Involuntary inpatient civil commitment refers to a legal intervention used in every U.S. state where individuals not accused of a crime but suspected by laypersons or after a psychiatric evaluation to pose a danger to themselves or others because of mental illness or substance abuse can be seized, transported, or held in custody at a hospital or other authorized facility for examination and sometimes involuntary treatment. Civil commitment raises vexing clinical, ethical, legal, and human rights issues (
1). However, how often it is employed in the United States is unknown. No federal data set appears to track commitments (
2), unlike rates of other formal deprivations of liberty, such as criminal arrest or imprisonment, which are documented yearly by the federal government (
3,
4).
Incidence refers to how often an event newly occurs in a given population over a set period, commonly expressed as the number of events per 100,000 persons per year. Counting civil commitments, however, is difficult because laws across 50 states specify different mandates and timelines to initiate and maintain a commitment (
5–
7). Nonetheless, the core component of civil commitment is involuntary detention of an individual because of mental illness. Its simplest typology is a short term or emergency detention that may overlap with or extend into a longer-term detention (itself sometimes subdivided into a “commitment court order” and an “extended commitment”) (
5,
8,
9). In the first phase, a person is held in custody generally for a period legally limited to 3 or 4 days (although variations exist, up to about 30 days) (
10); the person then either agrees to be hospitalized, is released, or is held to await a hearing to determine whether longer-term commitment will be pursued. The next phase is expected to proceed if a court or physicians order a commitment, sometimes specified to last up to 14 days and extend in 30-, 90-, and 180-day increments (variations exist here too), subject to judicial review. We aimed in this study to count shorter- and longer-term detentions.
One-fifth of publications indexed in PubMed under the medical subject heading “commitment of the mentally ill/statistics and numerical data” originated from the United States (results of the PubMed query are presented in a table in an
online supplement to this article). We found population rates in just three studies, each using state counts. In Florida in 2000, the rates were 506 all-ages emergency detentions or 351 persons per 100,000 (
11), and during 2000–2003, “close to 1% of all youth in the state” (
12). In Oregon, the rates were 45 and 22 all-ages longer-term commitments per 100,000 in 1983 and 2003, respectively (
13). Other studies provided aggregate counts of involuntary psychiatric detentions or of unique individuals subjected to them in a single county or state. In Spokane County, Washington, the number of 72-hour detentions increased continuously each year, from 200 in 1974 to 700 in 1984, and 14- and 90-day commitments rose less sharply (
14). In California, aggregate quarterly counts of 72-hour detentions and 14-day and longer commitments in 28 counties between 2000 and 2007 exhibited seasonal variation (
15). Two studies counted substance abuse commitments specifically: circa 2010, a mean of five per county in Wisconsin (
16) and a total of 14,200 in seven of 50 states surveyed (
17). One study reported that, among 257,625 adults receiving emergency paramedic services between 2011–2016 in Alameda County, California, 26,283 were placed on an involuntary 72-hour hold (
18). Some of the aforementioned studies reported that 20% of people had more than one emergency detention (
11,
12,
14), and 7% had more than five (
18), highlighting the need to specify whether numerators of population rates contain numbers of detentions or of individual persons and whether denominators contain adults, minors, or both (
19).
Data on length of stay (LOS) were few and disparate: among 265 involuntary holds of preadolescent children in one pediatric emergency department in Los Angeles in 2016, the median LOS was 4.7 hours for discharged children and 11.7 hours for those transferred to hospitals (
20). Among 500 individuals under “temporary detention orders” in Virginia in 2008 (half of whom went on to a longer-term commitment), 14% were first held for 0–24 hours, 67% for >24–72 hours, and 20% beyond 72 hours (
21). For 5,000 emergency holds in community inpatient settings in Oregon in 2005, the mean LOS was 10.7 days (
22).
Finally, although two reports aimed for multistate or national scope (
10,
17), we located only one national estimate: on the basis of data from a survey of 544 psychiatric and general hospitals, it was estimated that 26% of 1.17 million inpatient admissions in 1980 were “involuntary noncriminal commitments” (
23).
In summary, over the past 40 years, data on the frequency of involuntary civil psychiatric detentions in U.S. jurisdictions have remained sparse. We found no time series or comparative study that included two or more states, and studies using state counts rarely assessed their accuracy (
24). No study raised the issue of extralegal detention (not prescribed by law, such as formally voluntary patients being informally detained) (
25–
27).
We were familiar with counts released annually by California and Florida and analyzed in some studies (
11,
12,
15) and aimed here to collect similar counts—excluding those of outpatient and criminal commitments—from as many U.S. states as possible to compute population rates during the 2010s. We sought publicly available counts because their existence partly fulfills the accountability of state institutions for rights-restrictive measures carried out in the public’s name, using the public purse. Civil commitment, a main proxy measure for coercive care, persists despite major changes over 40 years in the nature, loci, financing, and organization of mental health services and in access to these services (
28,
29). Presently, civil commitment faces challenges from a human rights approach rooted in the United Nations Convention on the Rights of Persons With Disabilities (
30), and some officials advocate expanding civil commitment to respond to social problems, such as firearm violence and homelessness (
31). A current, transparent effort to quantify involuntary detentions in the United States might lead to more informed analyses and discussions of civil commitment.
Methods
We carried out this study between April 2015 and February 2020. We conducted repeated state-specific online Google searches, excluding the District of Columbia and U.S. territories, using the following terms, singly and in combination: admission, commitment, compulsory, detention, emergency, examination, hospitalization, involuntary, and mental health. This strategy identified post-2010 annual counts from nine states. We then used the same terms to search the websites of each state’s department of mental or behavioral health (DMH) and court or justice system, bringing the total to 36 states. In addition, we found one state’s counts in a journal article (
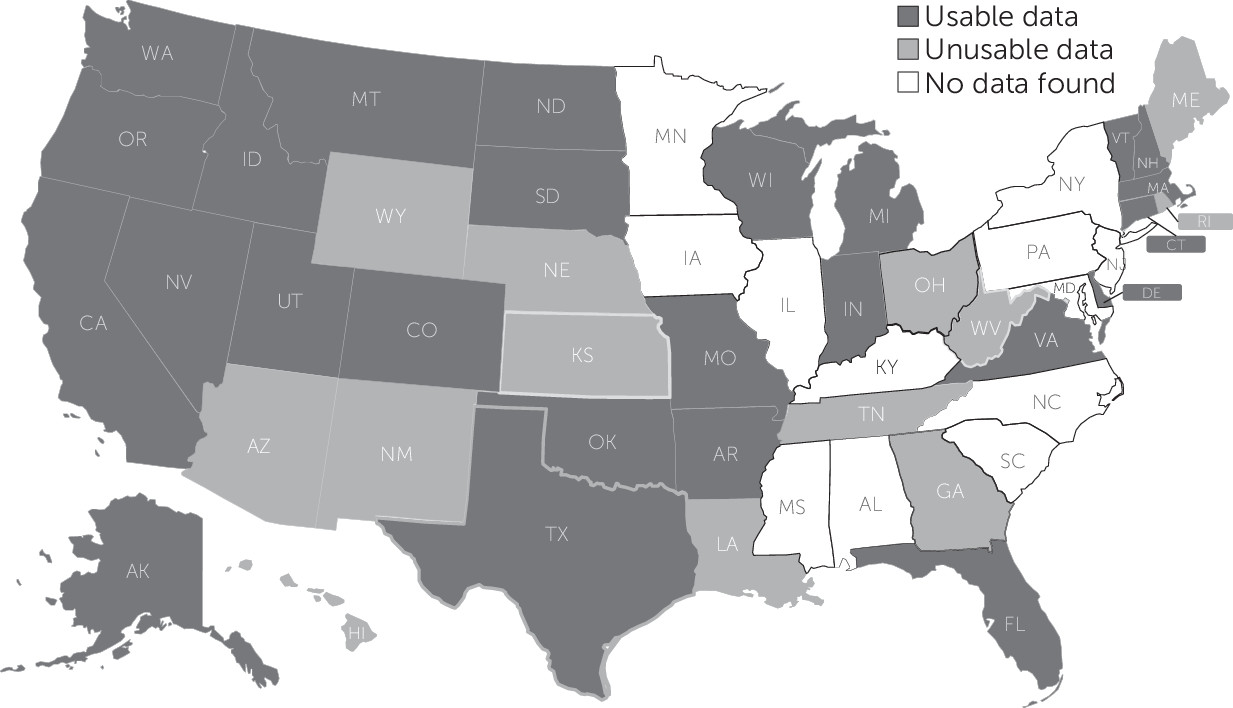
32), and one state provided counts after a telephone request. We found no data for the remaining 12 states. We did not contact officials or advocates in all states and may have missed pertinent data despite repeated searches. We scrutinized all collected counts, excluding 13 states because nine described counts in imprecise terms with no definitions, three mixed civil and criminal commitments, and one reported fewer than 12 commitments over 3 years despite other disconfirming evidence. This left 25 states that we both judged to have usable counts (
Figure 1), including 22 with 6 or more years of data between 2011 and 2018, which let us examine patterns of increase and decrease in counts.
The usability of counts varied (
Table 1); 15 did not distinguish between shorter- and longer-term detentions, so we treated them as emergency only, and 17 did not specify to which age group (adults or minors) their counts applied, so we used United States Census Bureau (
33) total-population estimates rather than age-specific estimates to compute yearly crude rates of detentions by state, as follows:
Each author independently extracted the data; both verified the data and resolved disagreements by discussion. A table in the online supplement includes all collected counts, classified as emergency and longer term, by state and year from 2011 to 2018, with percentage change from the preceding year and from first to last year of data. Another table in the supplement provides the name of each source, its online link, and its description of the counts.
Results
All-ages emergency detentions per 100,000 people from 2011 to 2018 in each of 25 U.S. states with usable counts are shown in
Figure 2. They ranged from 29 in Connecticut (2015) to 966 in Florida (2018). Among 22 states with at least 5 years of data without gaps (2012–2016), we calculated an average rate of 273.2 in 2012 (median 173.6), rising to 309.0 (a 13.1% increase) in 2016 (median 195.6), while the mean state population increased from 6.7 to 6.9 million (a 3.9% increase) during the same interval.
Of 22 states with 6 or more years of data, 15 had a net count increase between the first and last year (mean 50.5%, range 0.6%–139.2%), and seven had a decrease (−17.4%, range −0.4% to −68.5%). When we removed outliers, increases averaged 27.3% (range 9.1%–88.6%) and decreases averaged −3.8% (range −0.4% to −8.1%). States with count increases and those with count decreases both experienced population increases, averaging 5.3% and 4.8%, respectively. The largest count increases were in Nevada (139.2%) and Indiana (102.7%) over 8 years and in Colorado (88.6%) over 6 years. The largest decreases were in Delaware (−68.5%) and Wisconsin (−34.7%).
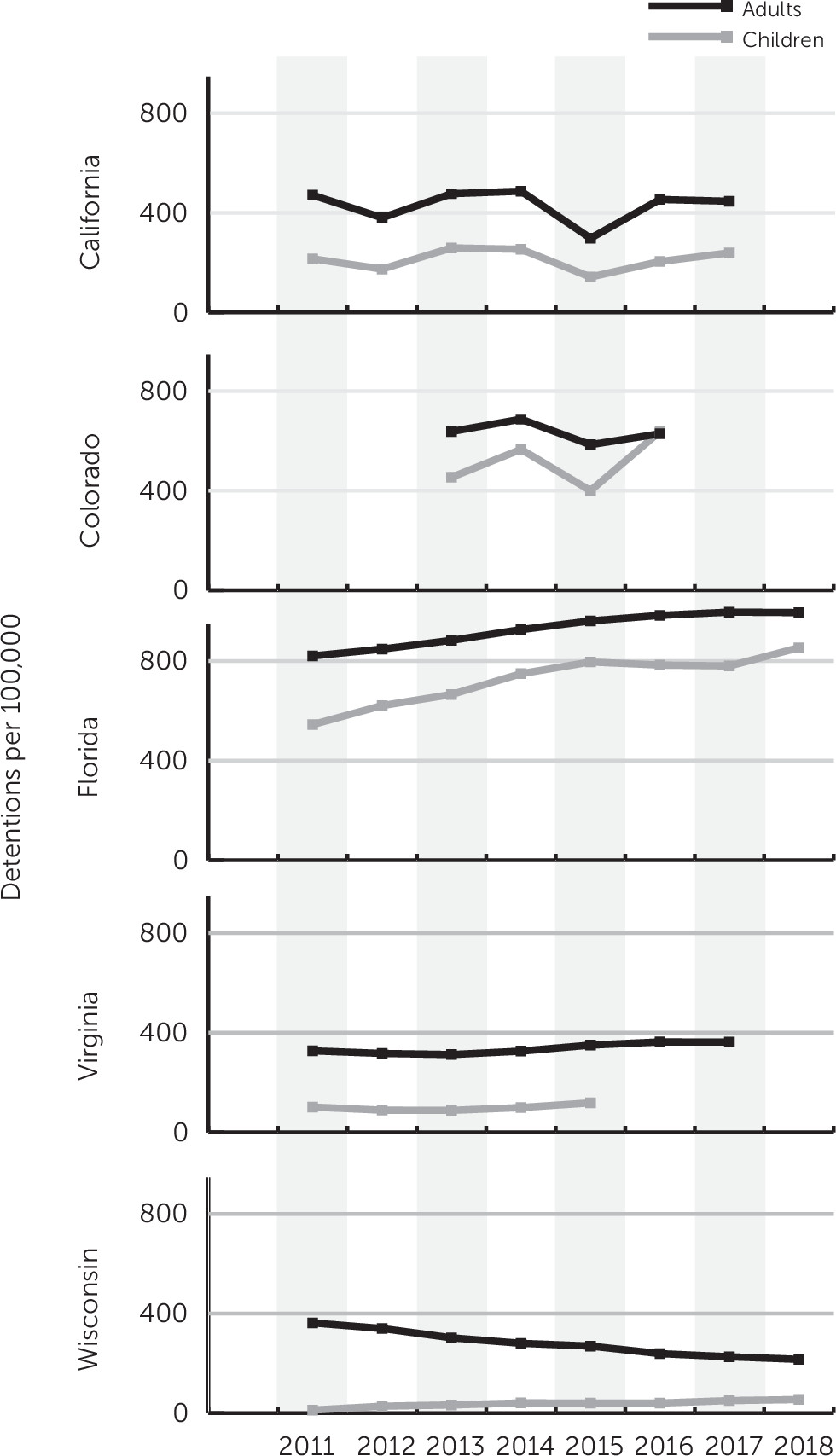
Figure 3 shows that in four of five states providing separate counts of emergency detentions for adults and children, rates for both groups showed nearly parallel lines over the study period.
Only eight states provided counts of longer-term detentions.
Figure 4 shows that, between 2011 and 2018, all-ages state rates per 100,000 people ranged from a low of 18 in Oklahoma to a high of 204 in California. We calculated mean annual state rates per 100,000 people, which ranged from lows of 25 and 27 (Oklahoma and Missouri, respectively) to highs of 158 and 159 (Virginia and California, respectively). These longer-term rates were, on average, 42.2% of a state’s mean emergency detention rate during the same period (median 38.9% and range 13% in Missouri to 107.9% in Vermont). Only Vermont reported LOS data: from 2011 to 2018, mean LOS for longer-term “adult involuntary stays” ranged from 35 to 48 days (median 18–21 days).
Finally, only Colorado reported separate counts of detentions and persons detained; from 2012 to 2016, a mean of 89.9% of all-ages emergency detentions (range 88.3%–91.7%) and 81.2% of longer-term detentions (range 68.8%–87.8%) represented unique persons. On request, Florida provided us with estimates of unique persons: a mean of 78% per year from 2010 to 2016 (range 78%–79%) of counts of all-ages emergency detentions (personal communication, Annette Christy, Ph.D., Louis de la Parte Florida Mental Health Institute, Baker Act Reporting Center, August 29, 2018). Thus, during the years surveyed, on average 10% and 22% of persons subjected to emergency detentions in Colorado and Florida, respectively, were held more than once.
In 2014, the most recent year with the most reported counts, 24 states—with a combined population of 165.4 million people (51.9% of the U.S. population)—recorded a total of 591,402 detentions that we classified as all-ages emergency detentions (a crude overall rate of 357.4 per 100,000). Five states, which accounted for 59.2% of the 24 states’ combined populations (Florida, California, Massachusetts, Texas, and Colorado), accounted for 79.8% of the detentions.
Discussion
To our knowledge, this study provides the first present-day estimates of involuntary psychiatric detentions in the United States based on publicly available data from the largest sample of states in the literature. In 2016, among 22 states, the median and mean emergency detention rates were 196 and 309 per 100,000 people, respectively. Between 2011 and 2018, across 25 states, all-ages emergency detention rates per 100,000 people ranged from 29 in Connecticut to 966 in Florida (a 33-fold variation). Of 22 states with ≥6 years of data, 15 showed a net count increase between the first and last year, and seven showed a decrease. Of eight states that provided counts of longer-term involuntary hospitalizations, all-ages rates per 100,000 people ranged from 18 in Oklahoma to 204 in California. The validity of these estimates, however, is weakened by the study’s limitations discussed in the following.
It is difficult to count civil commitments across states because definitions and mandates for commitment differ among states. The tallying was further complicated by too little accompanying information about the length of any detentions. The data fit the simplest typology of an initial detention that may extend into a longer-term detention, but the data (especially from courts) allowed no finer distinctions. We therefore treated unknown numbers of detentions extended for unknown durations as “at least emergency” detentions. Also, because courts rarely specified whether they counted adults, children, or both, our use of total-population denominators in these cases likely underestimated the incidence of involuntary psychiatric detentions. A few states had both court and DMH counts, but these were discrepant. In these cases, we selected the DMH data because they were better defined. Selecting only court data for consistency would have yielded a different sample of states and different population rates.
The dearth of case definitions and dispositions and our unfamiliarity with individual state practices strained our ability to interpret the data and to address sources of error—such as whether a state’s counts included detentions at nonstate or private facilities, which only a small number of states specified. For example, Colorado’s recent Senate Bill 17-207 mandates health care facilities “not designated” to receive emergency detentions to start reporting these detentions (previously excluded from Colorado’s counts). Its Office of Behavioral Health, responding to an open records request, documented that from May through December 2018, a total of 18,701 involuntary 72-hour holds—56% of which were extended to “continued involuntary treatment”—occurred in 75 “nondesignated facilities.” These concealed detentions would substantially increase the Colorado rates reported in this study.
The issue of privileged access to more complete data than are available on official websites deserves mention. We obtained unpublished data from two states, and our literature search found three studies that analyzed publicly unavailable data that researchers obtained because of privileged relationships with a state DMH and court system (
14,
21,
32). Other examples probably exist. This suggests that possibly better-quality incidence or prevalence data are available to some researchers, although we did not find these data used widely in the literature.
Because 24 of the 25 states included in this study provided no LOS data, it remains unknown whether there is a “mismatch” (
8) between the statutory timelines for involuntary hospitalizations and the relatively brief mean duration of psychiatric inpatient stays nationally (reported without attention to legal status), which was, for adults, 6.6 days in 2012 and 6.8 days in 2014 (
34,
35). Mean rates of longer-term detentions across eight states varied about sixfold and suggested that, on average, about 40% of initial detentions were extended to last anywhere from 2 weeks to 2 years. Only population-based data on the duration of any type of psychiatric detention will clarify the issues.
Despite a dissimilar incidence of emergency detentions of adults and children in the five states with relevant data, in four states the rates for adults and minors followed nearly identical trajectories over the years observed (except for a state that did not distinguish between emergency and longer detentions). The paucity of studies reporting or analyzing rates of civil commitment of youths impedes interpretation of this counterintuitive finding. If not an artifact, the relationship suggests that strong nationwide factors uniformly influence the commitment of both adults and minors.
During our review, we found three relevant national databases and reports. First, the National Association of State Mental Health Program Directors’ National Research Institute (NRI) listed, without reliability checks, numbers of emergency holds or longer commitments from 18 and 37 states in 2013 and 2015, respectively (
36,
37), taken from a survey distributed to directors of states’ behavioral agencies. For 2015, in nine states for which NRI and this study shared emergency detention counts, NRI’s total was 190,000, whereas our study’s total was 290,000. This large difference could result from the NRI respondents’ inconsistent inclusion of commitments to private facilities and apparent omission of court records. Second, the Federal Bureau of Investigation’s National Instant Criminal Background Check System (NICS) receives states’ data on persons “adjudicated as a mental defective” or “committed to a mental institution,” who are prohibited from buying firearms under the Brady Handgun Violence Prevention Act of 1993 (
38). As of January 31, 2020, NICS had 6,065,302 active “adjudicated mental health” records (
39), but these do not separate “adjudications” from “commitments” or give dates for either. Third, 1-day point prevalence estimates of inpatients according to legal status were collected by the Substance Abuse and Mental Health Services Administration during recent surveys of all known mental health facilities. On April 29 of 2014 and April 30 of 2016, a total of 34,816 and 40,688 individuals, respectively, classified as “nonforensic involuntary” made up 34.4% and 38.4%, respectively, of the total U.S. psychiatric inpatient population (
40,
41), but percentages of patient mix cannot be used to derive annual estimates of commitment frequency. In summary, these three national sources did not permit us to reach valid conclusions about the annual incidence of civil commitment in the United States.
We calculated a 22-state mean incidence range of emergency detentions of 273 per 100,000 people in 2012 and 309 per 100,000 in 2016. A recent international comparative study found that rates of “involuntary hospitalization” per 100,000 people in 22 countries across Europe, Australia, and New Zealand in 2015 varied 20-fold, from 14.5 in Italy to 282 in Austria. Thirteen countries experienced an average annual percentage increase between 2008 and 2017, and five experienced a decrease (four did not provide continuous data) (
42). As in the present American interstate study, rates may have comprised both emergency and longer-term commitments in unspecified ways. Increasing rates were observed until the early 2000s in five of eight European countries (
43). In England (population about 56 million), a study of civil involuntary detentions in health care facilities under Part II of the Mental Health Act of 1983 (which included emergency detentions lasting up to 3 days only if they were extended to longer-term detentions) found that detentions increased 19%, from about 94 per 100,000 people in 2012–2013 to about 116 per 100,000 in 2015–2016 (
44). England’s 2017–2018 statistics specify that 15.4% of persons were detained more than once (
45), compared with the 16% average observed for emergency detentions in Colorado and Florida from 2010 to 2016.
In terms of clear definitions and adequate details, England’s annual reports on the Mental Health Act of 1983 do not differ substantially from the reports of some American states, notably Colorado, Florida, Virginia, and Vermont, on their own commitments. (Data from California, Texas, and Missouri were detailed but required more effort to interpret.) However, all these U.S. state reports, unlike England’s, generally contain little to no information on case dispositions, missing data, sources of error, and results of efforts to improve data collection and validity. We did not inquire about whether DMH data are produced pursuant to specific departmental customs, legislative mandates, or other directives, representing an area for future research. Court data, embedded within annual reports of court activities and statistics, generally had no commentary.
Conclusions
The discretionary rather than mandatory nature of commitment laws (i.e., an individual who meets a state’s commitment criteria may or may not be committed) reflects society’s ambivalence toward coerced care, and professionals and laypersons readily admit their mixed feelings on the subject (
2). The vague way that many sources defined their counts may also reflect this ambivalence. However, from whatever ethical angle one views commitment, it has profound implications for society (
2,
28,
46). Therefore, state and private agencies, lay and professional groups, and independent researchers should shed more light on involuntary psychiatric detentions, their correlates, and their outcomes.
Our findings imply that for the near future it will remain difficult to study inpatient commitment empirically, except in single jurisdictions at a time. To assess the broader effects of civil commitment as a primary institutional response to a person’s breakdown seems a more distant prospect. That only a single state reported data on the full length of involuntary detentions seems baffling in this era of electronic records. Why some states report detentions fully whereas others do not publish the simplest aggregate counts should be better understood.
Without accurate incidence estimates, links to potentially contributing and consequent factors of civil commitment cannot be reliably assessed; these include threatened, attempted, and completed suicides (
47); substance misuse or other previous commitments; availability of community resources and hospital beds; police involvement; chronic homelessness; economic deprivation (
48); publicized mass shootings; and natural disasters. The findings of this study signal the need for a meaningful, nationally standardized data collection approach to produce valid population-based estimates of a major rights-restrictive procedure that mobilizes considerable human, economic, and logistical capital across all behavioral health and justice systems in the United States.