The prevalence of co-occurring mental health and substance use disorders among adolescents has risen to a level comparable to that among adults and is an important public health concern (
1). Treatment for adolescents with co-occurring disorders is typically delivered in two separate service systems. Coordination of services is hampered by differences in treatment philosophies, clinical approaches, training, and eligibility requirements.
Funding mechanisms and administrative policies have historically defined the mental health and substance abuse treatment systems (
2). Obstacles to service use are characterized, in part, by the behavior of patients and their families that shape how symptoms are defined and by what they view as appropriate pathways into care and relevant services. Other obstacles reflect the training, orientations, and judgments of service providers and the financial and organizational incentives that affect their decisions (
3). These obstacles may be particularly relevant for rural adolescents, whose access to health services is further hampered by several factors, including fear of stigma, lack of insurance, and a paucity of health care facilities and personnel (
4).
There are several treatment models for adults with co-occurring disorders. Research has shown the effectiveness of coordinated and integrated treatments in improving symptoms, functioning, and treatment participation of adults (
5). The coordination and integration of mental health and substance abuse treatment has received substantial support from clinicians and national organizations (
5,
6). Despite recommendations that adults with co-occurring disorders receive treatment for both their mental and their substance use problems, most do not (
7).
There is a gap between what researchers have shown to be effective for adults with co-occurring disorders and what is practiced in clinical settings that serve youths. Although effective treatments for adolescents with mental health or substance use disorders have been developed and incorporated into programs of care, information on the availability and use of collaborative care by adolescents in rural delivery systems is scarce. This column presents the findings of a study of the treatment needs and service use of rural adolescents with mental and substance use disorders who were served in community-based settings.
Methods
A total of 177 adolescents aged 12 to 18 years who lived in a three-county region in southeast Iowa and who were discharged from 17 community-based mental health or substance abuse treatment programs during the one-year period from January 2001 to January 2002 were included. The study received institutional review board approval.
Diagnosis and demographic and background information were obtained from medical records. To assess the type and severity of clinical and psychosocial problems at admission and discharge, the Child and Adolescent Needs and Strengths (CANS) tool (
8) was completed retrospectively with use of medical records. The level of unmet treatment need, factors that predict service use, and the degree of improvement were summarized. Unmet need was defined as the presence of an unaddressed need during treatment or at discharge from the program. It was measured by the presence of a diagnosis or by a CANS score of 2 or 3 on items measured under problem presentation and by the absence of any use of services directed toward that need during treatment and the absence of arrangements to address that need at the time of discharge. Service use was assessed by reviewing service notes to determine whether a service was provided by a mental health or addictions specialist and whether the service was directed toward an emotional, behavioral, or substance use problem.
Results
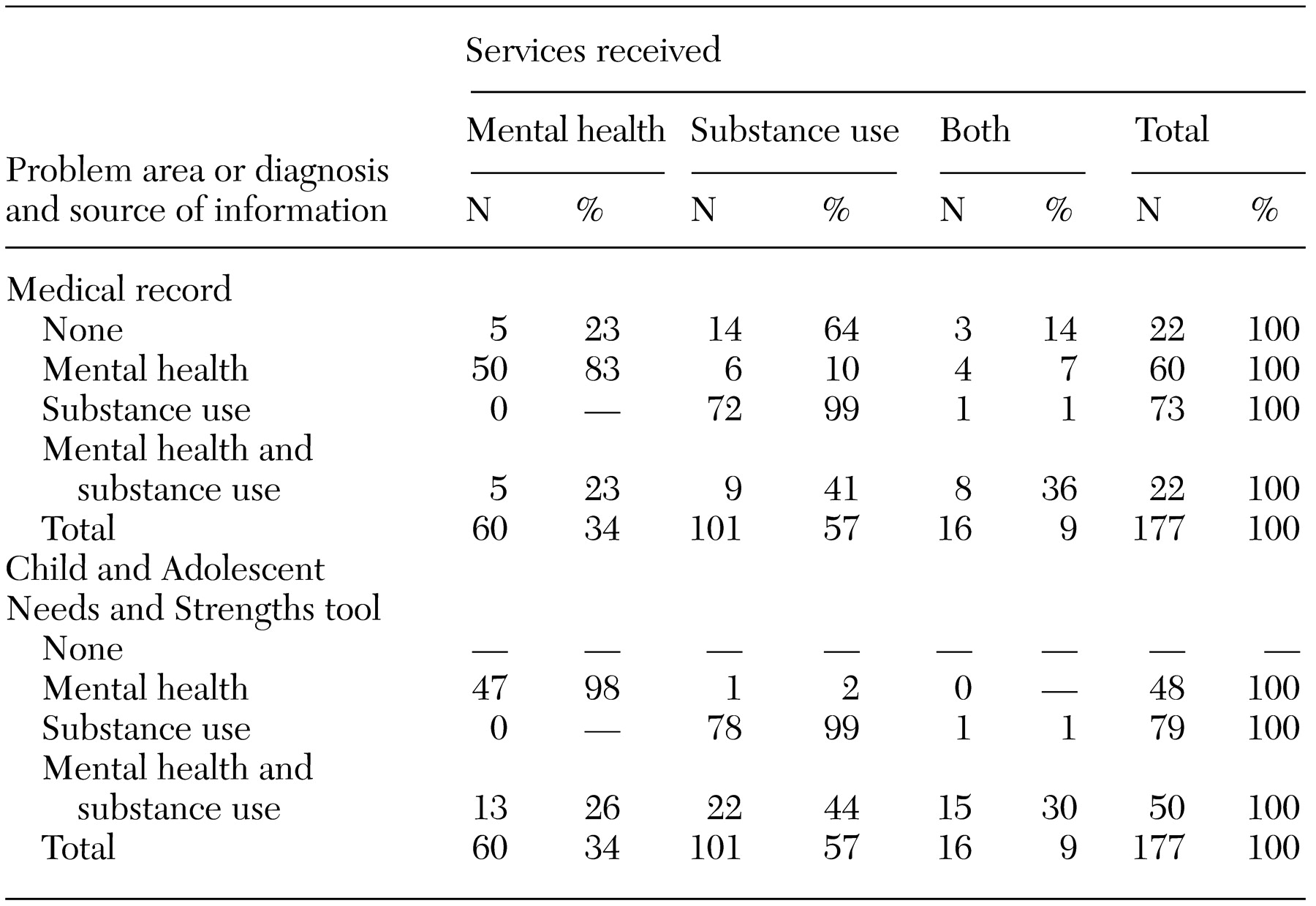
The average age of the 177 adolescents was 15.5 years. Sixty (34 percent) were girls, and 165 (93 percent) were white. Eighty-six (49 percent) were Medicaid eligible. Most (124 adolescents, or 70 percent) received treatment outside of the county in which they lived. The diagnoses of the 177 adolescents are listed in
Table 1 along with the treatments they received.
Of the 60 adolescents with a diagnosis of a mental health disorder only, six (10 percent) received no mental health treatment. Of the 22 adolescents with co-occurring disorders, only eight (36 percent) received both mental health and substance use treatment. When using the CANS as a measure of treatment need, only 15 (30 percent) of the adolescents with co-occurring disorders received dual services. In other words, about two-thirds of adolescents with co-occurring disorders or problems did not receive treatment consistent with widely supported guidelines recommending that they receive treatment for both their mental health and substance use problems (
5,
6).
Adolescents with co-occurring disorders who had more severe depression and less severe antisocial behavior and who had stronger social supports, previous mental health treatment, and no history of sexual or physical abuse were significantly more likely to receive dual treatment.
Adolescents with co-occurring disorders who received a single treatment improved according to most clinical and psychosocial measures at discharge. Interestingly, this group did not differ significantly in degree of improvement from the group that received dual treatment.
Discussion
Despite a growing body of evidence supporting coordinated treatment of mental health and substance use problems, it appears that when these problems co-occur among adolescents, treatment needs of this group continue to be unmet. This study found that about two-thirds of adolescents with co-occurring disorders did not receive the dual treatment that is recommended in widely supported guidelines. It must be noted that simply the presence of a diagnosis may not constitute sufficient reason for providing care. Similarly, the absence of a diagnosis may not constitute sufficient reason for not receiving care. Reliance on diagnostic criteria to determine the type and level of mental health services needed has generated little success, particularly for adolescents.
For adolescents, complex problems reflect interactions between biological vulnerabilities, developmental factors, and environmental circumstances, and categorical diagnoses in the
DSM-IV are less defined and clear (
9). However, the severity of presenting problems along with an assessment of functioning and risk behaviors has been a key indicator for treatment decisions (
10). By using the CANS to assess the presence, type, and severity of problems, a wider net was cast to include youths who presented with no formal diagnosis but some level of treatment need associated with co-occurring problems. Use of the CANS resulted in a slight increase in level of unmet need compared with use of chart diagnoses (70 percent compared with 64 percent).
The findings related to physical and sexual abuse are notable because evidence suggests that such abuse is associated with an increased likelihood of substance abuse and emotional or behavioral disturbance (
11). The relationship of a history of physical or sexual abuse and unmet need for mental health and substance abuse treatment not only highlights the importance of improved collaboration between mental health and substance abuse programs but also underscores the need for collaboration between the public health and mental health sectors to develop public education, community-based prevention, and outreach interventions targeting adolescents and their families.
Iowa remains one of 21 states that have separate administration of the mental health and substance use treatment systems. Without a unified state blueprint for developing programs and action plans, it is difficult to organize current resources toward any long-term cohesive goal and to plan for future service needs.
For adolescents with co-occurring disorders, the degree of improvement was about the same whether they received single or dual treatment. There are several possible explanations for the lack of difference between these groups. The groups were small, and their comorbid disorders differed—those who received dual treatment were more likely to have depression and those who received single treatment were more likely to exhibit antisocial behavior. Thus the extent to which appropriate care was provided for the comorbid disorders might account for the differences in treatments provided to the two groups. It is also likely that some adolescents who received a single treatment eventually received treatment for the other co-occurring disorder—a serial model of service delivery. A serial model is inconsistent with widely supported guidelines recommending collaborative and integrated treatment approaches.
Adolescents with co-occurring problems who received only mental health treatment had significantly improved mental health outcomes but showed no improvement in their substance use problems. Similarly, those who received only substance use treatment showed improvement in substance use outcomes but not in mental health measures. This finding is consistent with documented evidence of poor outcomes for adults with co-occurring disorders when programs fail to coordinate treatment needs (
12).
Conclusions
Minkoff (
13) has stated that the provision of services has been organized along a single-disorder model because clinicians believe that co-occurring disorders are an exception. However, Minkoff and others (
14) have documented that co-occurring disorders are the rule rather than the exception. Promising data on the positive effects of coordinated and integrated care among adults suggest that an increased commitment from policy makers, administrators, providers, funding agencies, and researchers is needed to provide an understanding of the benefits of collaborative management of adolescents with co-occurring disorders so that scarce rural resources can be more effectively allocated to increase the capabilities of the system.
Clear advances have been made in mental health and substance abuse treatment. Factors related to families, programs, systems, and policies that act as barriers to unifying philosophies and practices need further study so that adolescents with co-occurring disorders will receive appropriate care.