Recent efforts to accurately estimate the prevalence of mental illness among children and adolescents in the U.S. have highlighted various methodological challenges (
1). Nevertheless, data from the Phase I Disability Supplement of the 1994 National Health Interview Survey (NHIS-D) provide some information on school-related behavioral problems in this group.
The NHIS is a nationwide household survey that uses a multistage sample design to accurately represent the civilian noninstitutionalized population of the U.S. Selected questions from the 1994 NHIS-D provide estimates of children and adolescents who exhibit one or more behavioral difficulties in school as well as estimates of the number who meet regularly with a mental health professional.
A 94.1 percent interview completion rate was achieved for the 1994 sample, which consisted of 25,705 households containing 116,179 individuals. This report includes data on all household members up to age 17, a total of 30,032 individuals representing a population estimate of 70,023,660. For these target individuals, survey respondents were overwhelmingly a parent (91.6 percent) or a grandparent (6.4 percent).
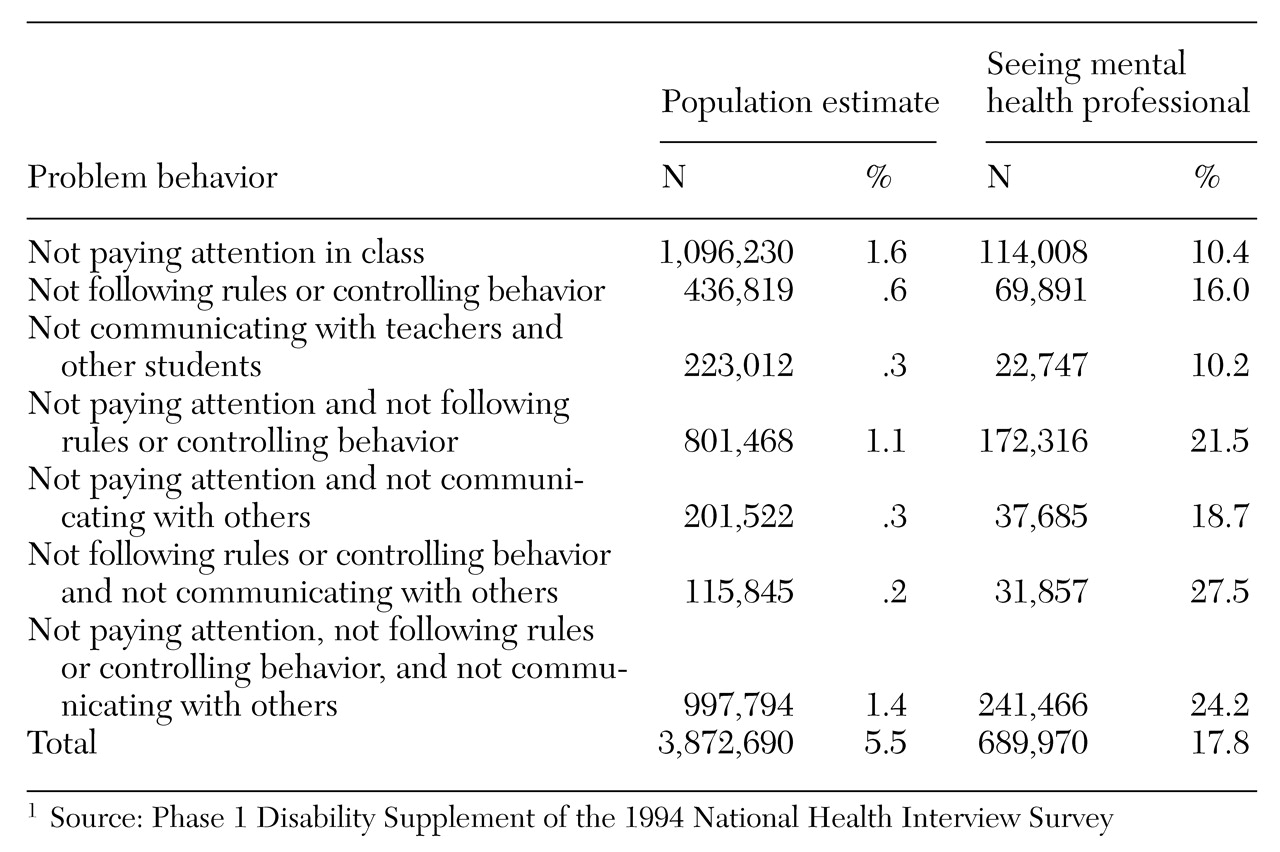
Youths were grouped by the parent's or caregiver's responses to questions about significant problems in three areas of school behavior: paying attention in class, following rules or controlling behavior, and communicating with teachers and other students. Data related to all possible combinations of the problems were examined. The study also examined data on whether the youth saw a counselor, psychiatrist, psychologist, or social worker regularly.
The results indicate that about one in 20 youths in the U.S. are reported to have one or more significant behavioral problems in school, and that only a relatively small percentage consistently receive any specialized mental health services.
Table 1 presents population estimates of the children who exhibit each type of problem behavior and who are currently seeing a mental health professional.
The study is limited because the youths were grouped on the basis of responses to a single question, parents or caregivers were used as informants, and the severity or degree of functional impairment related to the behaviors was not measured. Nevertheless, the relative consistency between these results and other studies using more extensive diagnostic and clinical procedures and protocols suggests that nationally representative samples such as the NHIS-D may usefully supplement epidemiological studies of psychiatric disorders and service use among children and adolescents.
Acknowledgment
The authors thank Henry Krakauer, M.D., for his assistance in the construction of data files.