Comorbid medical illness and inadequate health care are major problems for the growing population of older persons with schizophrenia. Approximately 50 percent of psychiatric patients have medical problems that warrant further treatment, and about 35 percent have undetected medical problems (
1). Furthermore, patients with schizophrenia seldom receive treatment in the early phases of physical illness but rather when the disease has become more severe (
2).
Some evidence suggests that there are gender differences in the prevalence and detection of physical illness among patients with schizophrenia. In a study of middle-aged psychiatric outpatients, the most common medical problem for men was gross dental disease, whereas for women it was gynecological disease (
3). Despite the frequency of gynecological diseases in this population, only 10 percent of these problems had been previously diagnosed. Another study found similar rates of preventive care among women with psychiatric illness and women seen in a medical clinic that provided services to persons with low income (
4). However, it is not clear that either group received preventive care in accordance with recommended guidelines. It has also been suggested that women with schizophrenia are more likely to have indicators of estrogen dysfunction—for example, later age of menarche, fewer pregnancies and births, and earlier age of menopause (
5). Such findings further underscore the importance of adequate gynecological care for this patient population.
The purpose of the cross-sectional study reported here was to compare gynecological variables and use of gynecological services among older women who had schizophrenia and a control group of women who were not known to have a psychiatric diagnosis. We hypothesized that older women with schizophrenia would report a history indicative of estrogen dysfunction and would have a lower use of gynecological services than the control group.
Methods
A convenience sample of older women with schizophrenia was obtained from an ongoing study of psychosis in late life at a large research center, which recruited from psychiatric treatment sites. The control group was recruited through advertisements. Data were collected between January 1996 and February 2001. Details of recruitment and the clinical evaluation have been described elsewhere (
6). Briefly, demographic, clinical, and medical information was obtained by self-report and corroborated by medical records. This study was approved by the local institutional review board, and all participants gave voluntary written informed consent.
To be eligible to participate, women had to be in the age range of 50 to 79 years, to be living in the community, to have been medically and psychiatrically stable for at least one month before selection for the study, and to have a diagnosis of schizophrenia or schizoaffective disorder if in the patient group and no known psychiatric diagnosis if in the control group. Women with a diagnosis of substance abuse within the past six months or a known diagnosis of dementia were excluded. A total of 65 women with a diagnosis of schizophrenia or schizoaffective disorder and 51 women with no known psychiatric diagnosis participated in the study.
Demographic and clinical variables, gynecological variables, and gynecological service use were compared between the two groups of women. In the schizophrenia group, psychotic and depressive symptoms were quantified with the Positive and Negative Syndrome Scale (PANSS) and the Hamilton Depression Rating Scale (HAM-D), respectively. For both groups, cognitive functioning was assessed with the Mini-Mental State Exam (MMSE).
Continuous variables were transformed, when necessary, to meet the assumptions of normality. Continuous variables were compared by using independent t tests, and categorical variables were compared by using chi square tests. All statistical tests were two tailed, and significance was set at .05. SPSS for Windows was used for the statistical tests.
Results
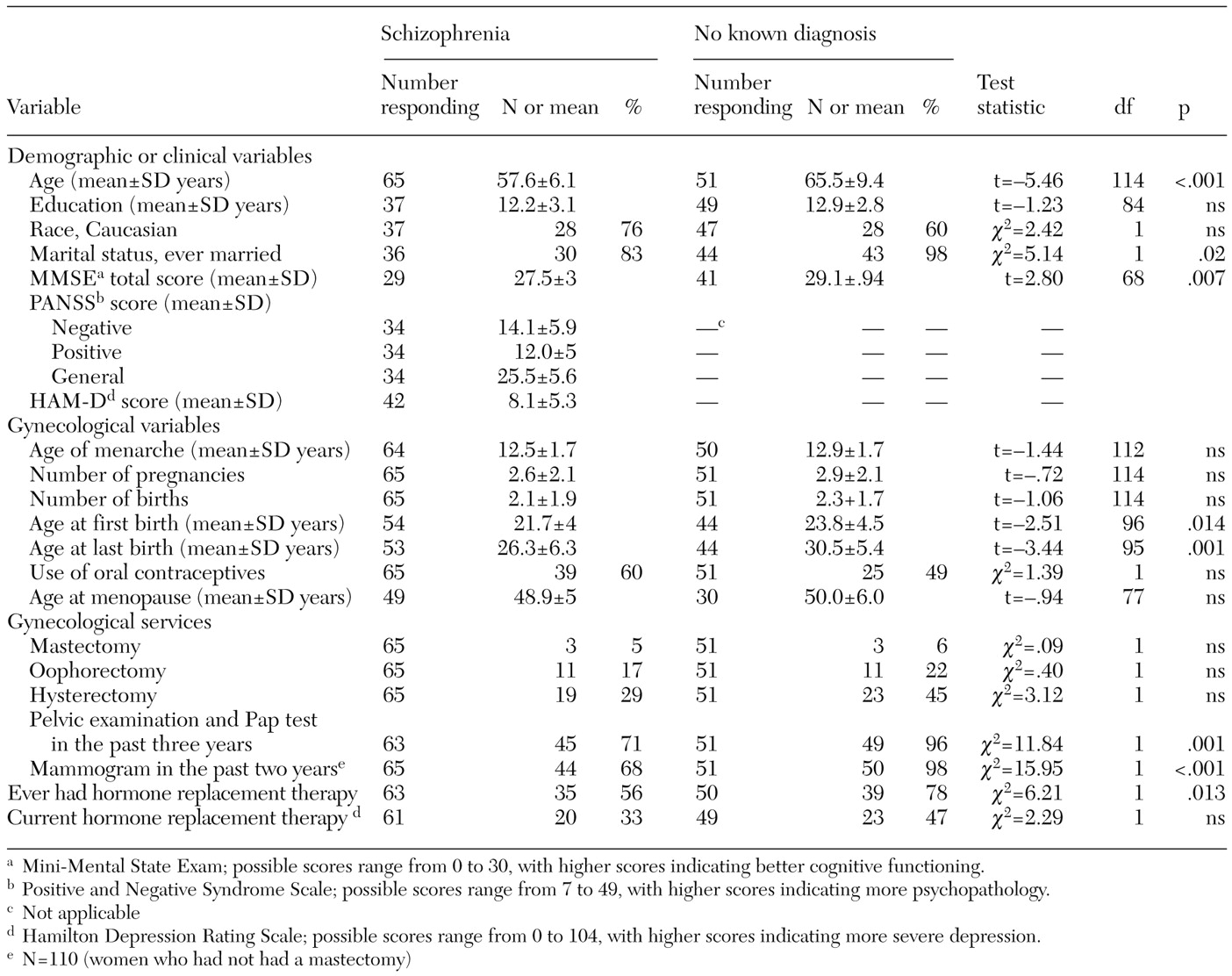
As can be seen in
Table 1, the women with schizophrenia were significantly younger than the women in the control group. The two groups were similar with respect to years of education and ethnicity. Although the women with schizophrenia scored significantly lower on the MMSE than the women in the control group, they did not perform in the cognitively impaired range.
The clinical presentation of the women with schizophrenia was typical of stable outpatients. Positive and negative symptoms, general psychopathology, and depressive symptoms were in the relatively mild range. Approximately half of the patients with a diagnosis of schizophrenia resided in assisted-living facilities, and the rest lived independently. The mean±SD age at onset was 29.2±12.5 years, and the mean duration of illness was 28.7±11.6 years.
The women with schizophrenia and the women in the control group did not differ significantly on many gynecological variables, including age at menarche, age at menopause, and use of oral contraceptives. Although there were no significant group differences between groups in the number of pregnancies or births, the women with schizophrenia were younger than those in the control group when their first and last children were born. The similarity of the two groups in these gynecological variables suggests that the women with schizophrenia did not have estrogen dysfunction.
The two groups of women reported similar rates of mastectomies, oophorectomies, and hysterectomies. Compared with the control group, significantly fewer women with schizophrenia had had a pelvic examination and Pap test in the past three years, had had a mammogram in the past two years, and had ever received hormone replacement therapy.
To control for the age difference between the two study groups, we divided the sample into younger (50 through 64 years) and older (65 through 79 years) subgroups and compared women with and without schizophrenia in each age group. A similar pattern of results was obtained for gynecological service variables, with the exception that the difference in the proportion of women receiving mammograms and Pap tests between the women with schizophrenia and the control group approached significance in the older group only, probably because of the smaller sample size.
Discussion
Women with schizophrenia and women in a control group reported no significant differences in the age of menarche, age of menopause, use of oral contraceptives, and number of pregnancies and births, which suggests that there were no differences in estrogen dysfunction between the two groups. The women with schizophrenia, however, were younger when their first and last children were born. Despite the similarities in many gynecological variables, the groups differed in rates of gynecological service use; women with schizophrenia were less likely to have undergone mammography and pelvic examinations and Pap tests or to have ever been prescribed hormone replacement therapy.
The rate of mammograms among women between the ages of 40 and 49 in California over a two-year period has been reported as 64 percent and among women between the ages of 50 and 64 has been reported as 81 percent (
7). Rates of Pap tests over a three-year period among women between the ages of 40 and 64 was reported as 83 percent (
7). Not only were the women with schizophrenia in our study less likely to receive these services than women in the control group, but the rates of mammography and of pelvic examinations and Pap tests were lower than those of the general population. Rates of current hormone replacement therapy among the women with schizophrenia and the women in the control group were similar to those found in other studies of postmenopausal women (
8). The women with schizophrenia were significantly less likely to ever have received hormone replacement therapy; however, the women with schizophrenia were younger than those in the control group, which perhaps limited the need for postmenopausal hormone replacement therapy.
This study had several limitations. First, information on gynecological variables was self-reported and therefore was subject to recall bias. Second, we used a convenience sample consisting of a large proportion of middle-aged, educated Caucasian women. Information about insurance coverage, other medical care, and perceived need for services was not measured. Finally, the possibility of type I error exists.
Conclusions
Women with schizophrenia were significantly less likely to receive mammograms and pelvic examinations and Pap tests and to have ever used hormone replacement therapy than were women with no known psychiatric diagnosis, and the rates of reproductive-cancer screening were far below those reported for the general population. Interventions at the system, provider, and patient level are needed to promote the use of cancer screening and other appropriate gynecological services among older women with schizophrenia.
Acknowledgments
This work was supported in part by grants MH-01580, MH-49671, MH-43693, and MH-59101 from the National Institute of Mental Health and by the National Alliance for Research on Schizophrenia and Depression, the Department of Veterans Affairs, and the Mental Illness Research, Education, and Clinical Center of Veterans Integrated Service Network 22 (VA Desert-Pacific Healthcare Network).