The guide describes a structured format for managing acute aggressive episodes and provides staff with a model for implementing the recommendations. It is assumed that interpersonal and behavior management techniques are considered before higher-level interventions are implemented.
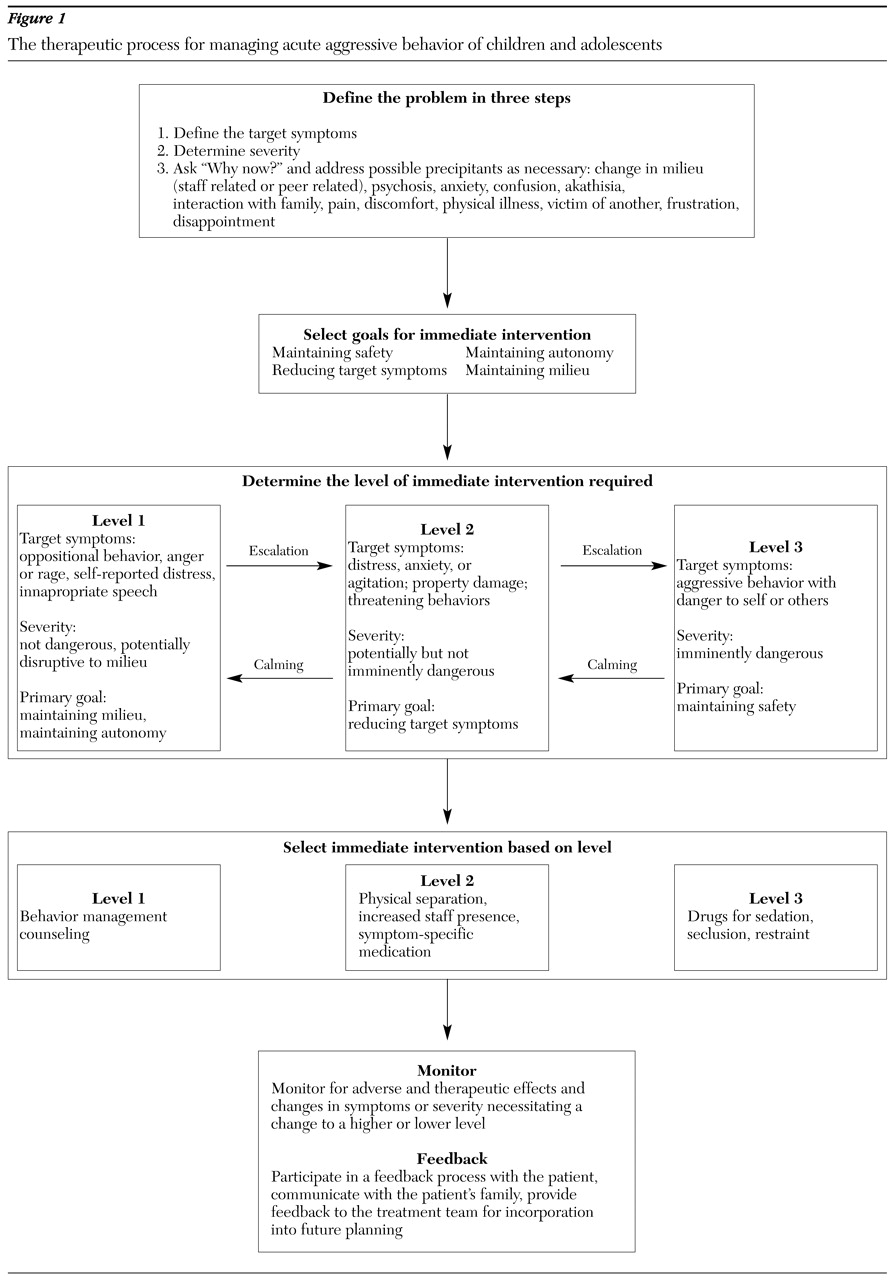
Conceptual model for the therapeutic process
The guide is based on a therapeutic process used in other areas of medicine (
6,
7). Although this process may appear time-consuming, it is likely to produce timely assessment and implementation by highlighting important concepts and reinforcing a systematic and comprehensive decision-making paradigm. Acknowledging that staff members already incorporate into their work most of the basic principles contained in the recommendations, this model aims to promote greater proficiency through reinforcement.
Define the problem. The first step in the therapeutic process is to define the problem. Although the initial assessment occurs instantaneously, staff should consider three key issues in defining the problem: the target symptoms, the severity of symptoms, and precipitating factors. The target symptoms—for example, pacing, increased attention seeking, and hitting—are the reason for acting. The severity of the target symptoms dictates the level of intervention—for example, nondirected verbal aggression versus physical aggression toward others. Finally, by identifying a precipitant for the behavior, the "cause" rather than just the symptom may be addressed, which has the potential to prevent future episodes. This cause may range from an exacerbation of an underlying disorder to a reaction toward a social situation, such as the fact that a parent does not visit, or disturbance in the milieu, such as teasing by another patient. The committee recognizes that the precipitating factors may not always be evident during the initial assessment.
Select goals for the intervention. Although the most salient goal during an acute aggressive episode is resolution of the behavior, other goals also warrant consideration. Such goals include maintaining the safety of the patients and staff, maintaining patient autonomy, reducing the target symptoms, and maintaining a therapeutic milieu. Occasionally patients and staff are in immediate danger, and safety surpasses maintaining autonomy and reducing the target symptoms. Nonetheless, the other goals should be considered as soon as the situation allows.
Determine the level of intervention required. Severity often dictates the level of intervention required. The higher (more restrictive) intervention level is used when there is potential or imminent danger. This level of intervention requires more resources and carries a greater degree of risk to health, safety, and autonomy. Sometimes multiple interventions within a level are needed, and unresolved or worsening situations may require higher-level interventions. When a situation begins to resolve, a lower-level (less restrictive) intervention may be used. Overall, staff should identify the level of intervention that will return the youth to the normal routine of the milieu as quickly and as safely as possible.
The intervention levels are as follows. Level 1 encompasses behavioral management techniques that instill trust and hope, such as listening to the youth. Level 2 involves interpersonal responses and orally administered antihistamines, benzodiazepines, and antipsychotics. Within this level, antipsychotics should be used only to reduce psychosis and disorganization and should be dosed accordingly. Level 3 interventions, which are considered a last resort, include seclusion, restraint, orally administered antipsychotics at dosages that will produce immediate sedation, and all intramuscular medications.
Select the intervention. Interventions should be based on patient characteristics and intervention-specific properties to promote individualized care. Patient-related considerations include medication allergies, current medications, diagnostic profile, conditions affecting dosage or route of administration (for example, oral or intramuscular), previous response to interventions, history of physical or sexual abuse, learning pattern, and intellectual capacity. Body weight should be considered in implementing restraints and dosing medications. Intervention-related considerations include side effects, time to onset, duration of effect, dosage form, and monitoring parameters. Patients who present imminent danger to themselves or others require interventions with a rapid onset of action, such as intramuscular medications, fast-acting benzodiazepines, and seclusion or restraint.
Monitoring and feedback. The final steps—monitoring and feedback—are intended to evaluate the effectiveness of the interventions. Discussions between the clinician and the youth should strengthen the therapeutic alliance and lead to a better understanding of each individual's perspective. Interventions that work best for the youth should be documented and shared with the treatment team.
Monitoring includes an evaluation of the positive and negative aspects of an intervention, including side effects, worsening of the target symptoms, and the effects on patient autonomy and on the integrity of the milieu. Most facilities already have established monitoring parameters, particularly for level 2 and 3 interventions. Clinical judgment determines when the goals of the intervention have been achieved. If the goals are not achieved, alteration or cessation of the intervention or selection of another intervention within the same or a different level may be warranted.
Feedback ideally should occur among members of the treatment team as well as with the patient and the patient's family or guardian. Discussions among members of the treatment team serve several functions. First, all individuals involved in the care of the youth become aware of the aggressive episode. Second, the team can determine whether changes in the treatment plan are needed, particularly when acute aggressive episodes occur frequently. Finally, staff become aware of the effectiveness of various interventions.
Communication with the patient and the patient's family or guardian also has important implications for the youth's treatment. This interaction may disclose new information about psychosocial issues that could have precipitated the aggressive episode or series of episodes and may lead to treatments that could prevent subsequent events. Feedback with the family or guardian fosters a more productive alliance with the treatment team and affords the opportunity for parent education.
Specific recommendations for the feedback process are provided for the most restrictive level 2 and 3 interventions. The recommendations are consistent with the recommendation of the CMS (42 CFR Parts 441 and 483) and JCAHO that were in place at the time that the guide was prepared. CMS requires a face-to-face assessment of the youth's physical and psychological status within one hour of seclusion or restraint, an assessment by a physician or a registered nurse immediately after the intervention, and communication with the youth's parents or guardian as soon as possible. Postintervention debriefing between the youth and the staff members who were involved in the incident should occur within 24 hours of the seclusion or restraint. JCAHO regulations are consistent with regard to notification of the youth's parents or guardian and the monitoring and evaluation during and after the use of seclusion or restraint.
Descriptions of the interventions
Level 1. The primary objective of a level 1 intervention is to maintain the milieu and maintain autonomy. Early interventions should prevent further escalation of the situation and therefore should be initiated as soon as mild agitation is detected. Ideally, level 1 interventions focus on the patient, the milieu, or both and are based on an understanding of the youth's typical behavior, developmental stage, and past experiences with behavioral management techniques.
Although a discussion of all potential behavioral management techniques is beyond the scope of the guide, a few examples are provided. Readers should refer to currently available programs and manuals for more detailed information. One example is communication. Listening and conveying interest in and concern about the patient's welfare are critically important. Second, engaging the patient in a conversation about his or her experiences and feelings may calm or rectify the disturbing situation. Third, offering choices gives a patient a sense of control over the situation and may include interaction with a trusted staff member; physical activity, such as walking or exercising; listening to music; meditation; and diversional activities such as woodworking and gardening.
Body language cues are another example. It is important to approach an agitated person in a nonthreatening manner and to be sensitive to a patient's need for adequate personal space. In addition, it is helpful to offer the patient a quiet place within the milieu, either to be alone or to interact with staff. Removing other patients and other stimuli from the immediate vicinity helps the agitated or aggressive patient regain control by decreasing stimulation and eliminating the urge to perform for one's peers. Finally, maintaining a therapeutic milieu that keeps patients engaged or occupied and conveys a sense of staff control reduces the potential for aggressive behavior.
Level 2. The primary goal of a level 2 intervention is to reduce the target symptoms. However, to the greatest extent possible, it is also important to maintain the patient's autonomy and maintain the milieu. Level 2 interventions should be considered when a level 1 intervention is not appropriate or has not been successful.
Level 2 interventions focus on interpersonal responses and medications to ameliorate specific symptoms and assist the individual in achieving behavioral control. All level 2 interventions require voluntary cooperation from the youth, and the youth maintains the capacity to communicate with staff and to negotiate his or her preferences for particular interventions. Alternatives are not presented in a coercive or punitive manner, but rather should encourage the youth to exercise autonomy. The classes of medications included within this level are based on a review of the literature about management of acute aggressive behavior among youths. Medication as a level 2 intervention is aimed at reducing the target symptoms and calming the patient. The sedative effects of these medications can impair cognition, resulting in some loss of autonomy, and should be taken into account before these medications are used.
For example, facilitating physical separation by directing the patient from an overstimulating environment to a quiet, less stimulating area helps to deescalate an agitated youth. This intervention may include the use of a quiet room or other unoccupied space. Once the youth has been removed from the stimulating environment, staff may use level 1 interventions to manage the situation.
Increasing the number of staff present during an acute aggressive episode is often sufficient to help a youth regain self-control. This approach also helps secure the safety of other persons. However, its feasibility is highly dependent on the resources available in the facility.
Level 2 medication interventions include antihistamines, benzodiazepines, and antipsychotics. Despite the lack of scientific evidence to support the use of antihistamines for the management of acute aggression, these medications have some beneficial therapeutic aspects. First, antihistamine medications have a relatively safe profile. Second, parents or guardians are likely to be more familiar with these medications than with psychopharmacologic agents. Third, patients often request antihistamines when they become agitated. Fourth, the sedative properties of antihistaminic agents have been used successfully to manage acute aggressive episodes.
Although little scientific evidence exists to support the use of benzodiazepines for the management of acute aggressive episodes, these agents may be particularly useful when anxiety is contributing to agitation or when some degree of sedation is warranted. One caveat is the paradoxical agitation that can occur with benzodiazepines, which should be considered carefully before a benzodiazepine is used.
A low dose of an oral antipsychotic that possesses more sedating properties is often used for its calming effects.
Level 3. The primary goal of a level 3 intervention is to maintain the safety of the patient, other youths, and staff. Level 3 interventions are the most restrictive and are used as a last resort when a level 2 intervention either is not appropriate or is unsuccessful. These interventions should be as short in duration as possible. At this level the youth may be irrational and unable to negotiate his or her preferences.
Level 3 interventions include seclusion, restraint, and intramuscular formulations of antihistamines, benzodiazepines, or antipsychotic agents and orally administered antipsychotics used primarily for sedation. Level 3 interventions should be implemented only by adequately trained staff who routinely undergo competency evaluations. After a review of the literature and several discussions, it was the committee's view that there is insufficient evidence at this time to rank the level 3 interventions on the basis of restrictiveness, tolerability, or safety. Thus one level 3 intervention is not preferred over another. Staff members are encouraged to use the therapeutic process to choose the most appropriate intervention.
The committee strongly emphasizes minimal use of seclusion, restraint, and intramuscular medications, all of which should be used only when the primary concern is the safety of all individuals in the milieu. Level 3 interventions are not to be incorporated into the youth's treatment plan, because they are not used to achieve treatment goals. Use of seclusion and restraint is analogous to cardiopulmonary resuscitation (CPR) in a crisis situation. Like seclusion and restraint, CPR is implemented in a precise manner, is used for safety reasons, aims to return an individual to baseline functioning, and does not treat an underlying condition or illness.
Past experiences and individual preferences for level 3 interventions should be noted in the youth's chart so that staff will be aware of these factors. The use of less restrictive level 1 interventions as a means of preventing escalation to level 3 also should be noted. Federal and state guidelines for the use of seclusion, restraint, and medications should be followed, and caution should be taken to reduce the risk of harming the youth, the staff, and other persons.
Looking at seclusion as an example of a level 3 intervention, this intervention has the positive aspect of minimal loss of functioning. The patient maintains control over mobility, thinking, and autonomy. Seclusion may be particularly useful for patients who are physically active but are not exhibiting self-injurious behavior. The negative impact of seclusion is the associated social isolation. Seclusion may be of greater benefit to youths who are overstimulated by social contact. Seclusion should be terminated as soon as possible, and when staff determines the patient can maintain self-control and refrain from unsafe behavior in the milieu.
In the case of restraint, there is a greater loss of autonomy and mobility than occurs with seclusion. Positive aspects of restraint include the fact that cognition is not altered and that there is less social isolation, because the youth has ongoing contact with staff. This approach may be particularly helpful for youths who fear abandonment. Restraint also may be preferred when the safety of the patient is in question. The use of restraint should be terminated as soon as the patient agrees to maintain self-control and refrain from unsafe behavior, and when the staff is assured that the youth is capable of such control.
In terms of medication interventions, intramuscular antihistamine, benzodiazepine, or antipsychotic formulations are more invasive than oral agents. In general, orally administered antipsychotic medications are reserved for patients whose acute aggressive episode is precipitated by an underlying psychotic process. In rare situations an intramuscular medication may be the most appropriate intervention—for example, if the youth cannot be maintained safely without antipsychotic medications or medications preserve autonomy more effectively than seclusion or restraint. Decreased autonomy, mobility, and cognition may be greater than with seclusion or restraint, because, once medication has been administered, staff cannot terminate the medication's effects, as can be done with seclusion or restraint.
Special considerations for level 2 and 3 interventions. One special consideration for level 2 and 3 interventions is the classification of chemical restraints. Federal regulations for specific situations in which pharmacologic interventions constitute a chemical restraint were carefully considered. According to the CMS regulations (CFR 483.352, effective March 23, 2001), which govern the use of seclusion and restraint in psychiatric residential facilities that provide psychiatric treatment to persons under the age of 21 years, medications are considered a restraint when all three of the following criteria are met: the medication is administered to manage a resident's behavior in a way that reduces the safety risk to the resident or others, the medication has the temporary effect of restricting the resident's freedom of movement, and the medication is not a standard treatment for the resident's medical or psychiatric condition.
Thus medications should not be considered a restraint when they are used to address psychiatric symptoms that are associated with the acutely aggressive episode. On the other hand, when medications are used solely to address the aggressive behavior or induce sedation and safety is the primary reason for use—that is, the medications are not being used for an underlying medical or psychiatric illness—this use is considered a restraint and is subject to the federal and state regulations.
Another consideration is "off-label" use of antipsychotic medications. Although oral atypical antipsychotics are widely used for the treatment of acute aggression, these medications do not have approval from the Food and Drug Administration (FDA) for such use among children and adolescents. The FDA does not have a formal opinion on the off-label use of antipsychotics (personal communication, Mosholder A, 2001). Given the lack of data for children and the potential for acute dystonic reactions and cardiac effects, the committee adopted a more conservative approach: use of oral antipsychotics at level 2 should be solely for the treatment of psychotic symptoms and disorganization. Modifications to the current recommendations await additional scientific evidence of their safety and efficacy.
In addition, it is important to consider intramuscular formulations of newer atypical antipsychotics. An FDA advisory board recommended approval of intramuscular olanzapine and ziprasidone in the treatment of acute agitation, although the available data cannot be extrapolated to include children (personal communication, Mosholder A, 2001). Revisions to these recommendations await adequate scientific evidence supporting the safety and efficacy of intramuscular formulations of olanzapine and ziprasidone for the management of acute agitation among children and adolescents.
It is also important to note that droperidol is not a pharmacologic alternative for a level 3 intervention. This agent has a more pronounced effect on the QTc interval prolongation, increasing the risk of cardiac complications compared with other antipsychotics. Equally efficacious agents that do not pose the same level of risk are available. Furthermore, use of droperidol requires a physician on-site 24 hours a day and access to a crash cart, which is not available in all facilities. Thus the youth's safety and the facility's resources were prominent factors guiding this decision.
Finally, the committee adopted a position on the use of seclusion and restraint that is consistent with the position statement put forth by the National Association of State Mental Health Program Directors, approved July 13, 1999. Seclusion and restraint, including medications as chemical restraint, are considered safety interventions of last resort and are not intended for punitive or coercive reasons. They should be used only when there is imminent danger to the youth or other individuals and no safer or more effective alternative is available. Furthermore, these interventions should not be used for staff convenience or in place of adequate staff and facility resources and should be implemented in a safe and humane manner by adequately trained staff. The dignity, privacy, and safety of the patient must be maintained to the greatest extent possible.
The feedback process
The committee strongly recommends that members of the treatment team reevaluate the treatment plan after an aggressive episode and provide feedback to the patient and the patient's family or guardian. Such feedback is particularly important when an additional medication, an extra dose of medication, or seclusion or restraint has been necessary to control the situation. At times the feedback process entails no more than noting in the youth's record that the incident was isolated and that no change in the treatment plan is warranted. This feedback is likely to result in better care, because it provides a mechanism for the treatment team and the line staff who are involved in the acute episode to communicate with the patient and his or her family or guardian and incorporate their input into the ongoing care of the patient; provide an ongoing dialogue to help the patient and his or her family or guardian understand the risks and benefits of the various interventions; reassess the contribution of precipitating factors; determine the effectiveness of the interventions that were implemented; evaluate potential adverse outcomes or unintended effects of certain interventions; establish trends that may require changes in the treatment plan; recommend interventions that have been successful in the past for future episodes; and develop preventive strategies and early intervention strategies that may help to avoid future episodes.
In the case of level 2 interventions, the feedback process should involve a meeting between a member or members of the treatment team and the patient, ideally within two hours of the intervention, to reassess the situation and to review the treatment plan. In the case of level 3 interventions, several follow-up contacts with the patient and the patient's family or guardian are strongly recommended. A meeting between members of the treatment team and the patient to assess the impact of the intervention should occur as soon as possible, but ideally within two hours after seclusion, restraint, or the use of a medication as part of a level 3 intervention. Discussion between members of the treatment team to assess the need to alter the treatment plan should occur within 24 hours of the intervention. Communication between members of the treatment team and the patient's family or guardian should occur promptly, ideally within two hours of the intervention.
In addition, staff members are encouraged to document successful level 1 interventions. In doing so, the treatment team can develop an individualized summary that includes common triggers of aggression, early signs of agitation, and successful interventions for preventing or deescalating the episode. The following approaches are recommended.
At intake, staff should ask the youth and his or her parents or guardian about common triggers of aggression, early signs of agitation, and any successful or preferable interventions—including those in level 3—for managing acute aggression. The staff should make this information easily accessible to the treatment team.
In addition, staff members are encouraged to document successful level 1 interventions, including the context of the situation, any warning signs, and the method used. Prevention strategies also should be noted. Facilities may incorporate this into existing documentation, such as shift notes, or develop new forms.
Finally, the information discussed above should be updated frequently and in conjunction with the data collected at intake to amend the individualized summary with more recent data. In this way, staff will become more familiar with individualized techniques to manage and prevent aggression.