There is compelling pharmacoepidemiological evidence to document the increasing prevalence of psychotropic drug use among children, even those of preschool age (
4). Moreover, the use of combined psychotropic drug treatment is on the rise. In a study of community mental health centers in Baltimore County, an increase in the use of multiple concurrent psychotropics was described for the period between 1988 and 1994: from 9 percent to 21 percent among outpatients taking medications and from 26 percent to 42 percent among inpatients (
5). A recent study stated that 30 percent of children with ADHD co-occurring with another disorder received concurrent medications, compared with 10 percent of those with ADHD alone (
6). A North Carolina Medicaid managed care study found that of 6,984 youths for whom a selective serotonin reuptake inhibitor (SSRI) was prescribed in 1998, 30.1 percent also received a stimulant during the same year (
7). In a small case series, 50 of 83 children (60 percent) living in a residential treatment center received combination treatments (
8).
At the same time, combined psychopharmacotherapy can be an unjustified practice, as when duplicative agents (two or more agents in the same class) or offsetting agents (two or more medications with opposing actions) are initiated (
10). Failure to prune ineffective medications during ongoing treatment is one of the common pathways from rational to irrational polypharmacy (
11). Drug interactions are another important consideration during combined treatment. Problems can arise either from pharmacokinetic factors—such as effects mediated by the cytochrome P-450 system (
12)—or from poorly understood pharmacodynamic mechanisms that may have additional developmentally sensitive implications—such as the purported toxicity associated with stimulant and alpha
2 agonist combinations (
13).
One of the primary aims of pharmacoepidemiology is to examine trends in clinical practice. Despite growing empirical support for psychopharmacological interventions for children with certain psychiatric disorders, a gap between research and practice remains, and clinicians are often constrained to making choices with incomplete evidence-based guidance. Indeed, randomized clinical trials are unlikely to investigate more than a small fraction of potential combination treatments. Moreover, the algorithms or consensus guidelines that have been published (
15), although they provide some support for combination treatments, are neither an accurate reflection of current clinical practices nor a substitute for the level of empirical support provided by randomized clinical trials. A claims-based study describing community practice patterns can be an informative initial step toward understanding current combination psychotropic interventions and can guide future research efforts on this type of treatment.
The objective of this study was to determine the prevalence, patterns, and demographic correlates of psychotropic drug use in general, as well as of multiple psychotropic pharmacotherapy in particular, in a statewide sample of low-income children and adolescents receiving community-based clinical care.
Discussion and conclusions
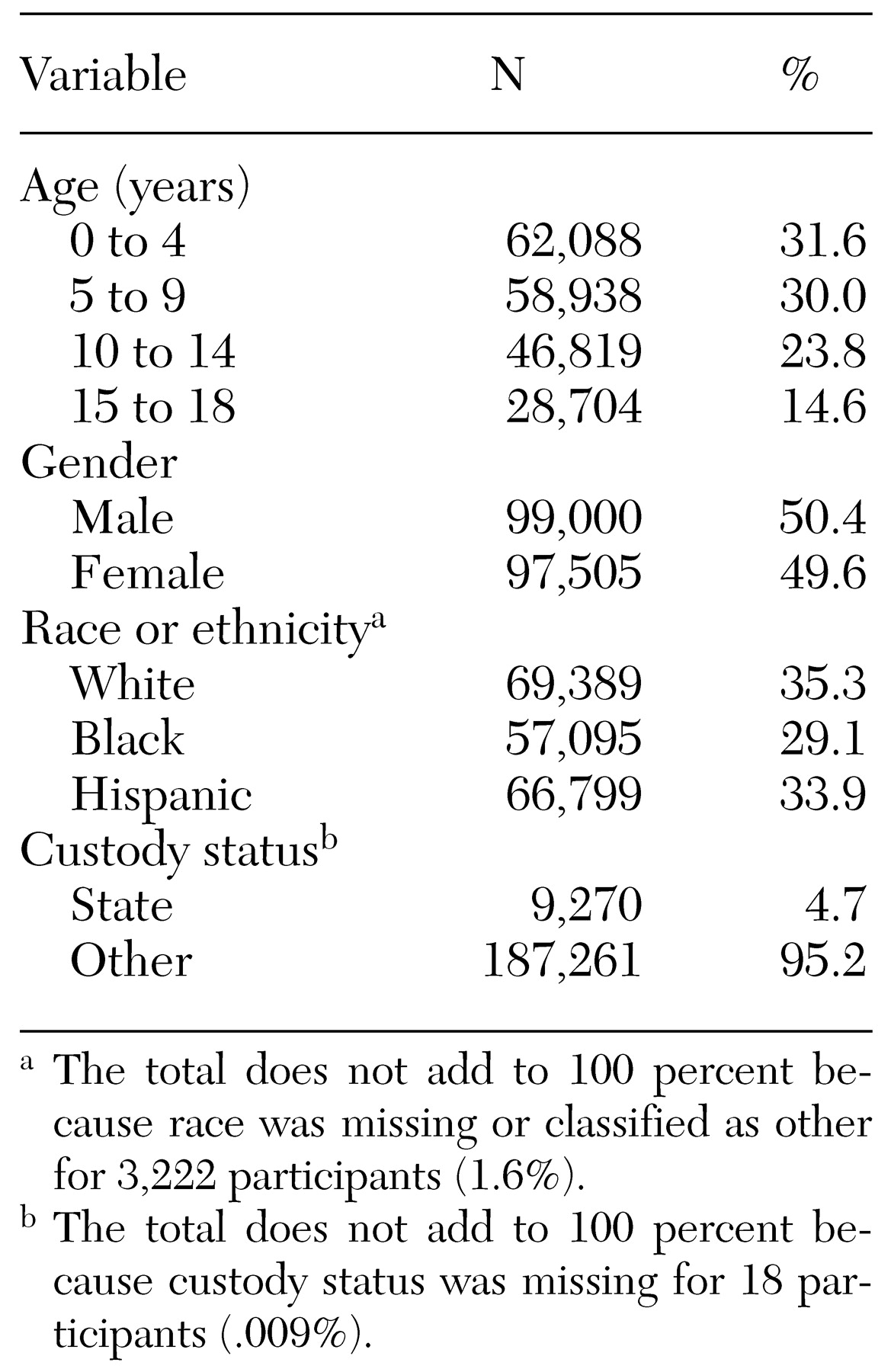
This study documented a 4.8 percent period prevalence of psychotropic drug use among children enrolled in Connecticut Medicaid managed care. This rate is virtually identical to that reported in 1995 for children enrolled in Kansas Medicaid, the most recent study for which comparable data are available (
18). Consistent with earlier reports, our findings reveal differences in age, gender, and ethnicity among youths who received psychotropic medications. Age differences are of a particularly timely relevance, because psychotropic medication rates among preschool children have recently attracted widespread attention in both the scientific and the lay press. Findings from our study corroborate the frequent use of psychotropics in this age group. For example, among 35,274 children aged two to four years, stimulants were prescribed for 396, yielding an age-specific period prevalence of 11.2 per 1,000. This rate is in keeping with preschooler rates recently reported in two studies. In a study by Zito and colleagues (
4), the prevalence of stimulant use in 1995 ranged from 5.1 to 12.3 per 1,000, and in a study of 1998 North Carolina Medicaid data the prevalence was 13 per 1,000 for children ages 1 to 5 (
7). Even if not strictly comparable, all three studies point to a prevalence in the range of .5 to 1.3 percent in this very young age group—one for which the empirical database is especially limited.
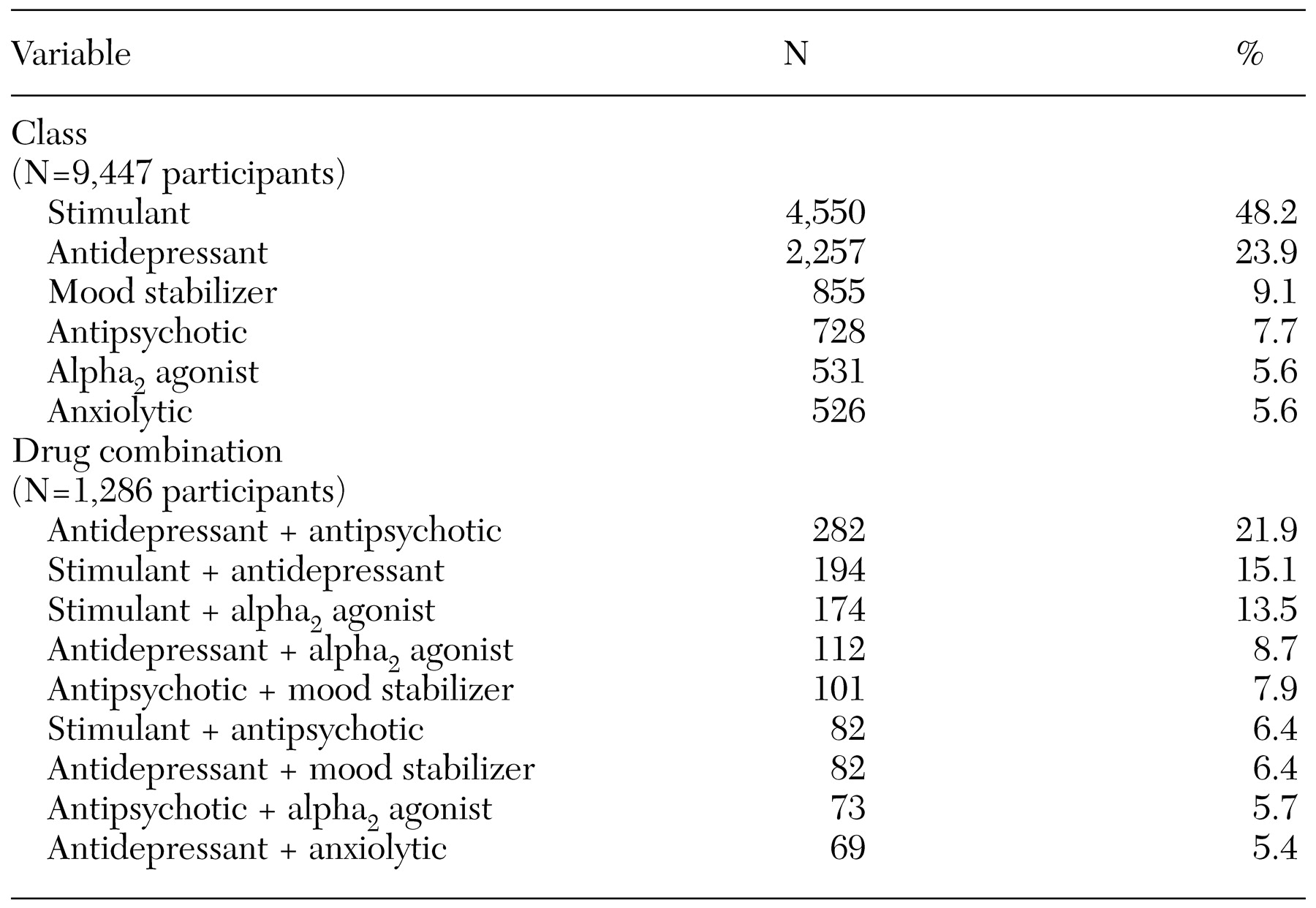
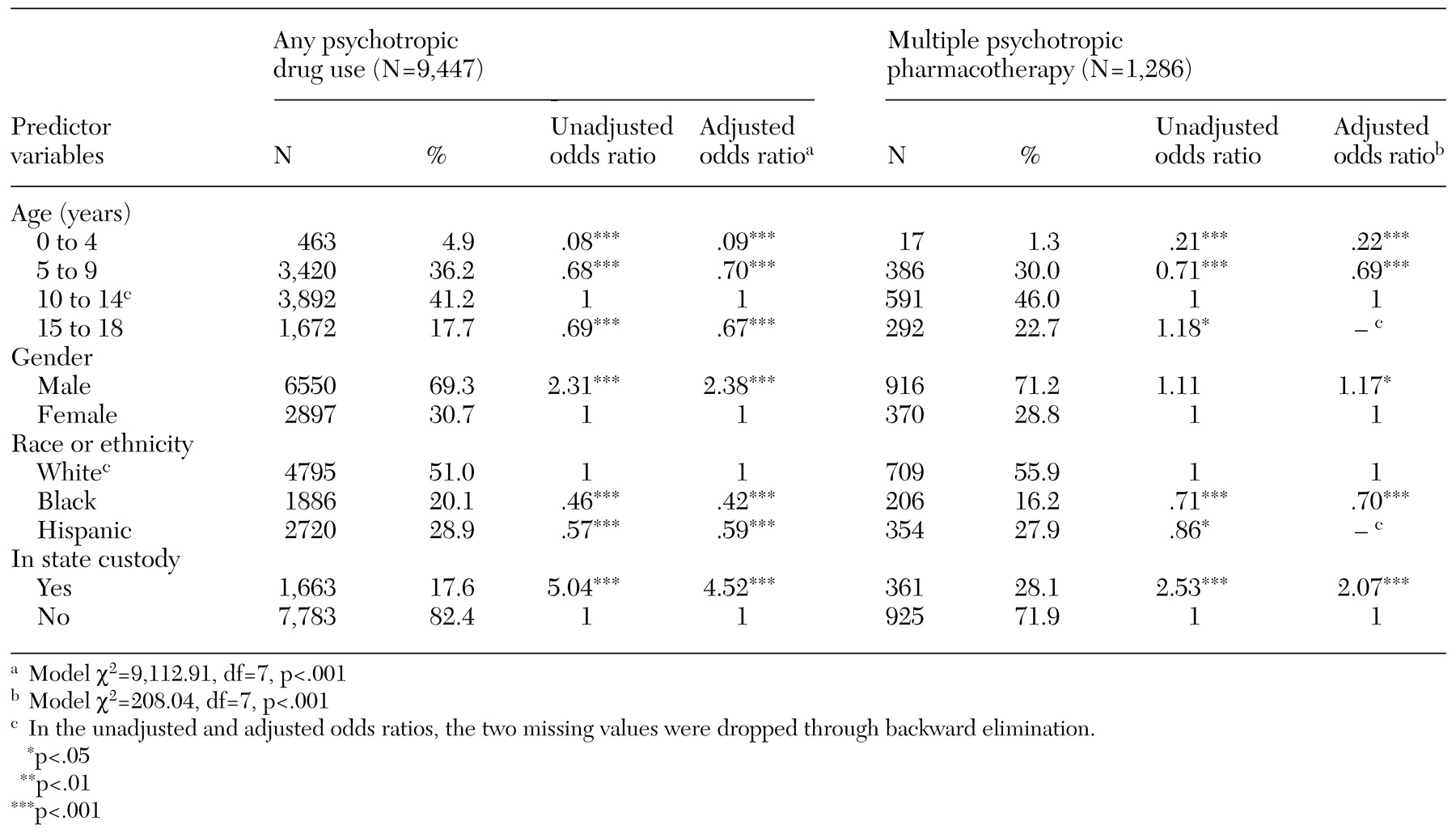
Overall, boys were 2.4 times as likely to receive psychotropics as were girls, and children aged ten to 14 years were at least 1.4 times as likely as those in any other age group. This distribution pattern, together with stimulants' being the most commonly prescribed psychotropic class (
Table 2), suggests that ADHD is the main condition targeted pharmacologically. Our diagnostic information, although limited, corroborates this impression: almost 60 percent of youths for whom data were available had a primary diagnosis of ADHD. Moreover, the second and third most common patterns of multiple psychotropic pharmacotherapy were stimulant plus antidepressant and stimulant plus alpha agonist—combinations suggested in a recently published algorithm for ADHD when stimulants alone are not effective (
15,
19).
Consistent with previous studies (
7,
20,
21), our data reveal that children from minority groups are less likely to have psychotropics prescribed for them. For example, when the analysis was adjusted for potential confounders, white youths were 2.4 times and 1.7 times as likely to have psychotropics prescribed as were their black or Hispanic peers, respectively. This consistently documented racial and ethnic disparity may reflect differences in access to care or different attitudes or cultural beliefs among various groups—about mental health in general or about the use of psychotropics in particular. In addition, racial and ethnic misclassification is a small possibility to consider in the analysis of large databases. Regardless of the underlying reason for these differences, additional study is clearly warranted to understand and address such disparities in psychotropic drug use.
Children in state custody represented only 4.7 percent of the Medicaid population yet accounted for 17.8 percent of the psychotropic prescriptions filled. This 4.5-fold higher rate emerged as the single strongest predictor of psychotropic drug use in our study. Given that children in state custody are a vulnerable group at high risk of serious psychopathology, this is not an entirely surprising finding. To our knowledge, rates of psychotropic drug use for children in state custody have not been previously studied. However, two studies of children in the Los Angeles County foster care system (representing a segment of children in state custody) have documented a threefold higher rate of psychotropic drug use than in the control group of youths in the community (
22,
23), and a third study has found similar patterns among foster care youths covered by a mid-Atlantic state Medicaid program (
24).
As defined here, multiple psychotropic pharmacotherapy is a common practice in pediatric pharmacotherapy; 13.6 percent of youths for whom psychotropics are prescribed receive more than one psychotropic. Given the cross-sectional nature of our study, it was not possible to determine with certainty whether agents were used concurrently (as an additive strategy) or sequentially (for example, as part of a cross-tapering switch). To minimize this potential misclassification, we restricted combination use to medications from different drug classes, because medications in the same class would be more suggestive of a switching pattern. Only a longitudinal approach can distinguish such underlying prescription patterns; however, our findings suggest that treatment with more than a single psychotropic agent during this conservatively defined time interval are common in this Medicaid population, possibly as part of a change to more stable medication regimens. In addition to revealing multiple psychotropic pharmacotherapy as a common treatment pattern, our study found significant sociodemographic factors associated with its occurrence. Children who were ten years of age and older, male, white, or in state custody were all more likely to receive multiple psychotropic pharmacotherapy. These characteristics also predict psychotropic drug use in general, although they warrant particular attention as predictors of multiple pharmacotherapy. In the one previous study that assessed predictors of polypharmacy among adults, neither age, sex, nor race was a significant factor (
10).
Our study has several limitations. First, claims-based data provide minimal clinical information, and that information is of uncertain quality; there is no readily available way of validating assigned diagnoses. Moreover, a primary diagnosis was missing for 42.9 percent of children treated with psychotropics during the study period. Although this is a substantial proportion of participants, it is not an uncommon one in comparable pharmacoepidemiology surveys. For example, a recent outpatient study found that no psychiatric diagnosis was made in more than 30 percent of visits involving a psychotropic medication (
25). The investigators suggested that such a deficiency might be related to either of two factors: primary care physicians' limited knowledge about, or comfort with, assigning psychiatric diagnoses; or clinicians' resorting to pharmacological intervention when addressing vague behavioral problems for which there is no clear diagnosis.
A second limitation is that our choice of a one-week interval to estimate multiple psychotropic pharmacotherapy is potentially problematic. In the absence of a standardized time interval for the assessment of polypharmacy, some investigators (
7,
26) have chosen a one-year window. However, such a choice, while increasing the sensitivity of our findings, would have done so at the expense of an unacceptable number of false positives—that is, cases of sequential rather than concurrent use of different medications. Indeed, when we used a three-month window, our estimate of multiple psychotropic pharmacotherapy more than tripled, to 42 percent. Our ultimate choice for the briefer window of time is consistent with the published experience of another group (
17) and protects from overestimation of multiple psychotropic pharmacotherapy (false positives). Clearly, the best way to estimate the prevalence and specific patterns of multiple psychotropic pharmacotherapy, and to differentiate concurrent from stepwise or sequential drug use, would be to track participants longitudinally. Other informative next steps toward this end might be targeted chart reviews and surveys of the decision-making processes of community practitioners. Despite the uncertainty of our one-week window, our study does provide initial insights into an increasingly common practice within the field of pediatric psychopharmacology.
A third limitation is that the Connecticut Medicaid managed care database did not include information on prescribers' professional affiliation, such as physicians, physician assistants, or clinical nurse specialists, or their specialty training, such as primary care medicine, pediatrics, or psychiatry. Previous studies have documented that in the treatment of ADHD, for example, the majority of psychotropic medications are prescribed not by mental health specialists but rather by general practitioners (
27,
28). Another consideration is that the more complicated or treatment-refractory cases may in turn be referred to specialists, who may follow different prescription patterns, including combination treatments (
29). In a previous study of adults, physician specialty (psychiatry versus nonpsychiatry) was found to be the single strongest positive predictor of polypharmacy (
10). Two subsequent studies have also found physician specialty to be significantly related to psychotropic combination prescription patterns for youths (
26,
30). Such findings have direct training and administrative implications, supporting the need for more extensive training in psychopharmacology for pediatricians and other primary care practitioners, the procurement of appropriate staffing, and the facilitation of more efficient referral pathways to specialists.
Despite its limitations, our study documented rates and patterns of psychotropic drug use among young Connecticut Medicaid managed care enrollees that are comparable to rates in other parts of the country. In particular, our study replicated findings of both clear differences among racial groups in this modality of treatment and the use of psychotropic drugs among as many as 1 percent of preschoolers. Moreover, our study showed that a considerable proportion of children receiving psychotropics have been treated with two or more such agents within a one-week period. Future claims-based research in pediatric psychopharmacology will permit the study of changes over time in this modality of treatment, as well as the characterization of the extent and patterns of multiple psychotropic pharmacotherapy in community-based clinical settings.