Health risk factors among patients who have schizophrenia include cigarette smoking, poor nutrition, polydipsia, hyponatremia, poverty, diabetes mellitus, and obesity (
1). Weight gain is a documented side effect of treatment with antipsychotic medications (
2,
3). Weight gain is detrimental to self-esteem and frequently leads to noncompliance with medication regimens (
4). Of the newer antipsychotics, olanzapine in particular is one of the agents that have been shown to cause significant weight gain beyond what patients may have already experienced as a result of other antipsychotic medications (
5).
No published studies have examined weight loss interventions among patients who have schizophrenia and who have gained weight as a result of treatment with antipsychotic medication. The goal of our study was to determine whether an established weight loss program, such as Weight Watchers, would be successful for patients who had olanzapine-related weight gain. In addition, we were interested in determining whether the severity of patients' psychiatric symptoms was correlated with their success in losing weight.
Methods
The study was conducted from February 4 to April 15, 1999. The participants were outpatients who had been treated with olanzapine for at least six months at a dosage of 15 to 40 milligrams daily and who had gained at least 7 percent of their pretreatment weight. We ruled out other possible causes of weight gain among these patients, including use of other medications for which weight gain is a side effect. All patients had a DSM-IV diagnosis of schizophrenia or schizoaffective disorder. The age range of the patients was 18 to 60 years.
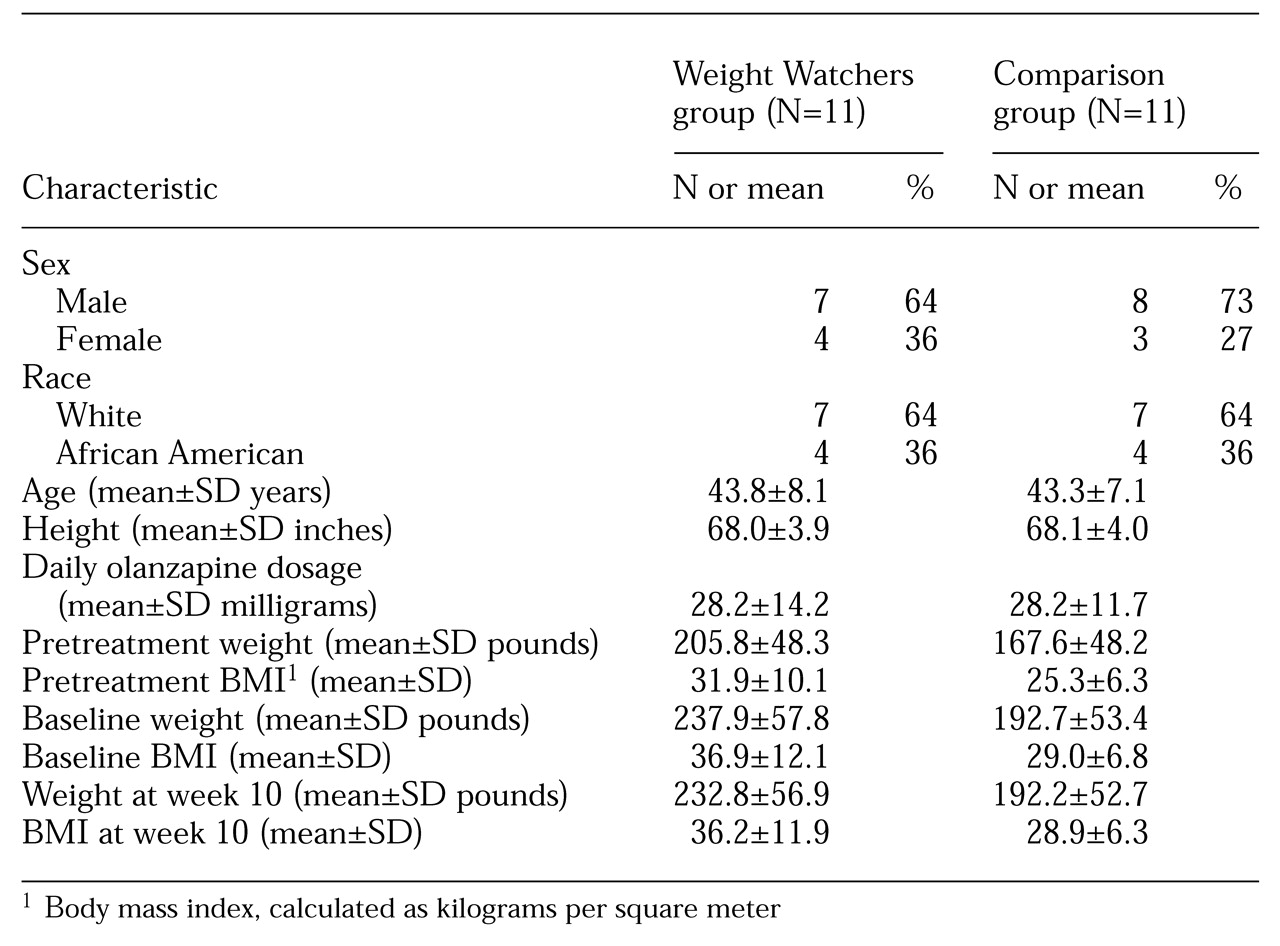
A comparison group was selected from the outpatient research program at the Maryland Psychiatric Research Center and was matched on the criteria described above, as shown in
Table 1. Patients in the comparison group did not participate in the Weight Watchers program but continued their usual olanzapine treatment. All study participants received a full explanation of the study procedures and gave written informed consent before participating in the study.
A physical examination, blood chemistry analysis, urinalysis, an electrocardiogram, and, for the women, a pregnancy test, were performed at baseline. Analyses of percentage body fat and fat mass were conducted at baseline and at the end of the study with a hand-held bioelectrical impedance analyzer. Psychiatric symptoms were assessed with the Brief Psychiatric Rating Scale (BPRS), the Scale for the Assessment of Negative Symptoms (SANS), the Hamilton Depression Scale (HDS), and the Clinical Global Impression (CGI) scale at baseline and at the end of the study. Possible scores on the BPRS range from 1 to 140, on the SANS from 0 to 125, on the HDS from 0 to 80, and on the CGI scale from 1 to 5, with higher scores indicating worse symptoms. The participants' body weight, blood pressure, and body mass index were assessed weekly.
Ten weekly Weight Watchers meetings were held at the outpatient research program of the Maryland Psychiatric Research Center in Baltimore. The basic Weight Watchers program—known as the 1-2-3 Program—teaches participants to use a points system to evaluate food choices. Exercise sessions were scheduled three times a week and were monitored by at least one of the investigators. The type and duration of exercise was recorded for each participant. A parent or caregiver was asked to supervise each patient's diet and exercise at home.
Tokens were used to reinforce exercise and adherence to the diet. The patients were given tokens weekly for weight loss, attendance at the group meetings, participation in the exercise sessions, and documentation from caregivers and family members on exercise and adherence to the diet. The patients could buy gift items with these tokens at an auction that was held after the final Weight Watchers meeting.
A 2×2×2 repeated-measures analysis of variance—Weight Watchers group versus control group, male versus female, and baseline versus the end of week 10—was used to assess changes in weight and body mass index. Paired t tests were used to assess changes in the severity of psychiatric symptoms. Pearson product-moment correlations were used to examine relationships between changes in body weight and body mass index and changes in psychiatric symptoms.
Results
Twenty-one patients agreed to participate in the Weight Watchers program, 11 of whom completed the study. Of the other ten patients, seven withdrew before starting the Weight Watchers program. After the study started, one patient dropped out of the study because of the death of his mother, one dropped out because of transportation problems, and one dropped out because he could not read the written materials. Eight patients participated in the supervised exercise program—six men and two women.
Although participants who completed the Weight Watchers program lost more weight than participants in the comparison group, no significant differences were noted in weight changes or changes in body mass index between the two groups. A significant sex by group by time interaction was observed for body mass index (F=4.31, df=1, 16, p=.05). Therefore the weight and body mass index data for men and women were analyzed separately.
All seven male participants lost weight. The mean±SD weight loss for the men was 7.31±5.87 pounds (median, 7.6 pounds) (F=4.88, df=1, 11, p<.05); weight loss ranged from one pound to 18 pounds. A nonsignificant difference in body mass index was observed between the two groups (1.05±.87 lower in the Weight Watchers group; range, .16 to 2.75). Three of the four women gained weight; the other woman lost 13.2 pounds. The overall change in body weight and body mass index for the women was not significant.
The participants' exercise sessions increased from a range of five to ten minutes, walking about .1 mile, at the start of the program to 25 minutes, walking about one mile, at the end of the program. No significant correlation was found between exercise participation and weight loss.
The patients remained clinically stable during the study: mean±SD scores on the BPRS were 29.09±6.90 at baseline and 31±9.62 at week 10; scores on the HDS were 7.36±5.48 at baseline and 6.81±6.75 at week 10; scores on the SANS were 19.54±5.90 at baseline and 19.81±8.64 at week 10. No significant differences were observed between the baseline and week 10 scores.
Discussion
The men in this study who adhered to the Weight Watchers 1-2-3 Program lost a significant amount of weight. The high correlation between the mean and median weight loss suggests that the significant mean weight loss was not likely to have been the result of an outlier. For the women in the study, weight loss was not significant. Psychiatric symptoms prevented two of the women, who did not lose weight, from adhering to the program; however, no significant associations were found between psychiatric symptoms and weight loss.
The Weight Watchers and exercise programs were well tolerated. The Weight Watchers leader reported that the success and dropout rates were similar to those of other groups that she had worked with in the community. The only population-specific modification that was made to the program was to change the recommendation to increase fluid intake; because of the risk of polydipsia among patients who have schizophrenia, an increase to no more than 80 ounces a day was recommended. Attempts to monitor the patients' diets were made, although such monitoring is difficult among outpatients.
The primary mode of exercise was walking. The maximum duration of exercise sessions that the participants achieved—25 minutes three times a week—is still below the recommended guideline of 45 to 60 minutes three times a week for weight loss. Longer sessions may help patients achieve an exercise level that is optimal for weight loss. No adverse events were observed with either the diet or the exercise program. The patients' vital signs remained stable during the study.
Conclusions
The results of this study indicate that weight loss strategies may be successful among patients with schizophrenia who have olanzapine-associated weight gain. The health risks of being overweight are an important consideration in evaluating medication choices for patients who have schizophrenia. To control medication-induced weight gain, patients need to be educated about appropriate strategies for managing this side effect. The approach to weight loss that was used in our study was not associated with any adverse effects. Thus further implementation of this or similar approaches may be worth the consideration of health care professionals.
Additional controlled studies are needed to confirm our results; to determine, in the context of longer studies, the extent to which weight loss is possible through the use of a combined Weight Watchers and exercise program; and to examine the potential benefit of combining this program with weight control medications.
Acknowledgment
This work was supported in part by grant MH-40279 from the National Institute of Mental Health and a research grant from Eli Lilly and Company.