Literature on the lack of trust between behavioral health care professionals and managed care administrators shows that health care organizations have been challenged about their commitment to best practices (
1). Clinicians report pressure by health care managers to discharge patients prematurely (
2), and concerns have been raised about limited access to psychosocial services (
3) and lack of coverage for community-based services (
4)—all important factors for maintenance of therapeutic gains. At the same time, a growing interest has been noted among behavioral health care managers in developing measurable standards for monitoring quality of care, access, effectiveness, and consumer satisfaction (
5). Consequently, there is a need to improve communication among all concerned parties on substantive matters pertaining to needs assessment and the quality and availability of services.
Few studies have focused on the psychometric properties and clinical utility of the Global Assessment of Functioning (GAF) scale, despite widespread use of the scale among practicing psychiatrists to assess patients' overall level of functioning (
6). Various articles have questioned the validity, clarity, and utility of the scale from a multiaxial perspective (
7). At the time these studies were conducted, the multiaxial integrative approach to axis V was not in use, as evidenced by the exclusion of axis IV psychosocial data relevant to full recovery and maintenance of remission. The purpose of this study was to revisit the utility of the
DSM-IV GAF scale for improving interdisciplinary communication about patient care.
Methods
The study was conducted in the adult mental health service section of a state psychiatric inpatient facility that was not affiliated with a university. The service comprised one six-bed temporary-observation unit (discharge within 72 hours of admission or transfer to another unit), one eight-bed crisis-intervention unit (discharge within seven days of admission or transfer), four 28-bed intermediate-stay units (discharge within 14 days), a unit for long-stay patients (up to 30 days), and a unit for medical psychiatry patients (beyond 30 days' stay). The patients who participated in the study were 92 women and 73 men between the ages of 18 and 68 years who were consecutively discharged during the study period (September to December 1997).
The computer-based GAF Scale Report (
8) is designed to provide mental health professionals with an explicit set of steps that follow the
DSM-IV axis V decision-tree process of deriving a GAF score. Accordingly, symptom severity and functional levels are considered in assessing all aspects of patients' functioning: psychological, social, and occupational. A GAF rating range is automatically calculated on the basis of this information. Within a given 10-point range, a patient's GAF score can be determined by using clinical judgment and hypothetical comparisons with patients in the same range. (Possible scores on the GAF range from 0 to 100, with higher scores indicating better functioning.)
All unit psychiatrists and attending psychiatrists (eight psychiatrists in total) generated GAF scores on the basis of their clinical impressions of patients. On the assumption that clinical-impression-based and computer-generated GAF scores involve the same decision-tree process, the psychiatrists attended a session to familiarize themselves with the computer software used to generate GAF reports so that a single baseline could be ascertained for both disciplines. Unit and staff social workers (N=13) participated in the study. They lacked previous experience with GAF assessments and received four sessions of training in generating computerized GAF reports.
The hospital's chief psychologist conducted the training for each discipline. The social workers completed computer-generated GAF reports for their patients no more than 24 hours before the start of the psychiatric discharge process and routinely transmitted the reports to the chief social worker. While routine collaborative treatment teamwork was in process, the psychiatrists and social workers agreed to refrain from discussing each other's GAF rating until the completion of the discharge note by the psychiatrist.
Spearman's correlations were used to test associations between the study variables. The paired t test and the nonparametric signed-rank test, respectively, were used to test differences between normally and abnormally distributed GAF scores obtained by the two disciplinary groups. Kappa agreement indexes were used to examine agreement between scores on various GAF categories. All analyses were conducted on dependent samples only. The tests were two-tailed, and a p value of .05 or less was considered significant. The data were analyzed with SAS software.
Results
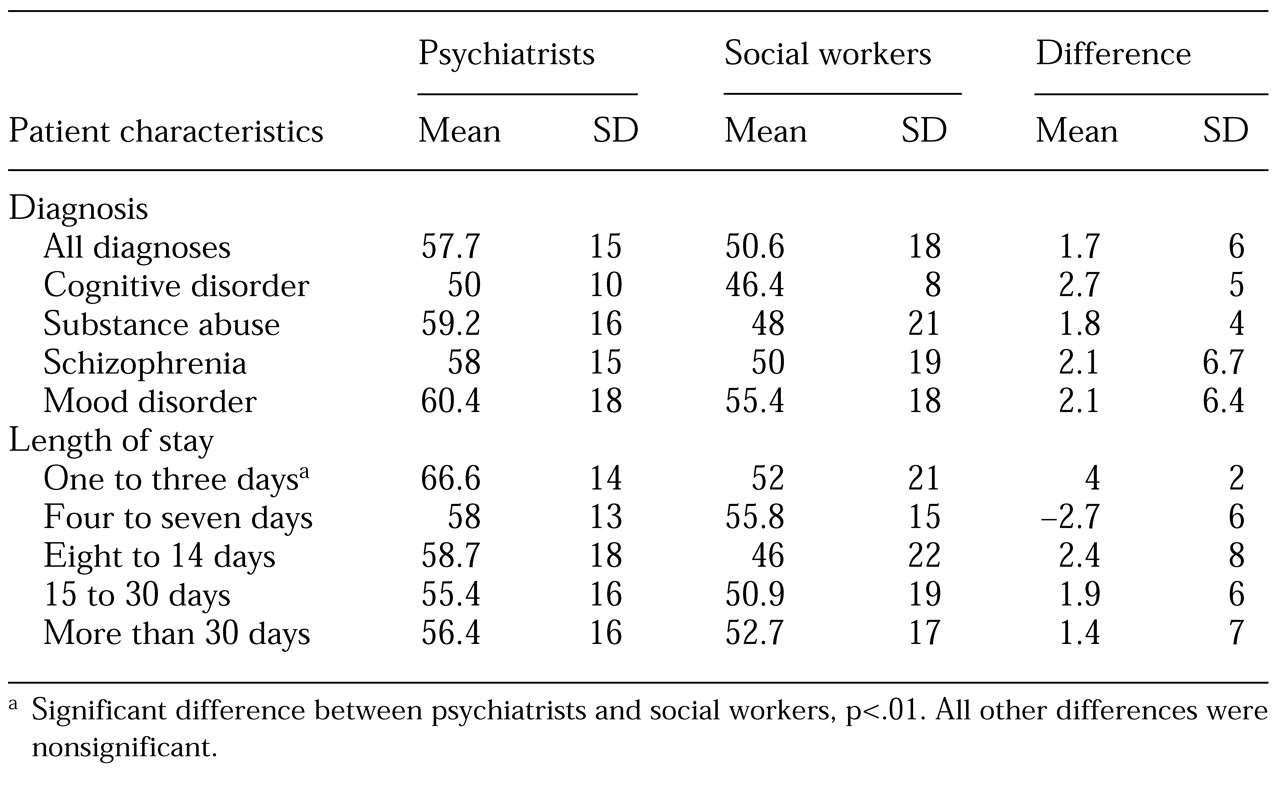
As can be seen in
Table 1, discharge GAF scores derived by psychiatrists and those derived by social workers did not differ significantly across diagnostic groups. A high, significant correlation was found between GAF scores derived by psychiatrists and those derived by social workers (r=.93, p<.01). No significant differences were found between the GAF scores of psychiatrists and those of social workers for patients with various lengths of stay, except in the case of the shortest stays (one to three days), for which the mean value of the GAF scores derived by the psychiatrists was higher than that of the scores derived by the social workers. To calculate the kappa agreement index, the GAF values were divided into three categories: 10 to 35, 36 to 55, and 56 or above. The kappa index was .85 (95 percent confidence interval, .78 to .91), which is considered to be very high. When the same index was calculated by dividing GAF values into two groups (below 50 and 50 or above), the kappa index was .86 (CI, .77 to .94), also considered very high. The calculated power (beta) was 74 percent.
Discussion and conclusions
The high reliability of discharge GAF scores obtained by social workers and by psychiatrists, observed across all diagnostic groups and most categories of length of stay, suggests that social workers, after receiving systematic training in computer-based GAF reports (
8), can provide reasonable assessments of clients' functioning. Only for patients with the shortest length of stay—one to three days—was interdisciplinary reliability absent. This finding may have been due to the fact that hospital policy exempted interdisciplinary treatment teams from conducting individualized treatment planning meetings that also addressed discharge considerations for these short-stay patients. Consequently, these patients, unlike those who had longer stays, did not benefit from an enhanced integrated understanding by the interdisciplinary treatment team. Professionals of each discipline maintained their respective impressions about patients' readiness for discharge, compromising interdisciplinary agreement on discharge GAF scores.
A lack of interdisciplinary agreement can have several negative consequences. From a patient care perspective, disagreement about patients' readiness for discharge may result in premature discharge and an increased risk of readmission, which has itself been associated with deterioration in mental health (
9,
10). From the perspectives of disease prevention, health promotion, and cost-effectiveness, a lack of investment in interdisciplinary collaboration for short-stay patients may result in cost-ineffective care in terms of continuity of preventive care. Policy-based interdisciplinary exchange of information about biopsychosocial factors associated with admission and readiness for discharge among short-stay patients can reduce the risk of readmission.
From an organizational perspective, a lack of interdisciplinary agreement about patients' readiness for discharge may compromise accountability for treatment decisions and outcomes among interdisciplinary team members, which can affect the general collaborative practices of the treatment team and consequently compromise the quality of patient care.
Interdisciplinary exchange of factual information is essential for a balanced, integrative formulation of GAF scores and thus should not be viewed as a source of bias in this study. Such exchange does not render other DSM-IV axes redundant. The results of the study highlight this fact: GAF scores differed significantly across disciplines when opportunities for such exchange did not exist. The GAF scale may facilitate reliable interdisciplinary communication across treatment settings and among health care provider organizations, including behavioral and medical managed care organizations with an interest in positive treatment progress, outcomes, and monitoring remission.