Study strengths and limitations
Although this study provided clinically detailed nationally representative data that reflect patients with schizophrenia who are treated by APA member psychiatrists in the full range of treatment settings, the study had several limitations. First, the study relied on psychiatrist-reported data and had limited data on the clinical context of treatment in terms of phase of illness, treatment history, and response to treatment. These limitations make it difficult to determine and model the extent to which psychiatrists are providing treatment that is consistent with many of the guideline recommendations. For example, for a majority of patients currently experiencing moderate to severe psychotic symptoms, we know the percentage of patients currently receiving clozapine; however, we do not know the proportion who ever received an adequate trial of another antipsychotic and whether these patients were ever offered or prescribed clozapine. Because of these limitations many of our guideline-conformance measures are somewhat crude. Because we do not have data on the indications for which medications were prescribed, we do not know whether benzodiazepines were prescribed for anxiety, agitation, sleep problems, or treatment-resistant psychotic symptoms. APA and PORT recommendations caution against using benzodiazepines for treatment-resistant psychotic symptoms.
We also did not have data on consumer preferences and the extent to which treatments were ever offered or provided to patients—for example, depot medications, psychotherapy, and vocational rehabilitation. With respect to the psychosocial recommendations studied, we did not have data on the type of case management or on the indications for vocational rehabilitation. Reliance on psychiatrist-reported data of treatments provided in the past 30 days may also significantly underestimate some measures, including side effects, treatment adherence, and substance use.
Because of the clinical caveats surrounding the guidelines, it was difficult to determine whether many of the recommendations were followed appropriately. In addition, our data did not clearly specify the intensity, frequency, and duration of treatments. Consequently, we were able to examine only general treatment patterns related to the PORT and APA recommendations.
Summary of key findings and implications
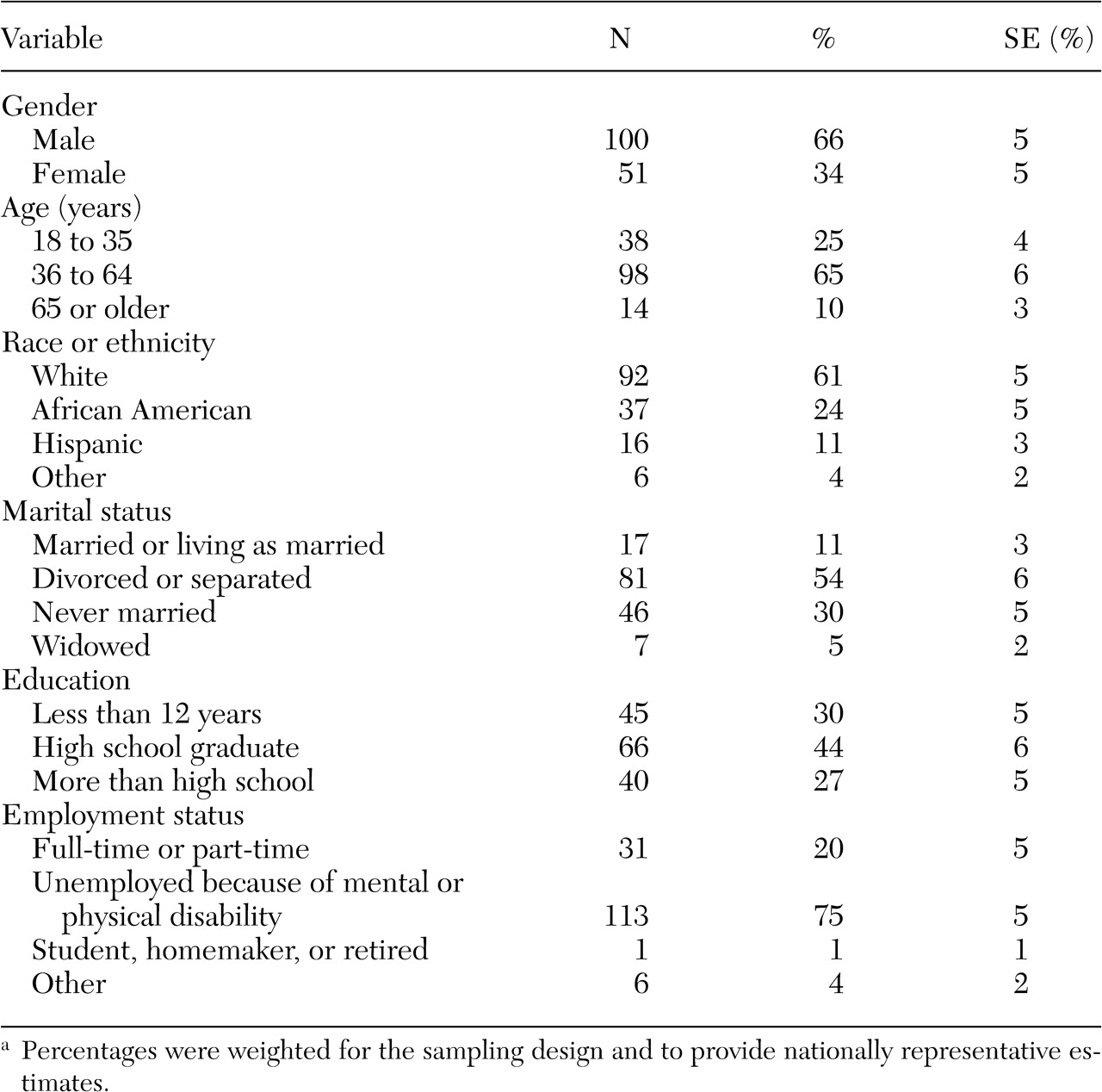
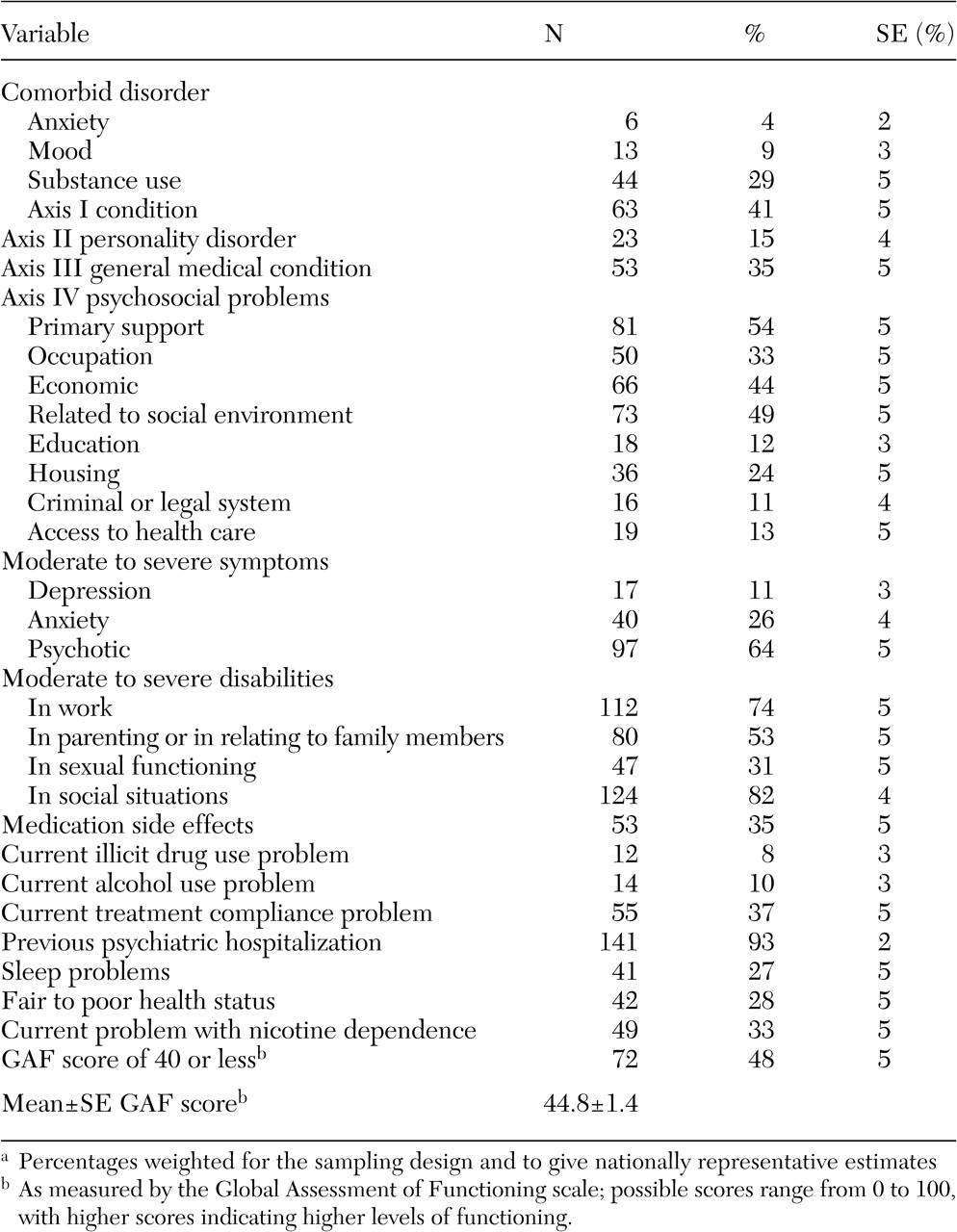
Overall, these data indicate that patients with schizophrenia who are treated by psychiatrists have highly complex clinical problems and are markedly disabled; 75 percent of our sample were unemployed because of a mental or physical disability. Psychiatrists reported that a significant proportion of the patients were experiencing medication side effects (35 percent) and had problems adhering to treatment (37 percent).
Most patients generally appeared to be receiving guideline-consistent psychopharmacologic treatment, and rates for this type of treatment were consistent with the previous PORT research findings reported by Lehman and Steinwachs (
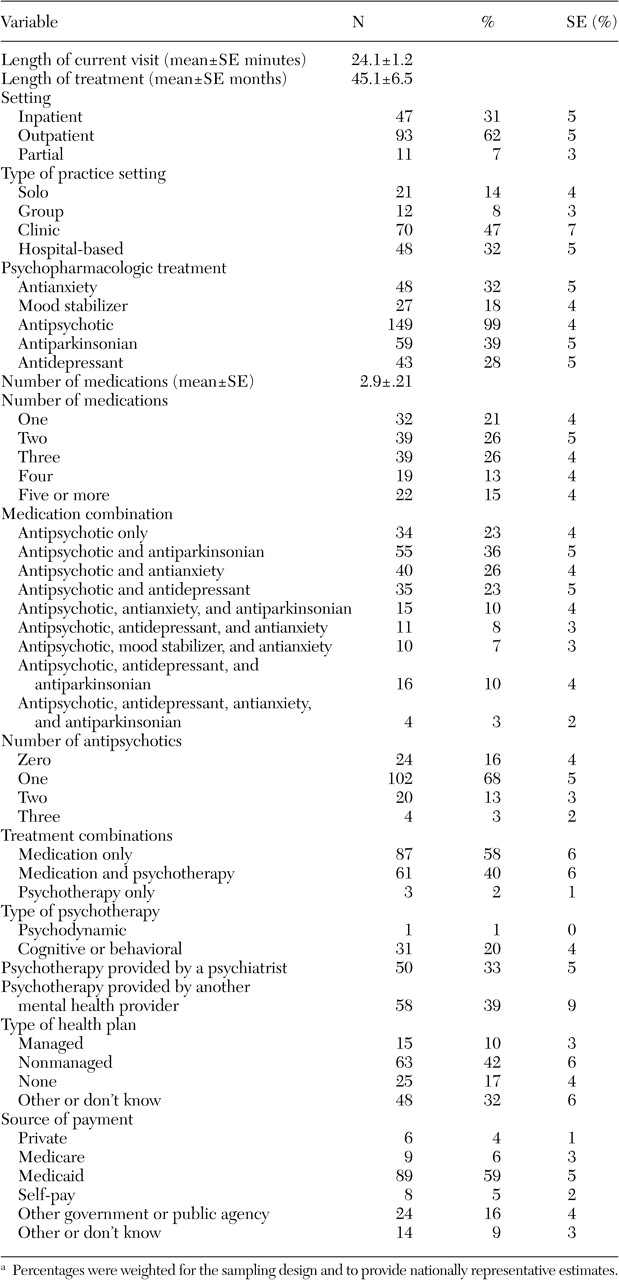
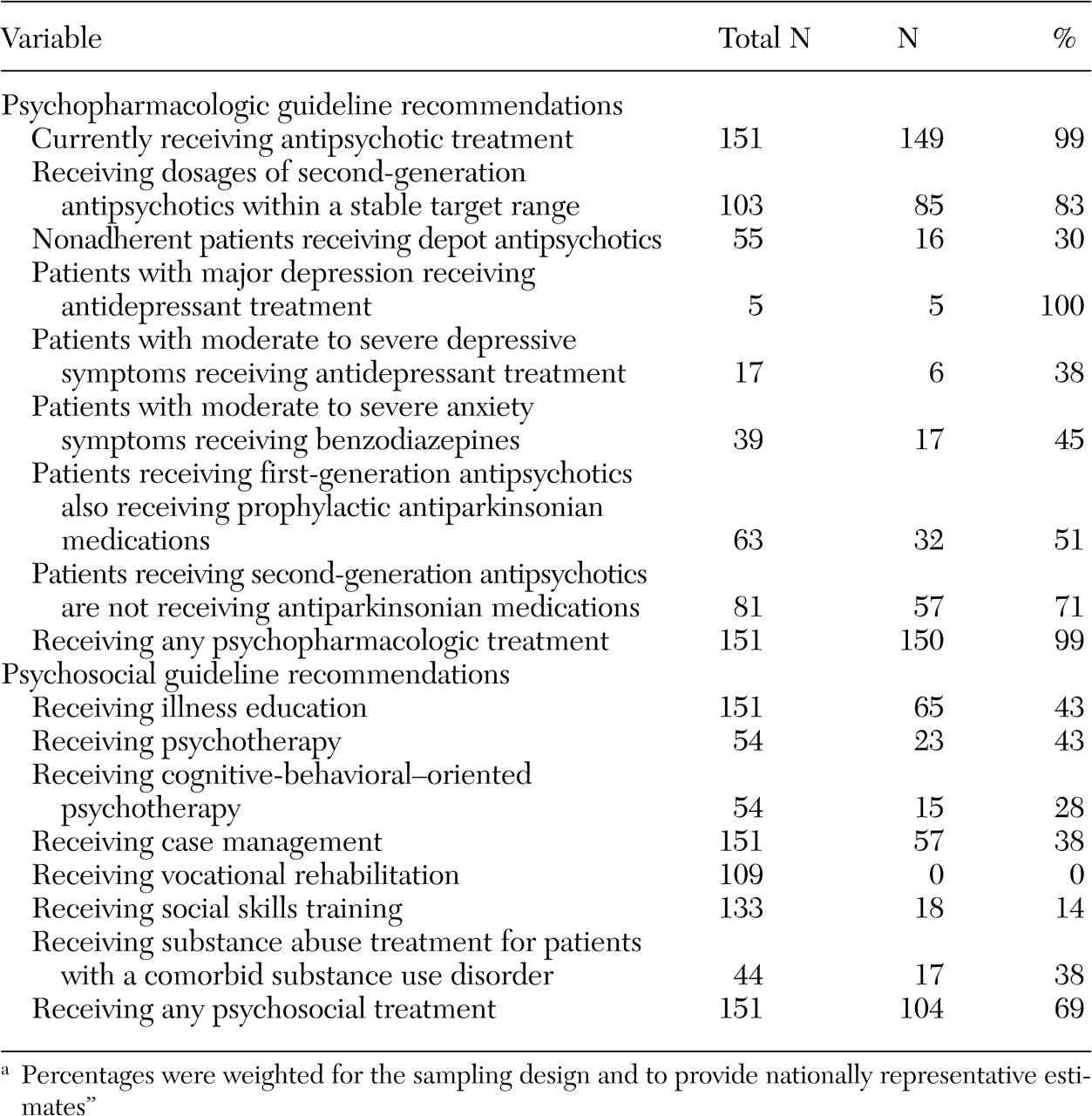
12). Our findings showed that the psychopharmacologic treatment was characterized by significant polypharmacy, with a mean of three medications prescribed per patient. A significant proportion of patients were also receiving two or more antipsychotics, a practice that is not endorsed by the guidelines that were used for this study. In addition, a notable proportion of patients who received second-generation antipsychotics were receiving dosages above the recommended range. This study also found that a majority of patients experienced moderate to severe psychotic symptoms, even though almost all patients in our sample received at least one antipsychotic and received treatment from their psychiatrists for three years on average.
These findings raise questions about whether available antipsychotic medications are used optimally or whether available antipsychotic treatments offer limited effectiveness (as demonstrated in randomized clinical trials) for clinically complex patients treated in routine practice. Some questions about the effectiveness of antipsychotic treatments may be answered through the National Institute of Mental Health's clinical antipsychotic trials of intervention effectiveness study, which is being conducted in a wide range of routine practice settings to assess the long-term effectiveness and tolerability of first- and second-generation antipsychotics.
As for whether currently available medications for the treatment of schizophrenia are being optimized in routine clinical practice, we do not have longitudinal data to characterize the extent to which patients received an adequate trial and dosage of one antipsychotic before another was added. We also do not know the extent to which clozapine was offered to or tried among patients who were receiving an adequate antipsychotic dose and actively experiencing moderate to severe psychotic symptoms.
Depot medications may be underused: 70 percent of the patients with current treatment adherence problems were not receiving depot antipsychotics. Rates of depot antipsychotic use in our study were consistent with those found by Citrome and colleagues (
27). In that study rates ranged from 12 to 39 percent in 21 psychiatric hospitals in New York State. Our data also indicate that a significant proportion of patients (29 percent) who received second-generation antipsychotics may be receiving antiparkinsonian medications unnecessarily. This issue warrants follow up in light of findings that show that several second-generation antipsychotics prescribed at higher dosages may have greater than expected side effect profiles (
28). In these areas clinical practice may be ahead of evidence-based guidelines.
The data that showed limited access to the psychosocial treatments that are recommended by the evidence-based guideline raises concerns. Our findings are consistent with those of Young and colleagues (
29), who studied 224 patients at two public mental health clinics and found that 52 percent received inadequate psychosocial care. The rates of psychotherapy that we found in our sample were consistent with those in the PORT study (
12). Although rates of vocational rehabilitation in our study were significantly lower than in the PORT study (no patients in our study compared with 23 percent), the PORT study included patients who reported looking for work or participating in a vocational rehabilitation program and patients for whom vocational rehabilitation was part of the treatment plan, regardless of whether vocational rehabilitation services were provided.
Vocational rehabilitation services for unemployed patients in our sample appeared to be nonexistent; no unemployed patients were currently receiving these services, although 14 percent of the employed patients were. This finding is particularly disturbing because of the high rates of unemployment among individuals with schizophrenia. Studies suggest that vocational rehabilitation can be effective in significantly increasing employment rates and levels of earned income in this population (
14,
30). Cohort and cross-sectional studies indicate that the relationship between employment outcomes and symptoms is complex, and symptom severity alone does not determine a patient's suitability for vocational rehabilitation services (
31,
32). A growing number of clinicians, patient advocates, and researchers have called for expanded vocational and psychosocial rehabilitation services to improve functional outcomes for individuals with schizophrenia (
33,
34).
The patterns that we identified are troubling for two major reasons. First, patients who are already receiving treatment from a psychiatrist would be expected to represent patients with greatest access to needed treatments. Second, for patients with public insurance, access to psychosocial treatment appears to be particularly limited: only 8 percent of patients with Medicare and 41 percent of patients with Medicaid received psychotherapy from a mental health care provider in the past 30 days. Provision of substance use treatment for this population was also strikingly low. Collectively, these data suggest considerable unmet need for psychosocial treatment services among individuals with schizophrenia.
Future research
Several future studies are being conducted or planned that can help illuminate the patterns of treatment for schizophrenia and the reasons for these patterns. In addition to the study described above on clinical antipsychotic trials of intervention effectiveness, we are currently completing a study of medication management decisions in schizophrenia. Using a large, nationally representative sample of psychiatrists in routine psychiatric practice, this study will evaluate the extent to which routine medication management of schizophrenia conforms to other evidence-based treatment recommendations. Furthermore, this study will identify factors affecting clinical decision making and modifiable factors associated with not conforming with these treatment recommendations.
To assess patterns of treatment and the extent to which treatments provided are consistent with evidence-based practice guideline treatment protocols, PRN studies are now being pilot tested to capture longitudinal data on the treatment history of psychiatric patients, patient preferences, treatment adherence, and patient response and outcomes of treatment. These studies will assess the extent to which specific subgroups of patients—such as patients with different severity levels, specific comorbid axis I disorders, or significant psychosocial problems who receive different types, combinations, intensity, and duration of treatment—have superior outcomes. These data will help in assessing the extent to which some of the current clinical practices identified in this study, which are not consistent with evidence-based guideline recommendations, are associated with favorable outcomes of treatment.