In outpatient psychiatric clinics, missed appointments can compromise quality of care and reduce the efficiency of resource allocation. Initial appointments are more frequently missed, are less often rescheduled, and require more staff time than appointments for ongoing treatment (
1). Studies to identify patients at risk of missing initial appointments in a variety of outpatient psychiatric treatment settings have yielded inconsistent results (
1). Younger age (
2,
3), low socioeconomic status (
4), and longer waiting periods from contact to appointment (
3,
4) are the factors most consistently associated with nonattendance. Knowledge of the characteristics of those who attend and those who do not in a particular setting allows the prospective identification of patients at risk and can lead to program modifications to reduce the risk and rate of nonattendence.
Methods
The sample population included 313 patients with scheduled appointments at a Southwestern medical-school-affiliated psychiatric outpatient clinic from April through August 2000. Study subjects were referred by the Texas Department of Mental Health and Mental Retardation, a public-sector state agency that provides mental health services to persons with serious mental illness who meet specific diagnostic and financial criteria. Patients were given a specific date and time for an appointment at this clinic, which was within their catchment area and thus accessible to them. Data were obtained from medical records, including clinicians' ratings on the Brief Psychiatric Rating Scale (BPRS) (
5), agency assessment using the Multnomah Community Ability Scale (MCAS) (
6), and a structured interview assessment of sociodemographic information.
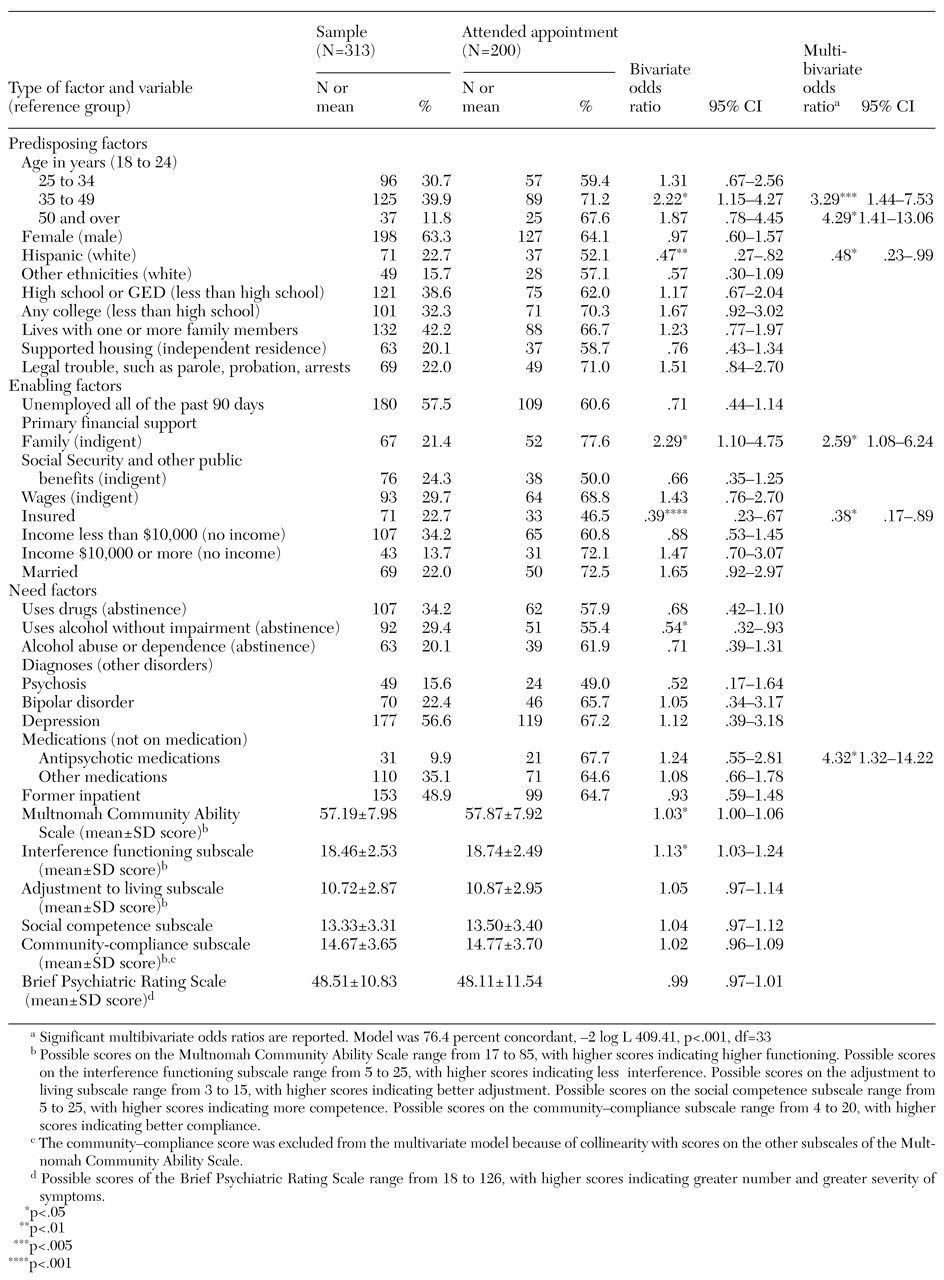
The explanatory variables in this study can be categorized as predisposing, enabling, and need factors in accordance with the behavioral model of health services utilization of Andersen and Newman (
7). Predisposing variables include age, sex, ethnicity, living situation, education, and legal trouble. Enabling variables include marital status, employment status, sources of financial support, annual income, and insurance status. Need variables included alcohol use, drug use, diagnoses, medications, inpatient history, BPRS score, and MCAS score. Tolerance statistics and Pearson correlation coefficients were used to examine correlations between predictor variables.
Logistic regression was used to identify factors associated with appointment attendance. Bivariate models of each explanatory variable assessed how useful the variable was at predicting whether patients would attend their appointments. A multivariate logistic model was used to determine which variables were independently associated with attendance after the other measured characteristics were controlled for.
Discussion
Although the "no-show" rate of 36 percent for this public-sector outpatient clinic was well within the range of the 26 to 50 percent previously reported for initial appointments (
4), this rate is nevertheless cause for concern. Patients who do not attend their appointments are at risk of being rehospitalized or of endangering themselves and others (
8).
At least one study found that most patients who miss psychiatric appointments reschedule within two weeks of the original appointment (
1). The problems of patients who do not spontaneously reschedule may resolve without professional care (
1,
9). However, this is unlikely to be the case among patients with severe mental illness, who constituted the patient population treated in the study clinic.
Our finding that patients aged 35 and older are more likely to attend their outpatient appointment than those under 25 is consistent with previous research (
2,
3,
4). The relationship between higher age and attendance may be related to previous psychiatric treatment, which is associated with attendance (
2).
The relationship between ethnicity and not attending the initial appointment is consistent with previous studies that reported less use of mental health services by Hispanics. Cultural barriers are often cited as the reason for less use by Hispanics when financial access is controlled for (
10).
The finding that the receipt of family support is related to appointment attendance suggests that such support may help to overcome financial barriers or that family members who provide financial support may also encourage the patient to obtain psychiatric care. Family support has been proposed as one mechanism that enables patients to seek care (
2).
The relationship between insurance and a lower likelihood of attending the initial appointment is interesting and suggests several policy issues connected with the relationship between access to care and funding. The findings of this study suggest that individuals who have health insurance, including Medicaid, have alternative treatment options and may use them if they offer advantages to treatment in a public-sector agency. While quality of care may not be adversely affected under these circumstances, they may contribute to inefficient use of staff and agency resources.
A major limitation of this study is that we had incomplete information about previous involvement with the psychiatric care system and about whether patients were referred from inpatient or community settings—factors that are known to affect appointment attendance (
2). Unfortunately, neither the date of hospital discharge nor the initial date of referral were consistently documented in the data available for review. This inconsistency also precluded the calculation of another important variable, the time between initial referral and the date of the scheduled appointment.
The important role we observed for antipsychotic medications is consistent with findings of studies that have identified a relationship between previous psychiatric treatment and appointment attendance (
2). Patients who take medications may be more motivated to attend their scheduled appointments, particularly if the benefit of medications is evident to them or their caregivers.