Persons with psychiatric illnesses are about twice as likely as the general population to smoke tobacco (
1), and those with schizophrenia are three or four times as likely (
2,
3). Alcohol and drug abuse are also strongly associated with a high rate of smoking, with prevalence estimates ranging from 71 to 100 percent (
4,
5,
6). Compounding the high prevalence of smoking is the fact that individuals who are mentally ill or have substance dependence tend to smoke much more heavily than smokers in the general population (
1).
Both neurobiological and psychosocial factors are thought to reinforce the use of nicotine in psychiatric populations (
7,
8). For many people with persistent mental illness, smoking is a major part of their daily routine and constitutes an activity that provides some structure to a day with few activities. Smoking also has long been considered an integral part of the psychiatric culture. Moreover, clinicians often believe that persons with mental illness are not able or willing to quit. Increasingly, however, health care facilities are implementing and enforcing smoking bans on their premises. These policies have heightened interest in outcomes of smoking cessation strategies for persons with mental illness or addictions.
Methods
We undertook a critical review of the literature to assess the impact of smoking cessation approaches on individuals with mental illness or addictive disorders. We conducted searches of large health care and other databases using the key terms smoking, smoking cessation, nicotine, health/ hospital/smoke-free policy, and psychiatry/mental/substance abuse disorders. The databases and the year spans used were MEDLINE, 1997-2000; CINAHL, 1990-2000; PsycINFO, 1990-2000; Best Evidence, 1991-2000; Healthstar, 1996-2000; Cochrane Database of Systematic Reviews, 2000; Legal Trac, Bioethicsline, 1973-2000; Philosopher's Index, 1940-2000; and Dissertation Abstracts, 1990-2000.
Many of the papers that address smoking cessation treatment for this population are reviews or discussion papers or are based on anecdotal evidence. We included only studies that presented data on samples of people with diagnoses of specific mental illness or addictive disorders, with no restrictions as to methodology. Broader studies reporting symptomatic subgroups in their analysis, such as persons with depressive symptoms, were not included. Overall, 15 studies were excluded.
Results
Smoking cessation approaches
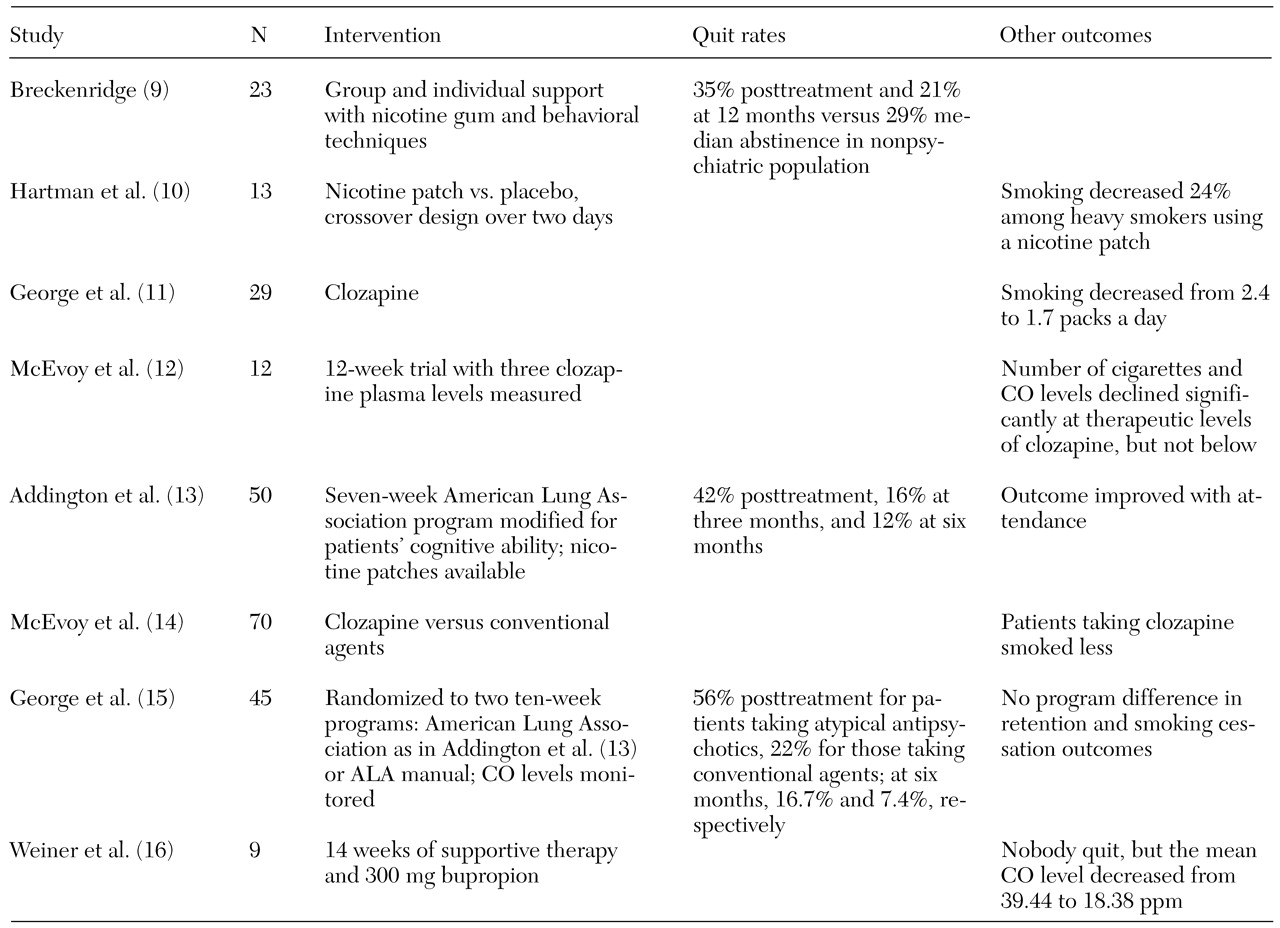
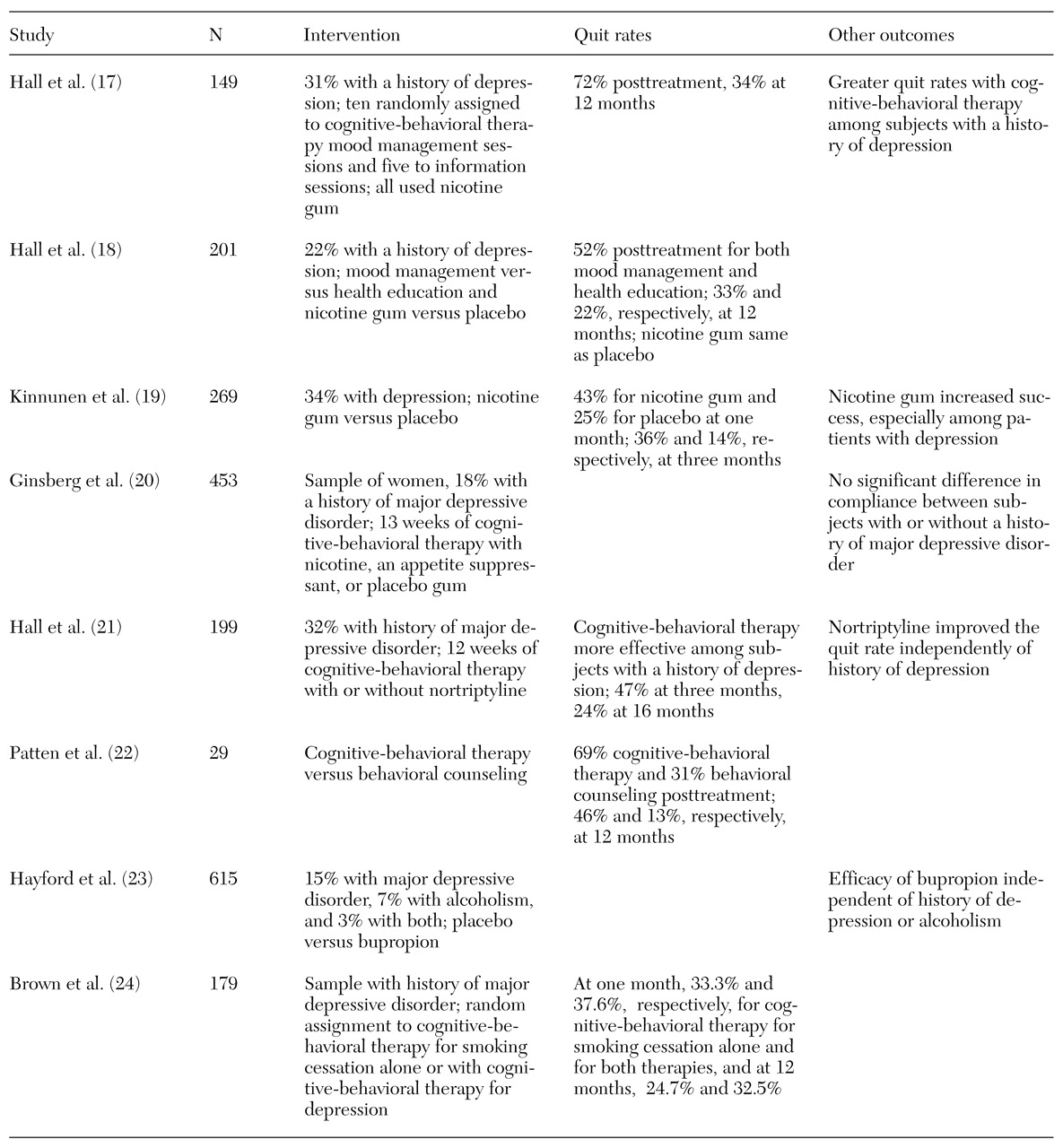
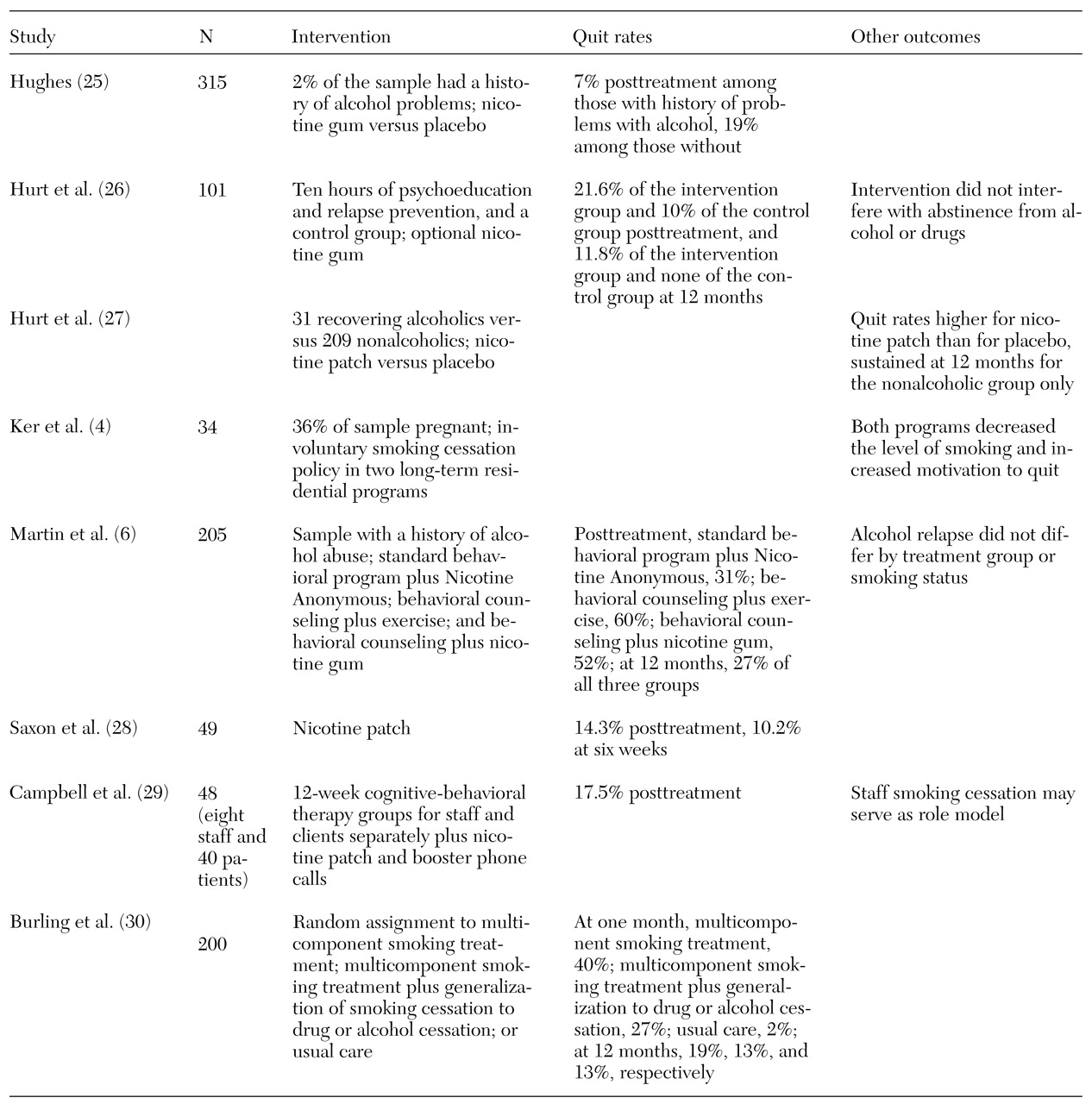
Twenty-four studies addressing the impact of smoking cessation strategies in samples of persons with mental illness or addictive disorders were reviewed. Eight included persons with schizophrenia, eight had substantial proportions of persons with depression, and eight focused on persons with addictive disorders.
Tables 1,
2, and
3 list the studies (
4,
5,
6,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18,
19,
20,
21,
22,
23,
24,
25,
26,
27,
28,
29,
30), the interventions they used, their quit rates, and other outcomes of interest.
The majority of interventions used a combination of medication and educational and cognitive-behavioral approaches. Variables that affected outcome included number of cigarettes smoked per day, duration of previous quit attempts, history of alcohol or drug problems, and confidence about succeeding. The outcomes included quit rates, number of cigarettes smoked, and expired breath carbon monoxide levels. The time intervals for assessment varied from two days to 16 months.
The studies of persons with schizophrenia mostly involved small clinical samples. Posttreatment quit rates ranged from 35 percent to 56 percent. Two studies replicating one another's methods reported six-month overall quit rates of 12 percent (
13), compared with 16.7 percent for patients taking atypical antipsychotics and 7.4 percent for patients taking conventional antipsychotics (
11). The use of clozapine seems to reduce smoking.
The studies of persons with depression involved larger, media-recruited samples of smokers and may represent a wider range of morbidity than the schizophrenia group. Quit rates in these studies ranged from 31 percent to 72 percent at the end of treatment and from 11.8 percent to 46 percent at 12 months. The integration of cognitive-behavioral therapy with standard smoking cessation strategies appears to result in higher quit rates for persons with a history of major depression. In one study the efficacy of bupropion for smoking cessation was found to be independent of any history of depression or alcoholism (
24).
The studies of persons with addictive disorders included both clinical and community samples. Quit rates ranged from 7 percent to 60 percent after treatment and from 13 percent to 27 percent at 12 months. When staff members quit smoking, it may provide positive role modeling for patients and increase staff willingness to provide smoking cessation support and intervention (
29).
Discussion and conclusions
Studies of different approaches to smoking cessation for persons with mental illness or addictive disorders are not sufficiently uniform to allow meta-analysis. Diagnoses encompass a broad range of dysfunction, particularly in the samples of persons with depression and addictions, and the degree of dysfunction affects outcome. The studies also do not use a standard time interval between intervention and outcome assessment. In addition, using measures of the use of or abstinence from a substance without using measures of other domains of functioning may oversimplify outcome assessment.
Generally, although quit rates of psychiatric populations may be lower than those of nonpsychiatric populations, the reasons for quitting smoking, such as health concerns and costs, are comparable (
31,
32). Poorer outcomes for smoking cessation strategies among psychiatric patients may have been expected because of the suspected use of nicotine for self-medication in this population. Nevertheless, posttreatment and 12-month quit rates for psychiatric patients appear to be only marginally lower than those for nonpsychiatric samples (
33).
These findings suggest that conventional attitudes about persons with mental illness being unable to quit smoking need to be modified. More resources should be devoted to cessation efforts for these populations, and clinicians should be more direct in asking patients about their interest in quitting smoking. Relatively brief interventions can increase the number of quitters, although smoking cessation tends to be a lengthier process for persons with mental illness. Staff training is a cost-effective investment.