At least half of all new HIV infections in the United States are among people younger than 25 years (
1). In this age group 10,295 persons currently live with HIV-AIDS (
2). Delinquent youths are at particular risk of HIV-AIDS. The most recent study found that nearly two-thirds of juvenile detainees had engaged in ten or more HIV-AIDS risk behaviors related to sex or drugs (
3).
Studies of youths in treatment and in the general population (
4,
5) suggest that major mental disorders (major depressive episode, manic episode, and psychosis), especially with comorbid substance use disorders (
6), may be an important risk factor for HIV-AIDS risk behavior among delinquent youths. One study examined symptoms of psychiatric disorders, drug use, and their relationship to HIV-AIDS risk behaviors in detained youths (
7). No study has examined mental disorders, comorbid substance use disorders, and their relationship to HIV-AIDS risk behaviors in detained youths.
This omission is critical. Among juvenile detainees, almost three-quarters of females and two-thirds of males have one or more psychiatric disorders, and approximately one-half have one or more substance use disorders (
8). Comorbid mental and substance use disorders are common. Among detainees with a major mental disorder, nearly three-fifths of females and almost three-quarters of males have one or more substance use disorders (
9).
HIV-AIDS risk behaviors of delinquent youths are a community public health problem because juveniles in detention have a median stay of only two weeks (
10). Moreover, studying juvenile delinquents yields important information about other youths at risk of HIV—runaways and those who use drugs or who trade sex for money—many of whom will eventually cycle through the detention center (
8).
This study examined major mental disorders and substance use disorders, comorbidity, and HIV-AIDS risk behaviors in delinquent youths.
Methods
The participants were part of the Northwestern Juvenile Project, a longitudinal study of 1,829 youths aged ten to 18 years who were initially arrested between 1995 and 1998 and detained at the Cook County Juvenile Temporary Detention Center in Chicago (
8,
9).
The random sample was stratified by gender, race or ethnicity (African American, non-Hispanic white, and Hispanic), age (ten to 13 years and 14 years and older), and legal status (processed as a juvenile or as an adult). We began collecting data on HIV-AIDS risk behaviors in 1997, midway through the study. Additional information on our methods and human subjects procedures has been published elsewhere (
8,
9). The study was approved by the institutional review board of Northwestern University.
Measuring HIV-AIDS risk
We examined sexual risk behaviors, injection drug use risk behaviors, and other behaviors associated with the exchange of body fluids. We also examined alcohol and other drug use because it can lower inhibitions, cause motor impairment, and increase the likelihood of unprotected sex, rough sex, exchanging sex and drugs, and injecting drugs. Interviewers (master's level or equivalent) gathered HIV-AIDS risk data with the Northwestern Juvenile Project's AIDS Risk Behavior Assessment (ARBA), which was compiled from three sources: the Risk Behavior Assessment, developed by the National Institute on Drug Abuse (NIDA) (
11); the Adolescent Health Survey, also developed by NIDA (
12); and selected items from the Diagnostic Interview Schedule for Children, Version 2.3 (DISC), developed by Columbia University (
13). We developed the ARBA because existing instruments that had been designed for adolescents and young adults did not assess the breadth, frequency, and severity of HIV-AIDS risk behaviors that are common among delinquent youths. Experts reviewed the ARBA, and we used a pilot study to test it on 58 participants. Items on the ARBA assess either behaviors over the lifetime or behaviors within specific time frames (for example, within the past month or past three months).
Assessing psychiatric disorders
We defined major mental disorders as major depressive episode, manic episode, or psychosis. To determine
DSM-III-R diagnoses within the past six months we used the DISC 2.3, the latest version available when the Northwestern Juvenile Project began in 1995. The DISC is highly structured, contains detailed symptom probes, has acceptable reliability and validity (
13), and requires relatively brief training. Further information on the DISC and prevalence of disorders can be found in studies by Teplin and colleagues (
8) and Abram and colleagues (
9).
Data analysis
Because we stratified our sample by gender, race or ethnicity, age, and legal status, we weighted all prevalence estimates to reflect the distributions of these variables in the detention center's population. Loglinear models were used for all analyses; all reported standard errors and tests of significance used Taylor series linearization to correct for design characteristics (
14). We used two-tailed tests; our level of significance for all tests was .05. We calculated specific differences between groups only when the overall test was significant.
Results
Of 1,052 detainees eligible for the study, 41 (3.9 percent) refused to participate, 14 (1.3 percent) did not complete the HIV-AIDS questions because of interviewer error, one (.1 percent) was released from the detention center before finishing the interview, and 196 (18.6 percent) left the detention center before we could locate their caretakers for consent or to schedule an interview. The final sample was 800—340 females and 460 males. The sample included 145 non-Hispanic whites (18 percent), 430 African Americans (54 percent), 223 Hispanics (28 percent), and two youths who self-identified as "other" race or ethnicity. No significant differences in refusal rates were found by gender, race or ethnicity, or age. Few data were missing; 760 participants (95 percent) had data for all variables; only eight (1 percent) were missing data for three or more items.
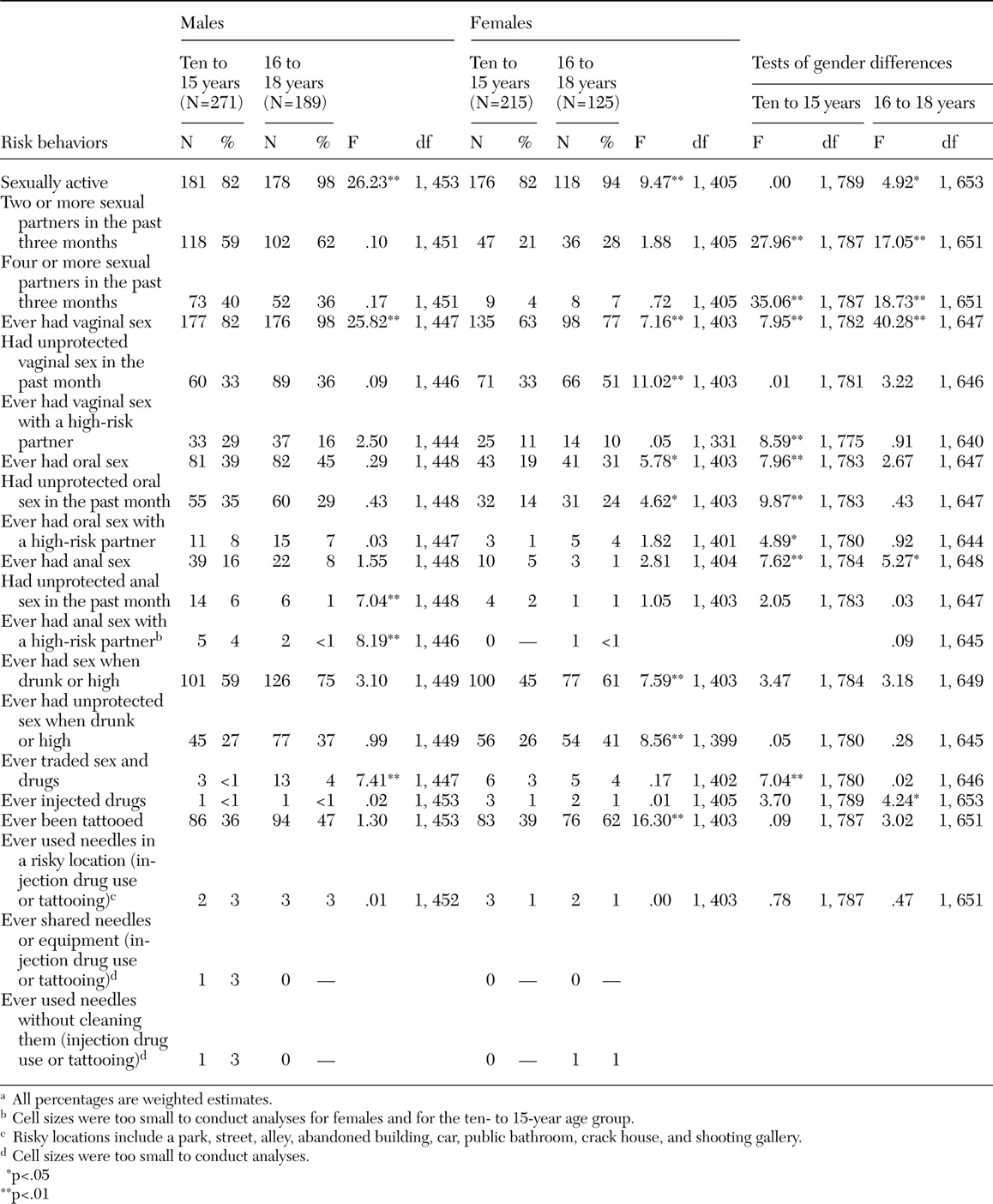
Table 1 shows the prevalence of 20 HIV-AIDS risk behaviors by age group (age ten to 15 years and age 16 to 18 years) for males and females. We examined age differences among males and females and gender differences within the age groups. Many of the risk behaviors were more common among older participants. Among participants in both age groups, significantly more males than females had engaged in several of the sexual risk behaviors. In the group of youths aged ten to 15 years, significantly more females than males had traded sex and drugs.
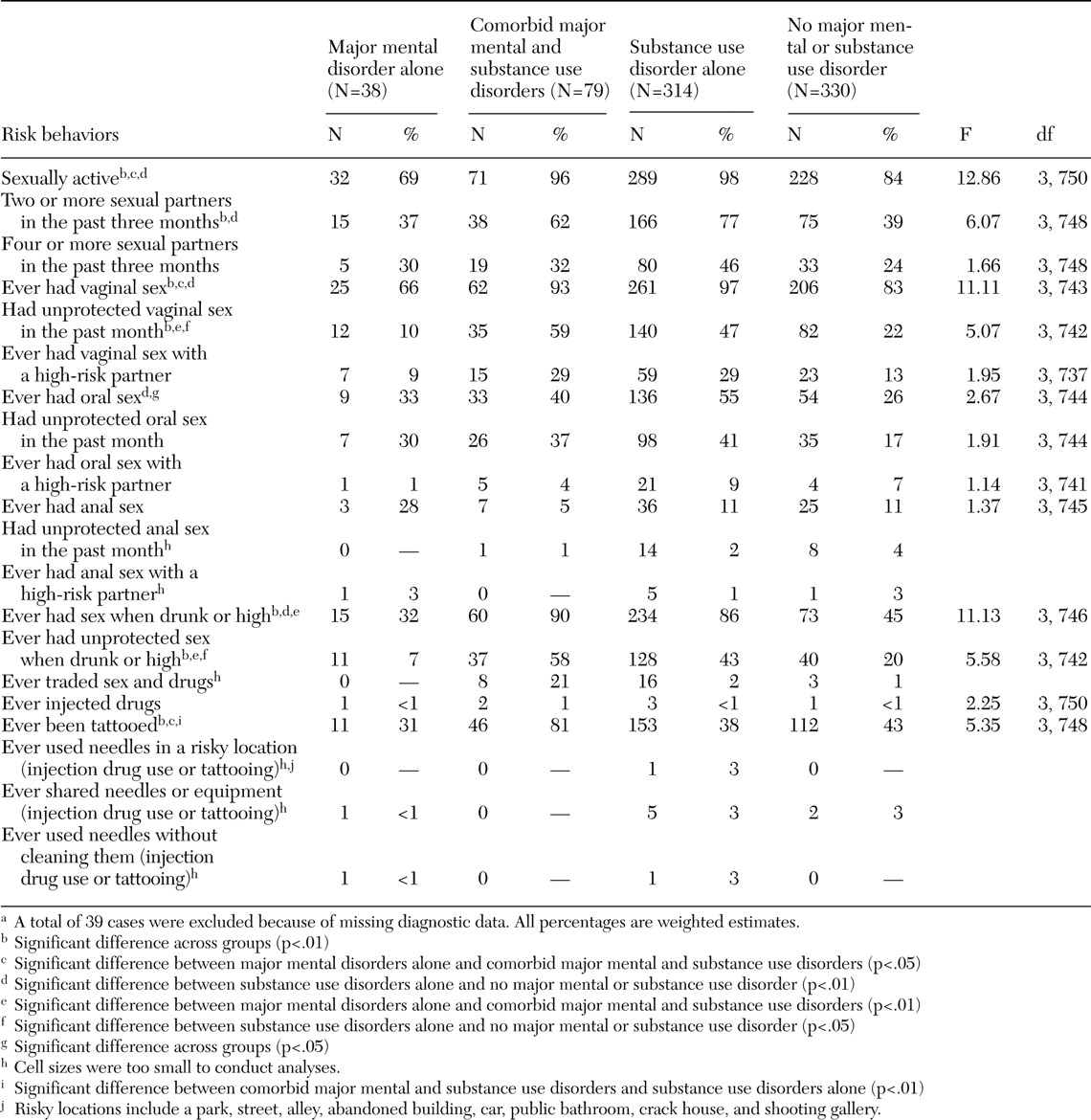
Table 2 shows the prevalence of 20 HIV-AIDS risk behaviors of four mutually exclusive groups: major mental disorders alone, comorbid major mental and substance use disorders, substance use disorders alone, and no major mental or substance use disorder.
Youths with major mental disorders
We compared youths with major mental disorders alone and those without any major mental or substance use disorder; no significant differences were found. Next, we compared youths with major mental disorders alone and youths with comorbid major mental and substance use disorders. Significantly more youths with comorbid disorders had been sexually active, had had vaginal sex, had had recent unprotected vaginal sex, had engaged in sex while drunk or high, had engaged in unprotected sex while drunk or high, or had been tattooed.
Youths with substance use disorders
We compared youths with substance use disorders alone and those without any major mental or substance use disorder. Significantly more youths with substance use disorders alone engaged in seven of the 14 sexual risk behaviors that are listed in
Table 2. Next, we compared youths with substance use disorders alone and those with comorbid major mental and substance use disorders. HIV-AIDS risk behaviors were prevalent in both groups; few differences were found. Significantly more youths with comorbid disorders had been tattooed than youths with substance use disorders alone.
Discussion
Our findings demonstrate that all delinquent youths are at great risk of HIV-AIDS, irrespective of gender, age, or psychiatric disorder. Delinquents with substance use disorders, either with or without comorbid major mental disorders, are at particular risk. More than 63 percent of detainees with any substance use disorder, either alone or with a comorbid major mental disorder, engaged in five or more sexual risk behaviors.
As with the other groups of detainees, youths with major mental disorders had a high prevalence of most HIV-AIDS risk behaviors, much higher than the rates found among youths in the general population (
15). Comorbid substance use disorders increased the prevalence of most HIV-AIDS risk behaviors. Among youths with comorbid major mental and substance use disorders, 96 percent had been sexually active, 62 percent had had multiple partners within the past three months, and 59 percent had had unprotected vaginal sex in the past month.
Our findings demonstrate that prevention is key. Many of the most serious risk behaviors—injection drug use and sharing needles—are still uncommon but may develop among detained youths as they age (
16). Early interventions can reduce the likelihood that these behaviors will be initiated (
17,
18). Providing HIV-AIDS risk interventions to youths while they are in custody could reach a population that may not receive interventions in the community. Although most schools now provide HIV-AIDS education (
19), many youths involved in the juvenile justice system do not attend school regularly (
20).
Future directions
Studies of persons with comorbid major mental and substance use disorders. Substance use impairs decision-making ability, lowers inhibitions, increases impulsivity, reduces perceptions of personal risk, and decreases the ability to negotiate safe-sex practices (
4,
21,
22). Future studies should examine how major mental disorders and comorbid substance use disorders affect the onset, persistence, discontinuation, and recurrence of HIV-AIDS risk behaviors. Examining comorbid substance use disorders is critical because they are so prevalent in populations at risk of HIV-AIDS—for example, youths in the juvenile justice system (
9), youths in mental health treatment (
23,
24), homeless youths (
25), and adult jail detainees (
26,
27). Despite the importance of studying comorbid substance use disorders, we found fewer than ten studies of HIV-AIDS risk of persons with major mental disorder and comorbid substance use disorder, either in community or correctional samples. Unless comorbid conditions are controlled for, we cannot know whether the apparently high rates of HIV-AIDS risk behaviors among persons with major mental disorders are an artifact of their substance use disorders.
Prospective longitudinal studies of high-risk samples. Longitudinal studies are the best way to examine developmental sequences of HIV-AIDS risk behaviors, identify critical periods of vulnerability, highlight modifiable risk factors, show which preventive interventions may be most beneficial, identify specific patterns of risk within key diagnostic groups, and determine whether mental health or substance use treatment decreases HIV-AIDS risk behaviors. Studies of correctional populations are especially needed. Studies of incarcerated adults suggest that delinquent youths are at substantial risk of contracting HIV as they age (
28). Data from 2001 showed that 2 percent of state prison inmates and just over 1 percent of federal prison inmates were known to be infected with HIV, rates much higher than those found in the general population (
28).
Limitations
Several cautions are warranted. Our findings, drawn from one site, may pertain to only detained urban youths who have high base rates of HIV-AIDS risk behaviors. Even with our large sample, there were too few youths with major mental disorders to examine contextual variables known to be correlated with HIV-AIDS risk behaviors. Moreover, our findings might differ somewhat if we had been able to use DSM-IV instead of DSM-III-R criteria.
Conclusions
The Surgeon General will soon issue a call to action on correctional health. HIV-AIDS is one of the most critical health disparities in our nation, particularly so in correctional populations, which are composed disproportionately of poor persons, poorly educated persons, and persons from racial or ethnic minority groups. Three-quarters of persons newly infected with HIV in the United States in 2002 were African American or Hispanic (
29). Among minorities, young disadvantaged women—an increasing proportion of correctional populations—are at particularly high risk of HIV-AIDS (
30). Persons from minority groups are disproportionately affected, in part, because social problems associated with poverty increase the risk of HIV-AIDS (
31). Reducing poverty, health disparities, and drug use could reduce the HIV-AIDS epidemic among delinquent youths and in the general population (
32). Greater coordination between community services and correctional facilities can reduce the prevalence of HIV-AIDS risk behaviors of juvenile delinquents and stem the spread of HIV infection among young people.
Acknowledgments
This work was supported by grant R01-MH-54197 from the National Institute of Mental Health, grant R01-MH-59463 from the Division of Services and Intervention Research and the Center for Mental Health Research on AIDS in the National Institute of Mental Health, and grant 1999-JE-FX-1001 from the Office of Juvenile Justice and Delinquency Prevention.
Major funding was also provided by the National Institute on Drug Abuse; the Center for Mental Health Services, the Center for Substance Abuse Prevention, the Center for Substance Abuse Treatment in the Substance Abuse and Mental Health Services Administration; the National Center for Injury Prevention and Control and the National Center for HIV, STD, and TB Prevention in the Centers for Disease Control and Prevention; the National Institute on Alcohol Abuse and Alcoholism; the Office of Research on Women's Health, the Center on Minority Health and Health Disparities, and Office of Rare Diseases in the National Institutes of Health; the William T. Grant Foundation; and the Robert Wood Johnson Foundation. Additional funds were provided by the John D. and Catherine T. MacArthur Foundation, the Open Society Institute, and the Chicago Community Trust.
The authors are indebted to Ann Hohmann, Ph.D., Kimberly Hoagwood, Ph.D., Heather Ringeisen, Ph.D., Jacques Normand, Ph.D., Helen Cesari, M.S., Richard Needle, Ph.D., Grayson Norquist, M.D., Delores Parron, Ph.D., and Celia Fisher, Ph.D. The authors thank project staff members Amy Lansing, Ph.D., and Laura Coats. The authors also thank the staff of the Cook County Juvenile Court and the Cook County Juvenile Temporary Detention Center, especially David Lux.