The overarching goal of psychiatric rehabilitation is to promote the highest possible levels of social and vocational functioning and well-being for individuals with severe and persistent mental disorders, so that they may enjoy optimal levels of independence from professional supervision and the least interference from symptoms and neurocognitive impairments. An essential aspect of psychiatric rehabilitation is for consumers to set personally relevant life goals, and in this task the involvement of their relatives and other supporters is critical.
Achieving these aims requires integration by a multidisciplinary team of what have traditionally been referred to as "treatment" and "rehabilitation" or the "medical" and "psychosocial" models of intervention. To integrate these domains of clinical activity, practitioners must blend competencies from both at the team and individual levels. At the team level, a full array of comprehensive, coordinated, and competently delivered services must be accessible to clients, their caregivers, and people in their naturally occurring support networks. In addition, the team must involve clients and their supporters as active participants in the ongoing process of planning and implementing services. At the level of the individual practitioner, each clinician must have the attitudes and abilities to work collaboratively and with respect for other team members. When all these elements are in place, the services delivered by the team are more likely to be individualized and prioritized to meet the personal goals of the client.
The first section of this article focuses on the properties and functions of the multidisciplinary team, the challenges posed by the need to individualize services, and the barriers to communication and coordination among team members. The second section addresses the roles of the various team members, including general and specific competencies required for conducting rehabilitation. A third section describes the unique role of the psychiatrist. Competencies and roles of team members are placed in the context of the growing availability of evidence-based treatments.
The multidisciplinary rehabilitation team
In psychiatric rehabilitation, many interventions must be implemented simultaneously in different settings with different supporters in a client's social network. Only a team can sustain an efficient and productive range of services. There are few Renaissance people capable of mastering and employing all of the interventions required for overcoming mental disabilities. Therefore, creating a team that collectively has this expertise is the most common means of conducting rehabilitation. In the 21st century, clinicians with multiple competencies in the use of evidence-based services should constitute the team.
In the past, it was customary to assemble treatment teams according to the professional disciplines of their members. Because there were never enough professionally prepared psychiatrists, psychologists, social workers, and nurses to provide services to the large numbers of mentally disabled persons who needed them, the typical team member was a paraprofessional with a high school or college education (
1). In the current era of evidence-based practice, the presence of large numbers of paraprofessionals may be less of a liability if these line-level staff can acquire relevant competencies.
The multidisciplinary rehabilitation team can no longer be limited to office- or hospital-bound clinicians. Instead, it must now include mobile educators, personal coaches, advocates, and community organizers. Contacts by team members with clients' employers, family members, and other supporters generate opportunities for clients to use their newly learned skills in normal environments and also reinforce the use of these skills.
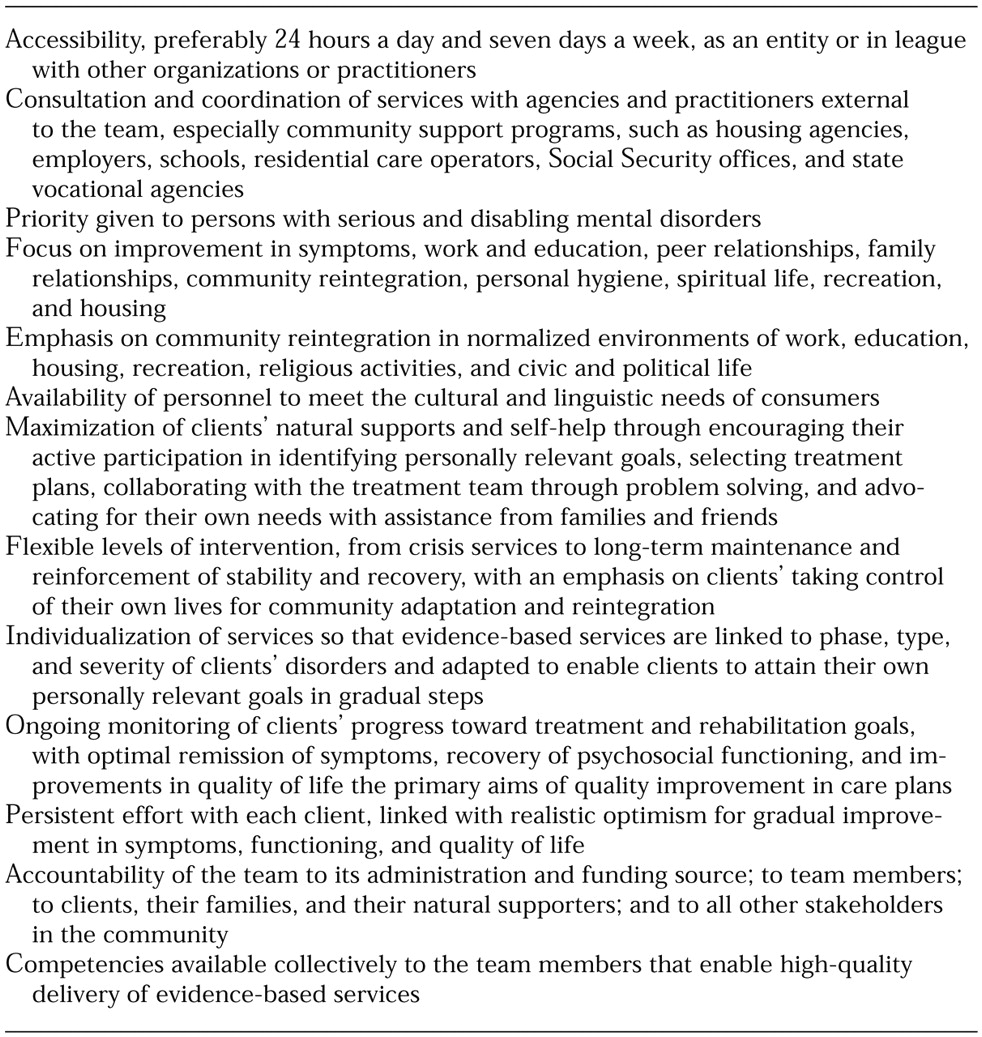
Table 1 lists some of the more important attributes of effective rehabilitation teams. Group dynamics are important correlates of these attributes and mediate team members' competencies for providing evidence-based services. Some of the important group dynamics of a team are cohesion, leadership, distribution of responsibilities and authority, participation in problem solving and decision making, and empowerment through participation in meetings and professional growth (
2).
Key features of the rehabilitation team
Even when a multidisciplinary team begins its work with high levels of motivation and competence, equipped with evidence-based practices, its efforts will be undermined or eroded if its parent agency and managers fail to articulate a clear mission and priority for rehabilitation (
3). Visible and continuing administrative support for the needs, resources, modalities, and goals of a team charged with providing psychiatric rehabilitation is a basic requirement for the team's successful operation, whether in the hospital or in the community (
4). In addition, the types of mental health and rehabilitation practitioners, as well as the balance between paraprofessionals and professionals, are less important for the integrity of a team than the members' competencies.
When team members' roles are well demarcated with clearly specified job descriptions and performance standards, positive supervision, and competency-based training, even well-functioning clients can be deployed effectively on teams (
5,
6,
7,
8,
9). Because of restricted funding for human services and limited availability of professionals, most workers in hospitals and community agencies who conduct psychiatric rehabilitation are paraprofessionals, with a bachelor's degree or less. Thus it is important to select team members for their personal skills and attitudes, such as communicativeness, cultural competencies, enthusiasm, and eagerness to learn, and to ensure that methods of assessment and intervention are user-friendly and well defined (
10,
11,
12,
13,
14).
All work groups, including psychiatric rehabilitation teams, tend to function better when considerable face-to-face interaction is permitted (
15). Thus a team size of four to 12 members is desirable—larger teams generally mean fewer opportunities for interactions with all team members. The workhorse of most teams is the clinical case manager. Some case managers have professional training in social work or psychology, but most are paraprofessionals. To maximize the impact of the case manager and to ensure that the team has competencies relevant to rehabilitation outcomes, specialists who have expertise in diagnosis and psychopharmacology, functional assessment and skills training, family interventions, and supported employment are included on the team.
Teams vary in their power structure. Their leadership and hierarchies differ, as do the clinical responsibilities of team members (
16). In large institutions and agencies, leadership of clinical teams is often based on seniority. However, in rehabilitation settings, personal skills and professional competencies for role modeling and supervision are the most important aspects of leadership (
17,
18).
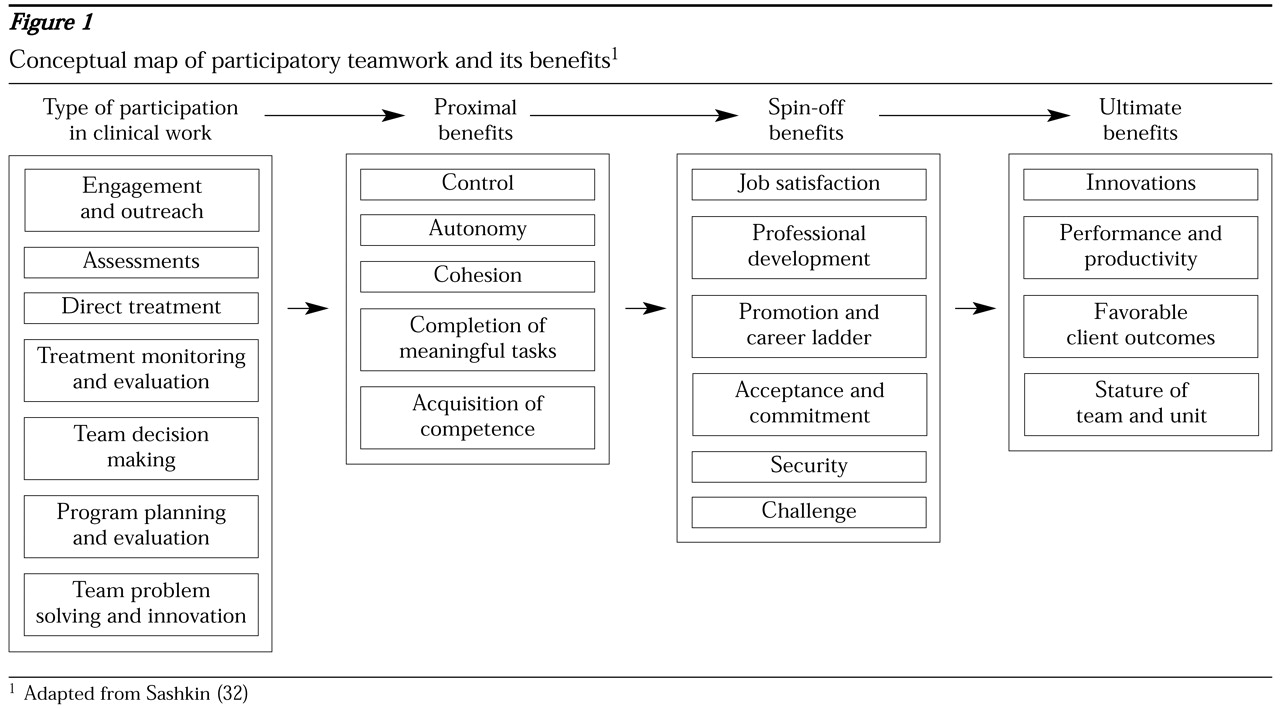
The conceptual map shown in
Figure 1 highlights some of the attributes of participative multidisciplinary teamwork that can promote clients' progress toward optimal levels of independent role functioning and quality of life. When the team's leadership encourages members' participation and shows respect for their expertise in goal setting, problem solving, task assignments, and decision making, members experience job satisfaction, challenge, control, and productivity, which often go hand in hand with clinical excellence. Clinical excellence requires that members reliably use empirically validated modalities; use of such modalities can be assured only when the team members possess the requisite competencies.
For competent teams to deploy evidence-based services effectively, two objectives must be achieved. First, the team must individualize its services to the needs of each client. Factors to be considered are the client's specific mental disorder and its phase and the client's personal values, cultural norms, and long-term goals. Second, the team must develop mechanisms that enable communication, collaboration, coordination, and problem solving among team members.
Individualization of treatment and rehabilitation
Teams should link treatment and rehabilitation to the type and phase of an individual's disorder and to the person's values and life goals. Most disabling mental disorders have four phases—the acute, stabilization, stable, and recovery phases. Despite the best efforts of multidisciplinary teams, some clients' illness will prove refractory even to evidence-based treatments. Highly specialized services are required for such clients, which teams may have to seek through consultation and referral. The phases do not always unfold in a linear sequence; the course of a disorder is influenced by the continuity, comprehensiveness, and quality of the care provided and is marked by plateaus, relapses, phase shifts, and overlapping loops.
Multidisciplinary teams face major challenges in providing individualized rehabilitation services. First, the time, tools, and knowledge of a client's clinical history that are necessary to identify the phase of the client's disorder are often lacking. Second, even though staff may be competent in providing evidence-based services, such services may not be enough to move clients from the acute phase through the stable phase and to the recovery phase. Third, assembling a full array of individualized services and providing them to the large number of patients typical of most teams' caseloads is a gargantuan task.
A few illustrations of the challenges to individualization of services, and thus to optimal treatment and rehabilitation, will suffice. During the acute phase of a disorder, the types and dosages of psychotropic medications differ from those required during the stabilization, stable, and recovery phases (
19). Similarly, the focus of skills training during the acute and stabilization phases is on illness management, whereas the focus shifts to family relations, recreation, housing, conversation, friendship, and intimacy during the stable and recovery phases (
20).
During acute episodes or exacerbations of symptoms as well as during social or personal crises, more intensive levels of supervision, contact, and intervention are usually necessary. Sometimes a client requires hospitalization or crisis and emergency services. However, administrative and logistical obstacles often interfere with the rehabilitation team's ability to maintain clinical contact and treatment responsibility through the different levels and settings of intervention. One of the breakthroughs of assertive community treatment (
21) is its principle of a single multidisciplinary team maintaining full and indefinite clinical responsibility for providing flexible levels of care. Implementing assertive community treatment is often fraught with difficulties, ranging from problems in recruiting, training, and retaining competent and conscientious personnel to overcoming resistance from agencies, administrators, and clinicians who are entrenched in more traditional modes of service delivery (
22,
23,
24,
25).
Community-based outreach teams should be able to achieve high levels of continuity of care. However, because of the logistical and administrative problems involved, it is likely that for the foreseeable future separate inpatient and outpatient multidisciplinary teams will have to bridge the chasm that exists between acute and brief hospital care and aftercare in the community. One way to improve continuity of care is to empower inpatients with the knowledge and skills they need to make personal follow-up contacts with outpatient staff; in this way, patients serve as their own case managers. The use of the Community Re-entry Module (
26,
27) in private, county, and Veterans Affairs hospitals has achieved this end.
Another challenge to individualizing psychiatric rehabilitation lies in the special competencies required of team members who conduct training in social and independent living skills, coping and problem-solving skills, and supported employment—services that are generally the most valuable during the stable phase of a disorder. Teams are faced with a multitude of questions. Should only specific team members be trained as specialists in these modalities, or should all team members be trained as part-time coaches? How should the team ensure that these trained specialists adhere to the rigorous competency standards required by these modalities? What is the best way to encourage clinicians to broaden their roles from therapists to educators? What is the best way to encourage clinicians to build on clients' assets rather than focusing on symptoms and deficits? What procedures should be established for dealing with clients' crises so that clinicians responsible for skills training or supportive employment will not be distracted from these responsibilities? How should skills trainers and employment specialists best communicate with psychiatrists and case managers to ensure a smooth and reciprocal flow of clinical information among team members?
Facilitating teamwork
The delivery of comprehensive, coordinated, consumer-oriented, and evidence-based services that use an outreach approach presents opportunities to broaden the concept of teamwork beyond the roles of professionals and paraprofessionals of conventional disciplines. The broader concept includes clients, their families, and other members of the client's social support network. When the rationale for having an extended team is explained to clients, few obstacles to the sharing of appropriate clinical information will be encountered.
Several critical elements of a multidisciplinary team will facilitate teamwork. First, the team must bring together people who possess the requisite expertise; a team member's discipline may foster acumen in a particular expertise. For example, the practical and behaviorally oriented training and experience of many occupational therapists may prepare them to be particularly effective in conducting skills training. Second, the team must integrate the different areas of expertise at the level of service delivery. Third, mechanisms for accountability for achieving favorable outcomes for clients must be established. Finally, versatility among team members should be cultivated, so that the team encompasses flexible levels of intervention to meet the individualized needs of clients.
Effective rehabilitation teams have a common frame of reference—for example, they acknowledge the importance of using consumer-oriented treatment and involving families and other persons in the client's natural support network. Effective mental health teams also have a common treatment philosophy—for example, they value skill building and provision of supports. Effective teams also share a commitment to implementing evidence-based services and evaluating them. In addition, teams must be empowered by agency managers and policy makers to make their own clinical decisions and decisions about hiring, staff training, programs, and organizational structure. Only through decentralized responsibility and accountability can teams successfully evolve in an era of flux and challenges. Such challenges include dealing with changes in financing and delivery of services and changing clinical populations, problems, and priorities.
Team communication
As Casey Stengel once said, "It's easy to get good players. Getting them to play together is the hard part." The concept of multidisciplinary teamwork is a vision in search of practical tools. Teamwork requires an efficient means of communication about patients' goals, progress, and problems. Team leaders must possess leadership skills that include being able to organize and lead a productive team meeting and maintain cohesion and morale among team members. Leaders must help meet the personal and professional needs of team members, making decisions about clinical assignments, scheduling work and vacation time, and helping team members avoid burnout. Leaders must also provide team members with mechanisms for discussing their concerns and differences of opinion, solving problems, and sharing their expertise. Mechanisms must also be in place to facilitate the exchange of information with community agencies, housing programs, consumers, and families. Finally, leaders must be capable of addressing systemwide economic and sociopolitical challenges to the delivery of comprehensive and coordinated services (
28,
29,
30).
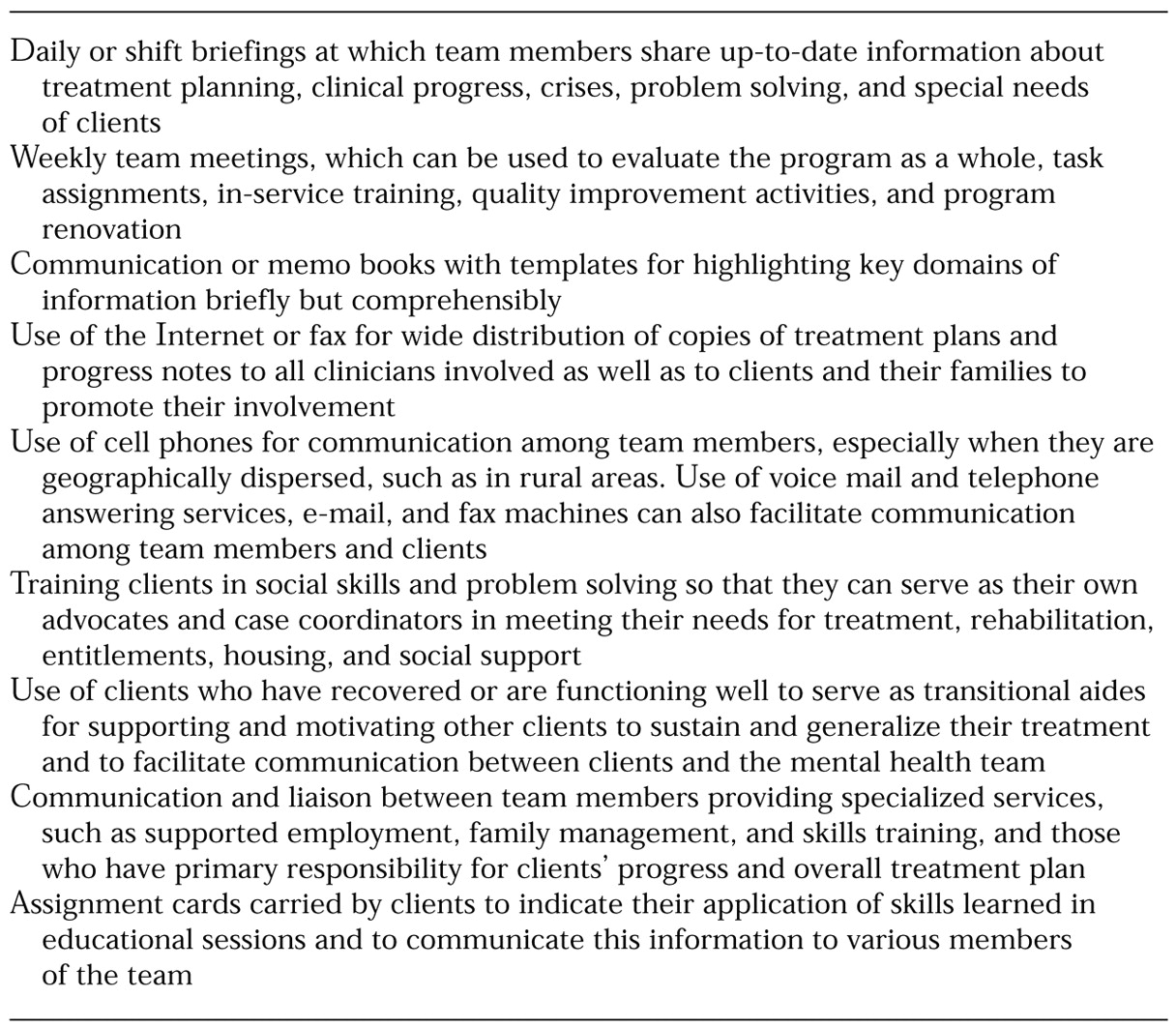
Table 2 presents examples of how these challenges to communication have been met. These examples may help readers develop creative solutions to problems they encounter in attempting to implement and improve multidisciplinary teamwork.
Theory and empirical research in organizational psychology and management can help multidisciplinary teams cope with the challenges of leadership, cohesion, and communication (
31,
32,
33). For example, organizational theory suggests that the team's professionals use their time more effectively when they teach and supervise case managers rather than when they attend numerous administrative meetings, have individual contact with clients, write in medical records, and prepare reports (
34). Such a reformulation of the professional's role has three advantages: it extends the clinical impact of limited professional resources; it enables direct, face-to-face modeling of skills and feedback to staff members who have the greatest contact with clients; and it frees time for services—time that might otherwise be consumed by lengthy staff meetings.
In the teamwork model of psychiatric rehabilitation, information about clients' progress is obtained from regular monitoring, preferably in community settings in which clients live, work, and socialize. When procedures for monitoring the quality of assessments and interventions are structured, well defined, and infused with positive reinforcement and when team leaders encourage initiative, problem solving, and decision making by team clinicians, the participation and morale of the team can be raised (
6). Although the professionals designated as supervisors or team leaders are ultimately accountable for service delivery, everyone on the team shares the responsibility for outcomes.
Supervisory monitoring and feedback do not obviate the need for regular staff meetings, which all team members should attend. How such meetings are led will determine the fruitfulness, value, and efficiency of communication among team members (
35). As the chairperson of staff meetings, the team leader focuses the meeting on the needs of clients, on how current services are addressing those needs, and on making changes in treatment plans as needed; ensuring that team members keep clients' goals paramount when they evaluate clients' progress and plan interventions; setting expectations that the reports presented at meetings by team members will be specific and cogent; involving staff in prioritizing the topics and clients for discussion as well as in problem solving, decision making, and treatment planning; and translating the decisions made at the meetings into the written clinical records.
The use of more frequent meetings, such as morning briefings in which the most current information about clients is distributed, has become the mainstay of communication on assertive community treatment teams. Another example of team communication and coordination is provided by community support programs, in which the client, the case manager, and a family member or other support person meet periodically. At these meetings, the psychiatrist team leader writes a formal contract on the client's medication regimen that delineates the responsibilities and benefits for each person signing the contract. The contract is attached to the client's bedroom wall or refrigerator, and modifications are made as information accrues over time from follow-up meetings (Hartwig D, personal communication, 2001).
One innovative method recently used to improve communication among team members and clients involves the use of personal digital assistants by psychiatrists on a large county-operated inpatient and crisis unit (
36). Hand-held computers used in tandem with desktop units allow rapid and reliable distribution of information about treatment planning and evaluation to all staff.
In a geographically dispersed rural catchment area, one assertive community treatment team used cell phones to keep all team members abreast of the daily changes in the clinical status and psychosocial needs of consumers (
37). This practice enabled the team to flexibly deploy its personnel, to offer more intensive supervision and assistance to clients in crisis, and to keep most of the team's clients living in the community.
Team members' roles
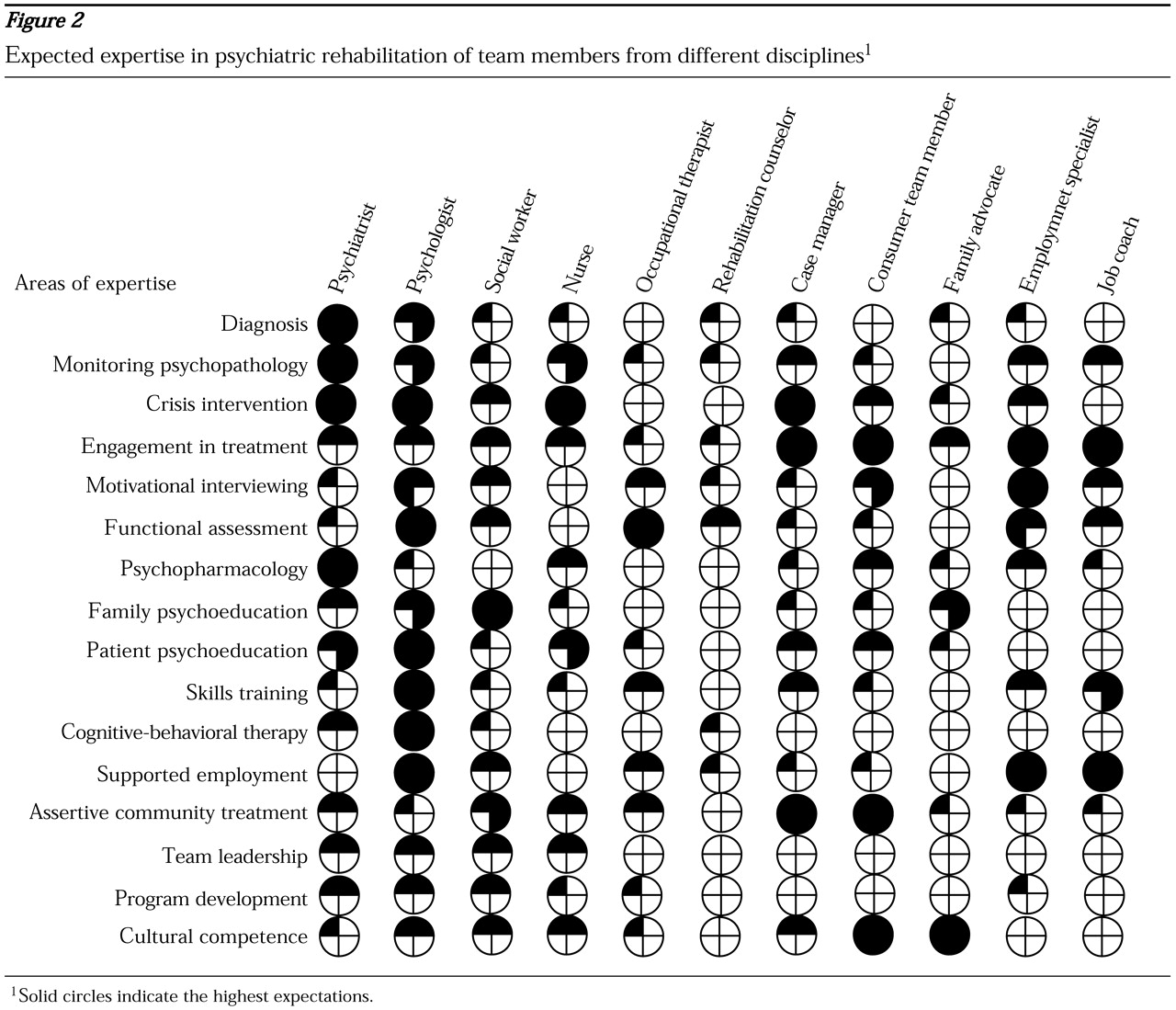
A well-functioning team contains specialists with expertise in critical areas, such as assessment and treatment of medical disorders and psychopharmacology, reliable diagnosis and ongoing assessment of the psychopathology of severe mental illness, functional assessment, management of substance abuse, skills training, employment services, housing, family psychoeducation, and access to entitlements and benefits. The emphasis on specific areas of expertise may vary with the nature of the population. For example, a team serving homeless persons must have members with knowledge about motivational enhancement, engagement of reluctant clients and clients with challenging diagnostic profiles, Social Security entitlements, representative payees, housing, and substance abuse.
Figure 2 summarizes the expertise that may be expected of members of the rehabilitation team from different disciplines. The knowledge and skills of different team members may overlap. Each member shares his or her areas of expertise through training, clinical experience, consultation, everyday interaction, and commitments to mutual clinical responsibility.
Team members' roles are also influenced by the level of complexity inherent in many of the functions of the multidisciplinary team. Minimal expertise and training are required to assist a client with tasks such as shopping and taking medications. On the other hand, teaching social skills and drug-refusal skills requires a higher level of expertise. An even higher level of expertise is required to conduct interventions such as dialectical behavior therapy and cognitive-behavioral therapy for clients who have posttraumatic stress disorder or refractory psychotic symptoms (
38,
39,
40). Management of comorbid disorders requires certain team members to possess highly specialized knowledge and skills (
30,
41).
Medical personnel
The different areas of expertise required for effective psychiatric rehabilitation do not necessarily correspond to specific disciplines. However, certain areas of expertise are more in the province of one team member than another. For instance, diagnostic, medical, and pharmacological knowledge and skills require a medically trained professional, such as a psychiatrist, nurse, clinical pharmacist, or physician's assistant. Because nurses generally have more opportunities to interact with and observe clients who are taking medication, it is particularly important for them to be trained to recognize and monitor the therapeutic effects of medications and their side effects. Nurses can promote long-term adherence to medication regimens if they are trained to use educational programs that promote clients' informed collaboration rather than their passive compliance (
42).
However, it would be a mistake to underestimate the importance of the psychiatrist's role in educating clients and their families. Clients and their family members and community supporters, as well as the members of the treatment team, value the expertise of psychiatrists and their status. When psychiatrists participate in the educational process, clients are more likely to attend educational sessions and use information about medications. Much can be accomplished by psychiatrists if they reengineer their interactions with clients to include information about how medications are selected and how to understand and monitor the prophylactic and therapeutic effects of medications. A collaborative empiricism can be established if psychiatrists encourage clients to give them feedback about how medications help or hinder them from achieving their personal goals. Because of the special role of psychiatrists in rehabilitation and their increasing presence in public mental health programs (
43), a separate section below addresses their contributions to the multidisciplinary team.
Psychologists and social workers
Psychologists and social workers possess important skills in community organization, advocacy for program development, interagency collaboration, and community liaison and consultation. Psychologists and social workers whose postgraduate training has emphasized principles of consultation, community mental health, and community organization are particularly likely to have these skills. In general, psychologists, especially those who have been trained in empirically validated psychosocial treatments, have the greatest knowledge and the most skills in the application of structured interventions with families, skills training, and cognitive-behavioral therapies. Among the team members, they are also the most likely to have training in formal evaluation of clients. Social workers are usually more attuned to the needs of families and are best able to help clients obtain housing and financial entitlements.
Rehabilitation counselors
The discipline of rehabilitation counseling is more than 75 years old. However, these professionals have used their specialized knowledge of matching a disabled person's assets and deficits to job requirements almost exclusively for people with physical disabilities. Every state in the United States has a department of rehabilitation that receives funding from federal grants and state appropriations. But rehabilitation counselors rarely have the expertise to assist clients with psychiatric disabilities. Moreover, only recently, after a stinging rebuke of the Rehabilitation Services Administration by the National Alliance for the Mentally Ill (NAMI), have state rehabilitation agencies begun to work in an integrated fashion with mental health teams (
44,
45).
With the encouragement of advocacy organizations such as NAMI, demonstration programs are being implemented to establish closer links between the vocational rehabilitation and mental health systems (
46). It will be interesting to see whether policy, bureaucratic, and personnel barriers to collaboration can be overcome. Recent attempts to build bridges between substance abuse and mental health agencies are not encouraging to interagency teamwork. Because most rehabilitation counselors have traditionally offered services from offices that are geographically separate from mental health teams, the new and more effective supported employment programs have been primarily staffed by employment specialists and job coaches who are hired by and closely integrated with the mental health teams whose clients they serve.
Occupational therapists
The field of occupational therapy grew up with a conceptual framework (
47) and a hospital-based practice for diversional activities that were successful in engaging patients but that rarely had carryover effects in job finding and job tenure (
48). If the field of occupational therapy is to target clients with psychiatric disabilities as effectively as it has targeted those with physical disabilities, it must provide its students and practitioners with expertise in using manual-based and evidence-based technologies, such as skills training and supported employment (
49,
50).
Case managers
Ideally, case managers have three distinct sets of competencies: clinical skills, relationship skills, and liaison and advocacy skills. Clinical skills include treatment planning, symptom and functional assessment, and skills training. Relationship skills include the ability to forge and maintain a collaborative, supportive, mutually respectful therapeutic alliance with clients of all types. Liaison and advocacy skills are necessary to develop and maintain productive interagency contacts for housing, financial entitlements, and vocational rehabilitation. The comprehensive repertoires of case managers can help them maximize their effectiveness. Effective case managers share responsibility and accountability in their areas of functioning, they have trust and confidence in one another's clinical judgment and seek out technical assistance and supervision from team members with more specific areas of expertise or more clinical experience. They are always ready for mutual assistance, and they expect to learn from other case managers and professional colleagues throughout their career. These characteristics of case managers breed successful outcomes for the team's clients
Specific and generalrehabilitation competencies
Representatives of the traditional mental health disciplines can contribute to the implementation of integrated and individualized services. However, to do so they must have specific expertise—or competencies—to help ensure that the team achieves positive clinical outcomes. Contemporary competencies were rarely taught when most currently employed mental health professionals were enrolled in their specialty training. In addition, most currently employed mental health workers have had little or no experience in the type of community-based teamwork described here.
The competencies necessary to deliver evidence-based care fall into four realms: attitudes and emotions; clinical wisdom and experience; generic therapeutic and relationship skills; and knowledge about and abilities in diagnosis, psychopathology, psychopharmacology, family and social systems, cultural competence, psychosocial interventions, and other technical aspects of assessment and treatment.
The first three realms can be viewed as general competencies that cut across the more specific competencies driven by evidence-based modalities. General competencies include personal attributes and relationship skills that are not easily taught but are the matrix within which more specific competencies are supported. Relationship skills include empathy, tolerance of ambiguity and individual differences, genuine concern, warmth and enthusiasm, realistic optimism about prospects for improvement, and respect for a client's strengths, unique qualities, and goals.
Specific evidence-based competencies for one of the rehabilitation services shown in
Figure 2, social skills training, include the ability to elicit information about clients' goals for skill development and to help clients set realistic goals in areas of their assets, deficits, and previous accomplishments; the ability to use motivational enhancement to engage clients in training; the ability to use social learning principles in teaching skills; and the ability to conduct outreach with natural supporters for promoting generalization of skills. Few individuals on a rehabilitation team are likely to possess all these competencies; however, it is important for all team members to at least be familiar with most of them and to demonstrate respect for one another's areas of specialization.
The role of the psychiatrist in rehabilitation
Because serious mental disorders are biomedical conditions that require accurate diagnosis, medicolegal decisions, and pharmacological treatments, the role of the psychiatrist is of special importance on a mental health team. In recent years, psychiatrists and their professional groups have asserted their unique value to multidisciplinary teams in clinical, organizational, administrative, and legal arenas. For example, the formation of the American Association of Community Psychiatrists was in large measure a reaction against the marginalization of psychiatrists in community mental health (
51). Health maintenance organizations and public mental health authorities have been criticized for using nonpsychiatrists to carry out essential medical activities.
However, the lack of full participation by psychiatrists on rehabilitation teams has come about partly by default. Because psychosocial services and long-term supportive relationships with clients have been delegated to nonmedical personnel, most psychiatrists have not been trained in these areas or their skills have become "rusty." In addition, many psychiatrists do not have the interpersonal skills or inclination to participate on multidisciplinary teams, let alone to lead them.
Given the fact that psychiatrists have designed innovative services and have made notable contributions to treatment and rehabilitation (
21,
52,
53,
54,
55,
56,
57), it is clear that psychiatrists can be active participants on, and even leaders of, multidisciplinary teams. There is no question that a large number of psychiatrists are needed in the rehabilitation field. However, if psychiatrists are to gain the respect and the key roles to which organized psychiatry aspires (
58), they will need to acquire general and specific competencies for effective professional functioning on multidisciplinary teams.
General competencies that are particularly valuable for psychiatrists as leaders of multidisciplinary teams include attributes such as persistence, realistic optimism, a collaborative style, teaching ability, and networking and system coordination skills. Psychiatrists can also act as role models for teams by demonstrating that boundaries between "medical" and "psychosocial" are illusory and that these areas of expertise must be integrated in the care of clients.
Psychiatrists who work with persons with severe mental illness and who wish to contribute as key members or leaders of their teams must go beyond their prescription pads to acquire knowledge, attitudes, and skills congruent with contemporary practice guidelines for psychiatric rehabilitation; giving respect and support to multidisciplinary team members and gaining their respect and support in return; coping with large caseloads; collaborating with agencies and programs to ensure continuity, consistency, and coordination of care; and valuing the roles and expertise of staff who provide case management, supported employment, skills training, and family and housing supports. If psychiatrists can incorporate these attitudes and skills, they can expect reciprocity and cohesion from other team members, and clients will benefit.
Psychiatric residents receive little competency-based training and have limited experience in teamwork, psychiatric rehabilitation, and community mental health. Thus acquiring the organizational and communication skills needed for effective teamwork may be a daunting challenge for psychiatrists. Mentoring, training, and clinical experience can build on a psychiatrist's generic skills in this area. Several competencies can readily be learned, such as effective ways to conduct and lead a multidisciplinary team meeting and techniques for developing collaborative therapeutic relationships with clients and families.
Psychiatrists who wish to make substantive contributions to a rehabilitation team should have a working knowledge of the changing scene of evidence-based interventions. Even if psychiatrists who wish to lead a team do not regularly conduct skills training or family psychoeducation or provide supported employment services, they should have knowledge and competence in these areas. More important, because leadership involves role modeling, the psychiatrist-leader should be able to demonstrate (and supervise) certain psychosocial interventions capably and confidently to clients, families, and colleagues.
Although the psychiatrist's profile of competencies may concentrate on the "bio" component of biobehavioral assessment and treatment, indifference to other modalities of rehabilitation will be the death knell for psychiatric leadership of a team. The triad of competencies described earlier for case managers—clinical, relationship, and liaison and advocacy skills—is a reasonable framework for a psychiatrist who desires more professional diversity and satisfaction. Surveys of psychiatrists working in the public sector have revealed that those who have a wider array of responsibilities and competencies are most satisfied with their roles; for example, a mix of clinical, consultative, supervisory, educational, and administrative duties appears optimal (
59). Among the activities most highly correlated with satisfaction are teaching, supervising, and consulting with clients, families, colleagues, agencies, and other stakeholders in the system of care.
Evidence-based modalities of psychiatric rehabilitation
The accumulation of scientific evidence has fostered the development of practice guidelines and treatment algorithms in the delivery of individualized services by multidisciplinary teams (
20,
21,
60). Professionals from all mental health disciplines must acquire the competencies necessary to provide evidence-based interventions and to deliver them in ways that are appropriately linked to the nature or phase of an individual's disorder. These competencies can be acquired through continuing education, in-service training, ongoing supervision, quality improvement activities, and revised postgraduate curricula.
Atypical or novel antipsychotic drugs are now considered first-line treatments for the various forms and phases of schizophrenia. The introduction of these drugs challenges psychiatrists and allied mental health professionals to use multidisciplinary teamwork in selecting and titrating medications with varied side effect profiles, tolerability, and efficacy for positive and negative symptoms and neurocognitive impairments. Case managers and other nonmedical team members, who have more opportunities than psychiatrists to observe clients, need mechanisms to convey information to psychiatrists about how pharmacotherapy is affecting a client's symptoms and neurocognitive and psychosocial functioning so that psychiatrists can make informed decisions about the types and dosages of medications to prescribe for a given client. In addition, teams can make good use of novel antipsychotic agents only when psychiatrists have regular opportunities to educate nonmedical clinicians about the efficacy and side effects of medications.
However, medications are not used in a socioenvironmental vacuum; they are necessary but not sufficient for achieving good outcomes. Clients cannot learn social and independent living skills by taking a medication, nor can they become reliable and informed consumers of medications without educational programs. Therefore, multidisciplinary teams must implement empirically validated illness management programs, such as the Medication and Symptom Management Modules (
61,
62). A variety of models are available for educational approaches to facilitate adherence to treatment and continuity of care, including the cost-effective use of nonprofessionals and paraprofessionals to augment a team's limited professional staff (
63,
64,
65,
66).
When teams combine judicious types and dosages of medication with family psychoeducation and skills training, outcomes include better continuity of care, protection from relapse, and higher levels of social functioning (
26,
67,
68,
69,
70), which help clients move into stable and recovery phases. Such interventions require close collaboration between the team's prescribing psychiatrist and the team members who provide educational services. Thorough assessment is necessary to individualize a client's education and to match the training to the client's needs. The team members who are best prepared to obtain additional expertise in psychoeducation and skills training are psychologists, psychiatrists, social workers, occupational therapists, and psychiatric nurses.
Some evidence-based programs have been specifically designed for use by well-trained experts on multidisciplinary teams, including the Optimal Treatment Program (
71), dialectical behavior therapy for borderline personality disorder (
38), integrated programs for clients with a dual diagnosis of a psychiatric disorder and a substance use disorder (
30,
41,
72), the Program for Assertive Community Treatment (PACT) (
21,
60,
73), and individual placement and support for supported employment (
25,
74,
75). Although PACT, dialectical behavior therapy, and individual placement and support specify the roles of team members and describe the interdisciplinary process required to implement these interventions, other evidence-based interventions give more latitude to the team.
The programs with more latitude include psychoeducational and behavioral family interventions (
76) and various skills training programs, including the video-assisted modules for teaching substance abuse management, basic conversation skills, recreation for leisure, workplace fundamentals, friendship and intimacy, and community reentry (
77,
78,
79,
80). Having greater flexibility is a two-edged sword. Although it enables multidisciplinary teams to "reinvent" the modality to fit the team's constraints and resources, it also burdens the team with having to make decisions about who is to do what with whom, when, and where.
The availability of treatment guidelines, manuals, and modules augurs a new era of high-quality care. However, teams must be able to tailor treatments to each individual's specific needs (
81). Because an individual's needs change with treatment, the phase of the disorder, stressors, situations, supports, abilities, and community resources, teams will be more likely to maintain quality of care if they periodically monitor and measure the client's symptoms, needs, and functional capacities (
10,
11,
13,
82,
83,
84,
57). Thus another challenge to a multidisciplinary team seeking to use evidence-based treatments is to integrate assessment methods with the choice and timing of treatments.
Conclusions
As advances accrue in our understanding of the potential for recovery from severe mental illness, rehabilitation practitioners and their teams will have to obtain a broader array of competencies. New modalities are in various stages of development. They include cognitive-behavioral therapy for refractory psychotic symptoms (
85,
86); naturalistic augmentation of skills training (
7,
87); neurocognitive psychopharmacology (
88); cognitive adaptive training and errorless learning, which are aimed at compensating for neurocognitive deficits that interfere with rehabilitation (
89,
90); precision teaching, computerized instruction, and use of the Internet for skills training; greater use of telecommunications and electronic communication for prompting, reinforcing, and problem solving; cognitive remediation (
90,
91,
92); combined skills training and supported employment; and integrated service agencies (
93,
94). These innovations will challenge mental health disciplines to broaden their professional training, roles, and repertoires or face displacement or even extinction. Novel rehabilitation technologies, combined with medications, will also require reconfiguration of multidisciplinary teams in ways that we can hardly anticipate.
Although progress in our knowledge of the biological basis of disabling mental disorders has captured the attention of academics, pharmaceutical companies, practitioners, family advocates, and policy makers, more practical gains have actually been made in improving the course and outcome of schizophrenia and related disorders through innovations in psychosocial interventions and the deployment of multidisciplinary teams for assertive community treatment. Through the development of evidence-based, comprehensive, coordinated, and integrated services, most clients with severe and persistent mental illness now have the opportunity to lead independent, satisfying, and functional lives. Judicious use of antipsychotic, mood-stabilizing, and antidepressant drugs, combined with social skills training, family psychoeducation, and supported employment, can result in optimal outcomes. These services can be effectively delivered through systems of care and multidisciplinary teams.
A key element in achieving favorable outcomes is the active involvement of clients, together with their families and other natural supporters, in the process of treatment planning, intervention, and evaluation of progress. To motivate clients to engage in treatment and adhere to comprehensive treatment regimens, the multidisciplinary team must help them identify personally meaningful goals and demonstrate that collaborating with treatment providers can help them attain their goals.
Because treatment and rehabilitation must be individualized, evidence-based interventions cannot be taken directly from controlled clinical trials and applied to all clients in the same way. Standardized treatments, both psychosocial and pharmacological, not only must be tailored to the individual client but also must be integrated with other services into a coherent package that changes as necessary with the phase of the disorder and the client's goals as treatment proceeds.
Because it is practically impossible for one caregiver to master the entire range of relevant competencies, the optimal vehicle for integrating and adapting diverse interventions is the multidisciplinary team. In the future, more services—and more effective services—will be delivered through teams by specialists with the requisite expertise, just as we have seen in other fields of medicine. The proliferation of effective services will place an even greater burden on mental health team members to learn diverse skills from each other and to share decision making and responsibility for reviewing, integrating, and implementing care plans. Only in this fashion will multidisciplinary teams be able to ensure continuity and comprehensiveness of care, even as individual service providers come and go. Because of acceleration in the development of evidence-based biobehavioral services, the future may hold some surprises for multidisciplinary teams in psychiatric rehabilitation.