two-day program where trained facilitators guide local community stakeholders through the sequential intercept model to identify resources and gaps in service. During the action planning portion of the workshop, the group identifies priorities for change and develops action plans to address their goals, some of which are short-term and attainable with little or no cost. Sequential intercept mapping helps communities identify resources, practices, and cross-systems approaches to encourage treatment engagement of those in need while preventing justice system involvement.
The Ohio Criminal Justice Coordinating Center of Excellence, a statewide technical resource center for jail diversion alternatives for adults with mental illness, has a team of sequential intercept mapping facilitators trained by Policy Research Associates. Since 2013, 22 Ohio communities have completed sequential intercept mapping to address the problem of adults with mental illness in the criminal justice system. Sequential intercept mapping is available to communities through other statewide initiatives in Pennsylvania, Oregon, Virginia, Florida, and Massachusetts, and throughout the U.S. by Policy Research Associates. Sequential intercept mapping is a promising way to stimulate collaboration across systems and stakeholder groups within a community to address the overrepresentation of adults with mental illness in the criminal justice system (
2). An evaluation of sequential intercept mapping is underway in Ohio, yet research on sequential intercept mapping and its effect on reducing the presence of adults with mental illness in the justice system is needed.
This framework has recently been applied to identify opportunities for screening, treatment, diversion, and overdose education to address opioid users at risk of overdose (
3). Adapting the sequential intercept model for opioids places greater emphasis on the ultimate intercept, now referred to as “intercept 0” (
Figure 1), and includes not only treatment services but also crisis response services, prevention, and regulation (
1,
4). Opioid-involved deaths continue to increase in the United States. There were more than 42,000 deaths in 2016, with an average of 116 Americans dying every day from an opioid overdose (
5). The crisis is burdening hospital emergency departments, crisis services, and law enforcement and has had an overall estimated economic cost of more than $504 billion, with a cost of $7.8 billion to the justice system alone (
5,
6).
The criminal justice system has a substantial overrepresentation of people with substance use disorders. About 68% of jail inmates meet the criteria for alcohol or drug use disorders and dependence, compared with 8% in the general population (
7,
8). Although the precise prevalence of opioid addiction among inmates is difficult to estimate, jails throughout the United States report the numbers have grown at an astounding rate (
9). Both the overrepresentation of people with mental illness in the justice system and the opioid crisis are complex problems that may be resolved only with the sustained efforts of a comprehensive set of engaged stakeholders from multiple systems working together to create solutions that fit the needs of their community.
Sequential Intercept Mapping for Opioids: A Promising Approach
Drawing from the Ohio Governor’s Cabinet Opiate Action Team and the Substance Abuse and Mental Health Services Administration’s Opioid Overdose Prevention Toolkit, the sequential intercept mapping framework was adapted to emphasize prevention, regulation, and treatment responses for opioid dependency, such as coordinated, evidence-based prevention programming that reflects a local community risk assessment, accessible prescription drug drop-off sites, and medication-assisted treatment. The sequential intercept mapping workshop developed by Policy Research Associates facilitates planning around the interface of community-based prevention and awareness activities, regulation practices, treatment services, and intercept points within the justice system; affords communities the opportunity to develop strategies across systems to improve care for individuals affected by opioid use; encourages collaboration to address a complex issue; and, it is hoped, ultimately decreases deaths associated with opioid overdose.
Sequential intercept mapping for serious mental illness and sequential intercept mapping for opioids have fundamentally different goals. Sequential intercept mapping for serious mental illness has the principal goal of reducing justice system involvement of individuals with mental illness; sequential intercept mapping for opioids has the principal goal of reducing opioid overdose deaths. Presumably in each case the goal is accomplished by connecting people to the treatment they need, although prevention and regulation are emphasized more within sequential intercept mapping for opioids. The two mapping initiatives result in different community-based solutions and priorities, even when engaging a similar array of community services, assessment practices, and procedural responses.
In opioid mapping, the stakeholders, community-based resources, and partnerships that are needed to address the problem reach beyond the intersections of the mental health and criminal justice systems. Stakeholders who participate in opioid sequential intercept mapping are sometimes less likely to participate in mapping for justice-involved adults with mental illness. They include representatives from public school systems, fire and emergency medical services, public health, the county medical examiner’s office, public media, and the business community. Attention is paid to addressing stakeholders’ biases about individuals with opioid addiction and their treatment. Sequential intercept mapping for opioids includes a training component in which the nature of addiction as a brain disease is articulated, as is the rationale and critical role of medication-assisted treatment along with 12-step and cognitive behavioral therapies. Both the medical and spiritual aspects of recovery are emphasized.
In Ohio, sequential intercept mapping to address opioids was piloted in a county with one of the highest opioid overdose death rates in the state. The success of the pilot led to the state’s decision to use 21st Century Cures Act funds to provide sequential intercept mapping focused on opioids to Ohio communities working to reduce opioid-related deaths. Now six counties have completed mapping specific to opioids, and an additional five communities are in the planning stages. Communities identified for sequential intercept mapping have been prioritized because of the number of opioid-involved deaths. The first county to undergo sequential intercept mapping for opioids in 2015 experienced 10 fewer overdose deaths in 2017 after leveling off in 2016, despite the increased presence of the dangerous synthetic opioids fentanyl and carfentanil. This is insufficient time to claim a decreasing trend, and research is needed to examine the effects (if any) of sequential intercept mapping on this pattern, but local stakeholders cite a shift in culture and communitywide collaborative efforts, including enhanced prevention programming, increased utilization of medication-assisted treatment, partnerships with first responders, federal law enforcement interdiction efforts, and specialty court dockets.
Primary Objectives
There are two primary objectives of sequential intercept mapping for the opioid crisis: encourage counties to organize their efforts within a cross-system, shared infrastructure that is driven by a common vision; and assist counties in selecting priorities to guide local efforts, based on evidence-based or best practices. Collective Impact, a framework for organizing multiple systems, is compatible with sequential intercept mapping and may provide the infrastructure necessary for organizing communitywide efforts. It involves the commitment of a group of important actors from different sectors to a common agenda for solving a specific social problem (
10). The framework is a structured approach to tackling complex social problems by using five elements: a common agenda, measuring results consistently, mutually reinforcing activities, continuous communication, and a backbone organization. One Ohio county that completed sequential intercept mapping for opioids adopted the Collective Impact framework to organize collaborative work. First, community stakeholders used sequential intercept mapping to establish a baseline map of systems, identify gaps and resources, and prioritize system gaps to be addressed through action plans. Then, all initiatives, strategies, data collection, analysis, reporting, and public communication were designed to flow through the backbone organization. Again, research is needed to substantiate any claims of effectiveness, but stakeholders have sustained their collaborative efforts to address opioid-involved deaths by using this combined approach.
Conclusions
Sequential intercept mapping is an important framing tool for organizing cross-systems responses to complex problems. Two such problems are the overrepresentation of people with mental illness in the criminal justice system and the epidemic of opioid addiction and overdose deaths. Sequential intercept mapping appears to be an approach to address the two problems, yet the resulting priorities and solutions and key stakeholders are different enough that distinct mapping exercises are necessary to help community stakeholders address each problem as effectively as possible.
Acknowledgments
The authors thank Christopher Nicastro, Julie Spohn, and the Ohio Criminal Justice Coordinating Center of Excellence.