Crisis mental health care is an integral component of the mental health care system but is currently deemed “inconsistent and inadequate” (
1). The National Action Alliance for Suicide Prevention, a public-private partnership focused on advancing suicide prevention in the United States, has prioritized transforming U.S. crisis mental health care, including enhancing the availability and quality of the 24/7 regional crisis call centers (including crisis text and chat services) that make up and extend the National Suicide Prevention Lifeline (NSPL) (
1). In August 2018, the National Suicide Hotline Improvement Act was signed into law, requiring federal agencies to investigate the feasibility of making crisis mental health care more available through an “N11” telephone number and to analyze the effectiveness of the NSPL. These intertwined efforts will require careful study of the calls made to the NSPL and other help-seeking behavior, as well as current capacities to meet demand, including where and when predictable surges may occur.
In the United States, there are temporal patterns in suicide; for example, suicides peak in the spring, with a second, smaller peak in early summer (
2). In addition, some events, including celebrity suicide deaths, serve as “shocks” that disrupt seasonal time trends and may prompt imitation (
3–
5). An estimated 1,841 suicides in the United States between August and December 2014 were attributed to imitation after the August 11, 2014, death of entertainer Robin Williams; most of the excess suicide deaths during that period resulted from suffocation, the same cause of death as Mr. Williams’, who died by hanging himself (
6,
7).
Estimating excesses of imitative suicide deaths, as was done in the wake of Mr. Williams’ suicide (
7), is useful for testing the “Werther” and “Papageno” effects—to determine how certain types of reporting might exacerbate and others help mitigate imitative suicides (
3,
8). The traditional preventive response is to encourage responsible reporting of celebrity suicides (by following guidelines listed, for example, on reportingonsuicide.org). Research on Canadian media confirmed that most stories adhered to published guidelines (
9), although we are not aware of U.S. media’s adherence to these guidelines after Mr. Williams’ suicide.
Mr. Williams’ death also led to increases in online searches for both harmful (e.g., “hanging”) and helpful (e.g., “lifeline”) information about suicide (
10). This, coupled with evidence that imitative suicides typically begin immediately after media reports of a celebrity’s death (
5), suggests that demand for crisis and suicide prevention services will spike immediately after a celebrity suicide. The aim of the investigation reported here was to examine increases in suicides and the demand for crisis services in the immediate aftermath of Mr. Williams’ suicide.
Methods
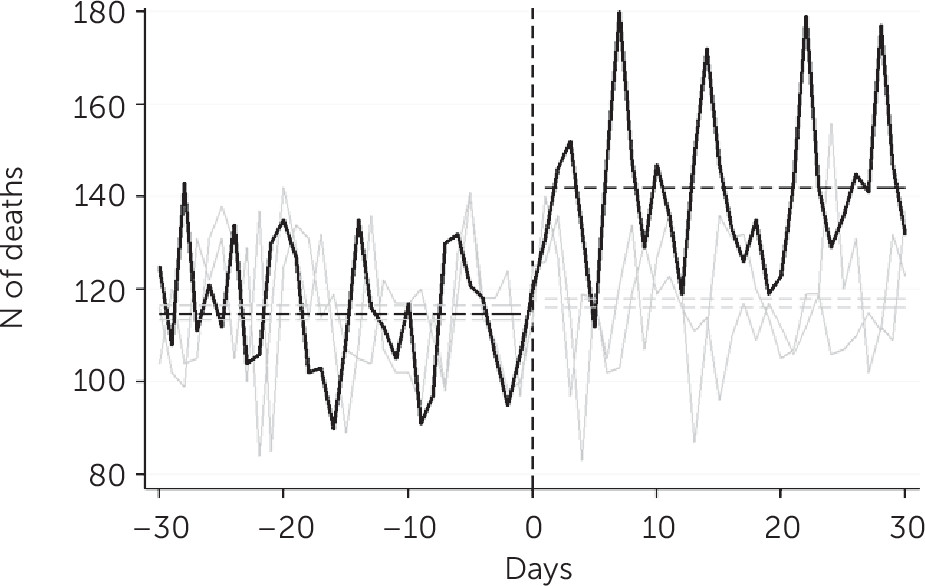
To confirm the hypothesis of an acute excess of deaths associated with celebrity suicides, we compared U.S. daily suicides by suffocation (ICD-10 code X70) and total suicide deaths (ICD-10 codes X60–X84 and Y87.0) in the 30 days before and after August 11, 2014, as well as for the same periods in 2012 and 2013 by using t tests. Data came from the National Center for Health Statistics’ Compressed Mortality File.
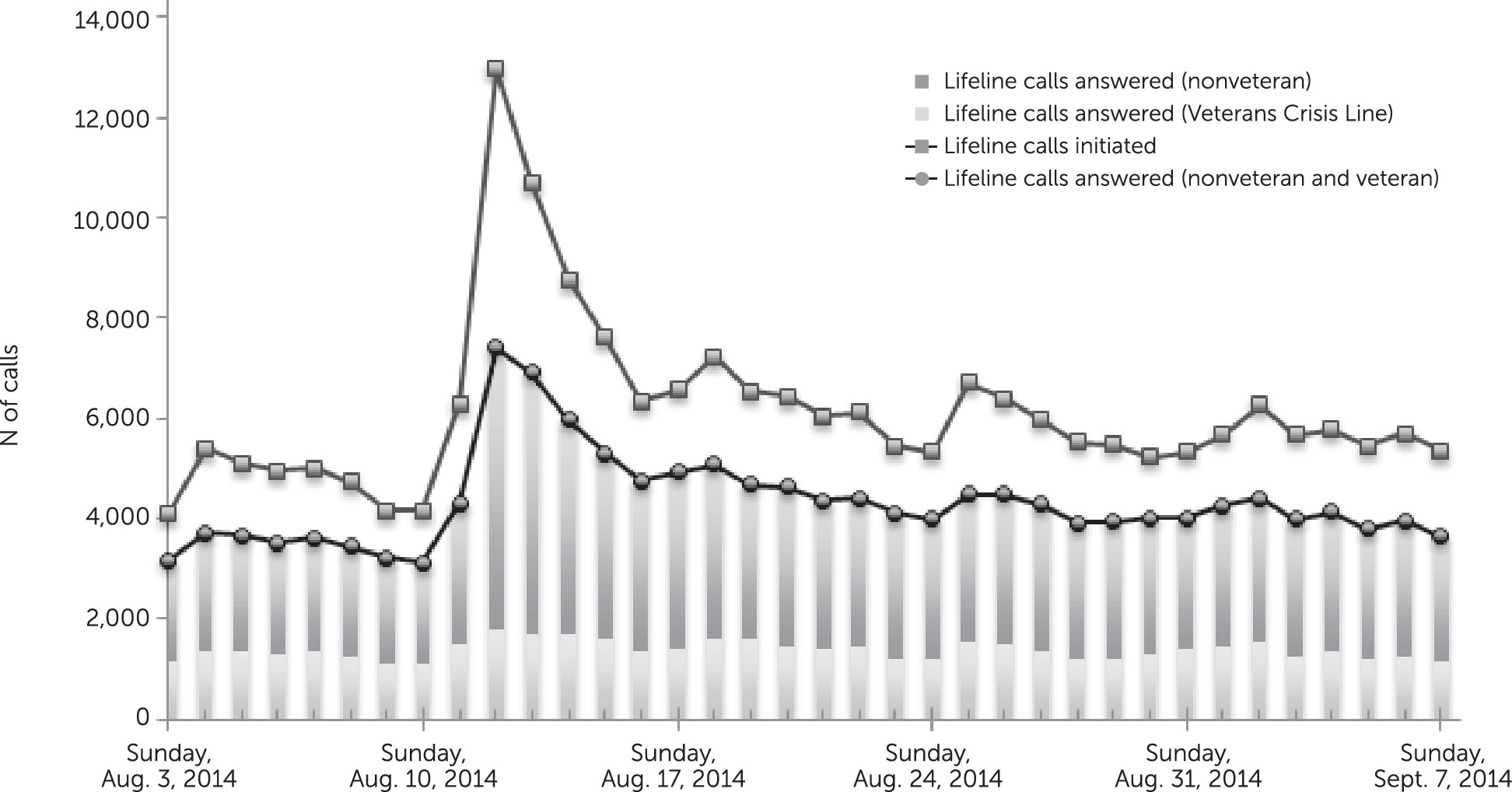
To examine help seeking for suicide crisis services, we analyzed call volume data from the NSPL, a national network of crisis centers connected to a series of toll-free numbers, the most prominent of which is 800–273-TALK (8255). Callers to the NSPL can access the Veterans Crisis Line (VCL), through a “press 1” option on the automated greeting message. All others are connected to one of more than 160 accredited community-based crisis centers across the country. We present descriptive statistics of daily NSPL call volume between August 3 and September 7, 2014, as well as information on the number of calls answered by the VCL and the non-VCL call centers.
To examine information seeking about suicide risk, we acquired data on daily visits to two Web sites: the Suicide Prevention Resource Center (SPRC), which provides technical assistance, training, and materials on suicide prevention; and Suicide Awareness Voices of Education (SAVE), which provides education and seeks to raise public awareness and serves as a resource for those affected by suicide.
Results
In the 30 days before August 11, the number of suffocation suicides averaged 27–31 per day in 2012, 2013, and 2014. For the 30 days after August 11, the average daily number of suffocation suicides was similarly 29 in 2012 and 30 in 2013, but in 2014 the number was 47 per day (p<0.001). We observed a similar pattern for suicides overall (
Figure 1). The average daily number was 113–117 for the 30 days before August 11 in 2012–2014 and for the 30 days starting August 12 for 2012–13; however, in the 30 days starting August 12, 2014, the average number was 142 per day (p<0.001). Approximately two-thirds of the additional suicides observed immediately after August 11, 2014, were suffocation deaths.
On August 12, 2014, there was a spike in calls made to the NSPL (
Figure 2). In the week prior to the death of Mr. Williams, the NSPL received from 4,116 to 6,302 calls per day. That number increased by up to 300% to 12,972 calls on August 12, 2014, and decreased incrementally thereafter. Most of the increase in calls was driven by the increase in nonveteran calls; the number increased from 2,839 NSPL calls answered on August 11 to 5,607 on August 12, compared with an increase from 1,469 to 1,799 VCL calls answered for those two days. Calls made to the NSPL returned to stationarity 2 weeks after the death of Mr. Williams, although the average daily number of calls during this period was higher (daily average of 5,748 between August 25 and September 7) than before Mr. Williams’ suicide (daily average of 5,375 between August 3 and 10).
Figure 2 also presents data on answered and unanswered calls. Between August 3 and August 10, 2014, 73% of calls to the NSPL were answered; between August 3 and September 7, 2014, 71% of calls were answered. Only 57% of calls were answered on August 12 and only 65% and 68% were answered on August 13 and 14, respectively, indicating a gap in current capacities. The proportion of answered calls between August 15 and September 8 fell below 70% only once.
The SPRC Web site averaged 2,315 visits per day between August 3 and 11, 2014. On Tuesday, August 12, a total of 5,981 visits were made to the site, and the average between August 13 and September 7 was 3,216 visits per day. For SAVE, the Web site averaged 4,239 visits per day between August 3 and 11 and 24,819 visits on August 12; the average daily visit rate was 5,201 from August 13 to 31.
Discussion and Conclusions
Improving America’s crisis mental health care system will require ensuring 24/7 access to crisis services. This requires ensuring capacity to meet regional and seasonal patterns of demand, as well as surge capacity to accommodate spikes in help seeking after future celebrity suicides or other events (i.e., television shows and movies) that may also give rise to imitative acts. Access to timely suicide surveillance data could enable researchers to identify smaller but still significant surges in suicide and help seeking. Investigating changes in demand for other crisis services after a celebrity suicide, which we recommend as subjects of future research, may identify the need to enhance surge capacity for these services to more adequately equip the national crisis mental health care system. This includes hospital emergency departments, law enforcement, poison control centers, and health departments, as well as the mental health resources that serve as referral endpoints to some crisis calls (
11) and that are listed on SPRC and SAVE Web sites. Across the range of crisis services, creative and efficient options need to be designed for meeting increases in demand, and research is needed to monitor and evaluate their success.
The public health response to celebrity suicides has been to encourage adherence to reporting guidelines to prevent subsequent imitative acts (
12). This is important and should continue, particularly because adherence to some of these guidelines declined between 2011 and 2013 (
9,
13). These guidelines include promoting suicide prevention resources; in August 2014, the NSPL tracked 1,520 mentions of its telephone number in media reports, up from 120 the month before. Such reporting—consistent with recommended practices—may have helped drive demand for crisis services beyond the NSPL’s capacities. The expanded use of SPRC and SAVE may also have contributed to the demand.
The findings presented here should be considered alongside certain limitations. A primary one is that it is unclear how many calls to the NSPL after Mr. Williams’ suicide were information seeking, and thus only somewhat reflective of “demand” for crisis services. This limitation is partly mitigated by the established increase in suicides that occurred after Mr. Williams’ death, suggesting that an acute suicidal crisis occurred after his suicide. We were also not able to track unique visitors to the resource Web sites; some of the visits may have been one or more persons visiting multiple times. These counts likely also included journalists and commentators using the wealth of information provided at each site for reporting on the celebrity suicide.
There is variability across the NSPL network, including in the resources available to specific call centers. Individual call centers receive federal funding of $2,500 annually to support hotline services, supplemented to varying degrees by state and local governments and private donors (
14). Additional and consistent support for the NSPL network and its components may help preempt future gaps in capacity, as shown in this study by the proportion of calls that went unanswered, but it is probably not feasible to operate regularly at the level needed under surge conditions. Whereas regional surges may be accommodated by shifting resources from an unaffected area to an affected one, celebrity suicides may have national or even global effects, limiting the feasibility of regional backups, because unaffected areas may not exist.
The enhancements needed for meeting demand for crisis mental health services, including surge capacity, will require both allocating existing funds more efficiently and procuring new funding, although the National Hotline Improvement Act of 2013 authorized no additional funding. Research is needed to estimate the potential cost savings that investing in the NSPL and other crisis mental health services, and building surge capacity specifically, may have on reduced emergency department admissions, hospital readmissions, overuse of law enforcement, and the loss of human life.