A number of studies assessing volumetric measurements of regional brain structures in bipolar disorder have been published in recent years, but results have been inconsistent with lateral ventricular enlargement being the most consistently reported finding (
1–
3). Markedly conflicting findings have been reported for some structures. For example, various studies reported increased (
4–
7), reduced (
8–
11), or no difference in amygdala volume (
12). A previous meta-analysis of methodologically robust volumetric magnetic resonance imaging (MRI) studies of bipolar disorder based on published aggregate data by our group revealed right ventricular enlargement as the only brain region that differed significantly from healthy subjects (
13). Extensive heterogeneity existed for several other brain regions, including the amygdala, subgenual prefrontal cortex, thalamus, and the third ventricle (
13). A recent meta-analysis of neuroimaging studies of bipolar disorder that included computed tomography and qualitative magnetic resonance studies highlighted the low statistical power of most studies and identified lateral ventricular enlargement as the only consistent volumetric finding (
14). This report included a metaregression analysis for sources of heterogeneity and found that those patients taking lithium were more likely to have increased gray matter volume. A further recent meta-analysis again identified lateral ventricular enlargement but also noted whole brain and prefrontal lobe reductions and globus pallidus enlargement in bipolar disorder (
15).
Meta-analysis is the most widely used method for averaging statistical effect sizes from different studies (
16) and is usually based on combining effect sizes from published literature rather than analyzing pooled individual patient data. Meta-analysis, however, is associated with several methodological problems, the most significant of which is the frequent inclusion of studies that are heterogenous in nature. Studies included in meta-analyses commonly differ in aspects of their design. Each study in a meta-analysis is drawn from somewhat different populations, depending on the patients chosen and the investigations and conditions unique to the study. Thus, even if each study has a large patient sample, the investigation effect would be expected to differ; these differences are known as random effects and describe the between-study variation with regard to an overall mean effect of all studies (
17). This between study variance is difficult to control using conventional meta-analytical techniques.
However, analysis pooling individual patient data from different studies, or mega-analysis (
18,
19), helps to adjust for between-study differences. In MRI datasets, unique conditions to individual studies include MRI field strengths and pulse sequences and different techniques to delineate anatomical brain regions. These differences cannot be controlled for using meta-analysis; however, mega-analysis has the advantage of being specifically able to control for research center and thus control for differences in MRI techniques between research centers. Additionally, because reanalysis of pooled patient data requires collaboration of the investigators who conducted the studies, it enables better identification of relevant studies and the provision of a more balanced interpretation and wider endorsement of results (
20).
Subjects
We invited research groups that had employed robust methodology in data acquisition by setting certain minimum requirements, and we used similar inclusion criteria to our previous aggregate data meta-analysis (
13): 1) an MRI scanner strength of 1T or greater, 2) regional brain structure measurement based on contiguous slices, 3) included individuals aged 16 to 55 years, 4) brain structures independently examined by three or more research groups, and 5) patients with bipolar disorder only—data contributed by research groups including individuals with schizoaffective disorder, schizo-phrenia, or unipolar depression alone were not included.
We identified 22 research groups meeting these criteria. Senior representatives from each group were invited to participate and submit to us their relevant individual raw data for this mega-analysis. Data requested included participant diagnosis, relevant brain volumetric measurements, demographic details including age and gender, clinical details about the age of onset and course of illness, and medication use. Researchers from 11 groups submitted data on 321 individuals with bipolar I disorder and 442 healthy subjects. Data on a further 29 individuals with bipolar II disorder were submitted; however due to this limited data, we only examined individuals with bipolar I disorder. The majority of these data have been previously published (Table S1 in Supplement 1) (
4–
9,
24–
43). Projects from each research center were approved by the respective ethical committees. Data from the different research centers were merged into a single spreadsheet and corrected for inaccuracies, duplications, and inclusion criteria (e.g., adolescents under 16 years and individuals with bipolar II disorder were excluded from further analysis).
Linear mixed effects regression models were used where the research center was incorporated as a random effect to account for the correlation due to individuals within each research center and possible heterogeneity between research centers. As the factor, gender, and covariates, age + brain slice thickness, could be potential confounders, these were forced into each model in addition to the primary diagnostic group variable. Summary statistics and point and 95% confidence interval (CI) estimates of the difference in the mean adjusted response variables across the levels of diagnostic group were reported. The level of statistical significance was set at α = .05, and effect sizes using Cohen's
d were also reported. Model diagnostics were performed using suitable residual plots. Ventricular volume distributions were normalized through log transformation. All analysis was performed using the Statistical Package for Social Sciences 15.0 for Windows (SPSS 15.0 for Windows, SPSS, Inc., Chicago, Illinois) and
R (version 2.6.1) (The
R project for statistical computing;
http://www.rproject.org). We corrected for multiple testing using the technique described by Holm (
44).
Our principal analysis compared regional brain volumes between groups (bipolar I individuals vs. healthy subjects). We also performed analyses to ascertain the effect of medication between subgroups (e.g., bipolar disorder individuals treated with lithium vs. bipolar disorder individuals not treated with lithium vs. healthy subjects) and any effect on brain volume or duration of illness and number of hospitalizations.
Results
Demographic and clinical data
The sociodemographic details are provided in
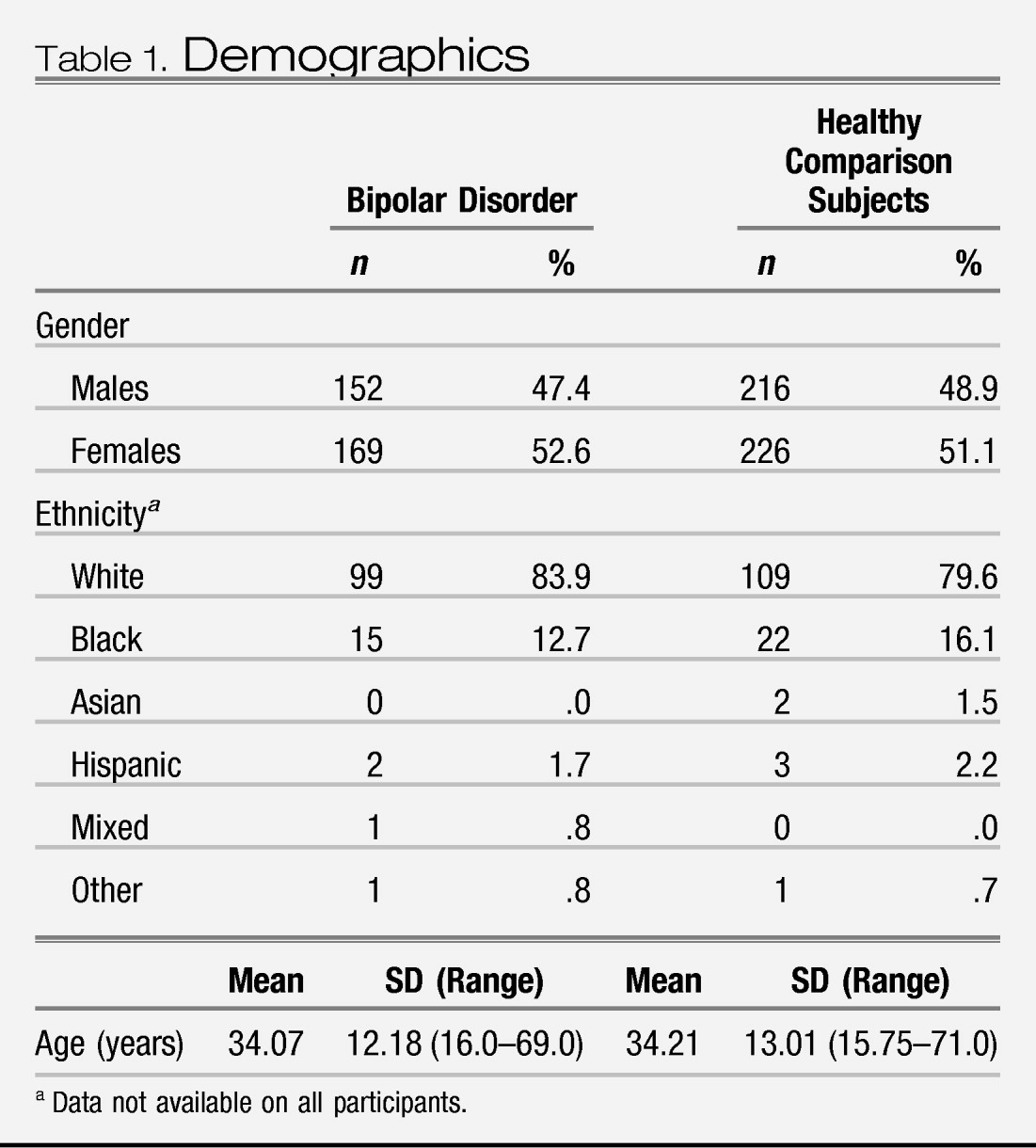
Table 1 and unadjusted regional brain volumes are provided in Table S2 in Supplement 1 for individuals with bipolar disorder and healthy subjects. All research centers used reliable and valid criteria for diagnosing bipolar disorder (Structured Clinical Interview for DSM or the Schedule for Affective Disorders [SADS]) and had appropriate mechanisms for drug coding. Age and gender were similar between the individuals with bipolar disorder and healthy subjects (
Table 1). In individuals with bipolar disorder, the mean age of onset was 21 years (SD = 7), the mean duration of illness was 12 years (SD = 11), and the median number of hospitalizations was 3 (range 0–20). For bipolar individuals with information on medication use at the time of MRI acquisition, 141 subjects (50.4%) were prescribed lithium, 74 (30.6%) were prescribed valproate, 17 (8.9%) were prescribed carbamazepine, 217 (77.5%) were prescribed at least one mood stabilizing agent (lithium, valproate, or carbamazepine), 90 (44.3%) were prescribed an antipsychotic medication, and 26 (24.3%) were prescribed an antidepressant. Our sample included 50 (15.6%) firstepisode bipolar subjects.
Bipolar disorder versus healthy subjects
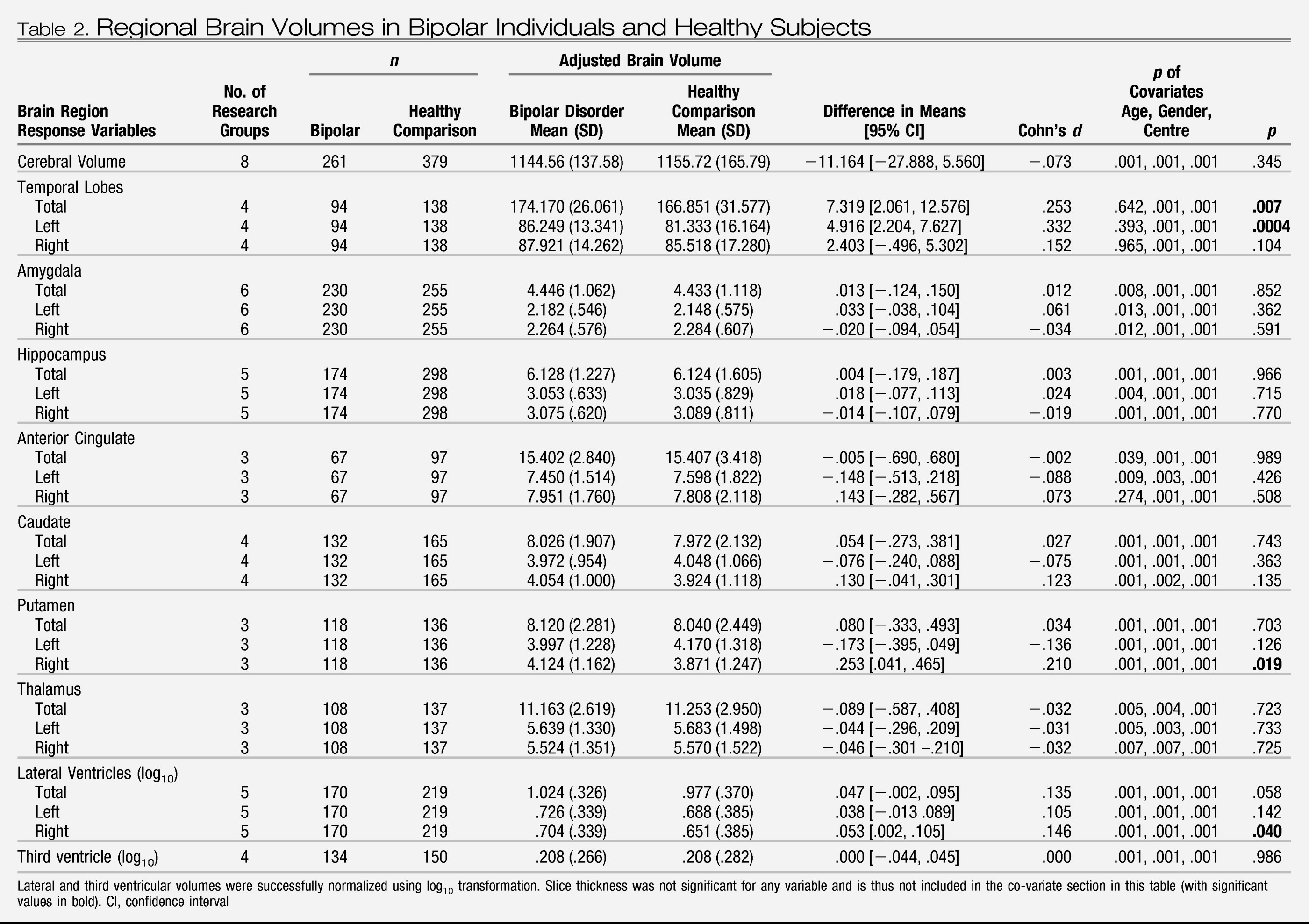
Mean adjusted regional brain volumes (for research center, gender, and age) of individuals with bipolar disorder and healthy subjects are shown in
Table 2. There was a significant difference in total temporal lobe volume between diagnostic groups (
p = .007). The adjusted mean temporal lobe volume was estimated to be between 2.1 and 12.6 mm
3 larger, on average, in bipolar compared with healthy individuals. Bipolar subjects also displayed significantly increased left temporal lobe volume, right putamen volume, and right lateral ventricular volume compared with healthy subjects. No significant differences were found between bipolar and healthy subjects for any other brain region. There was a differential effect of age for hippocampal volume with bipolar subjects having a greater decrease in hippocampal volume with age compared with healthy subjects (
Z = 2.86,
p = .001). This was not evident for other brain regions.
Brain volume and lithium
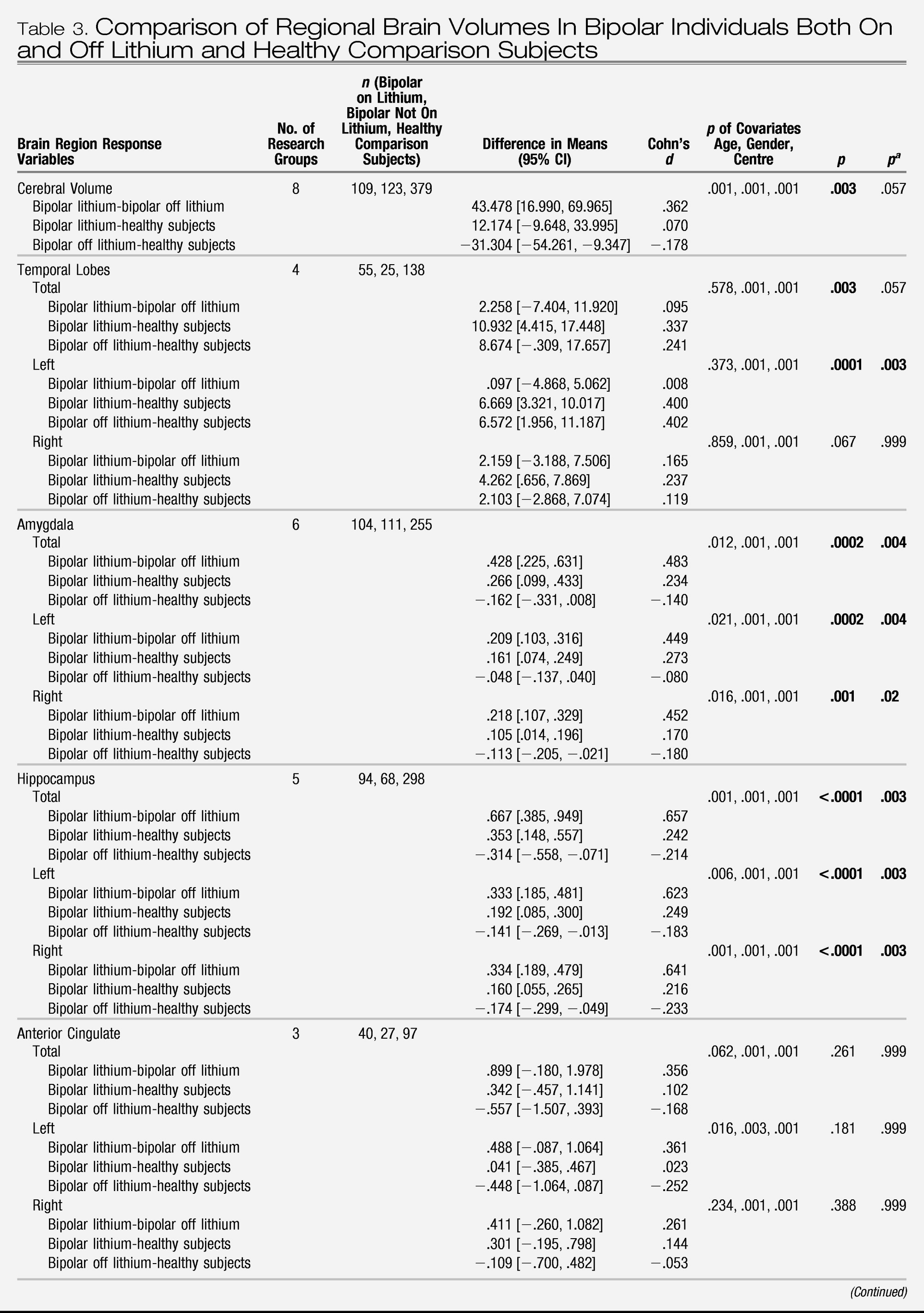
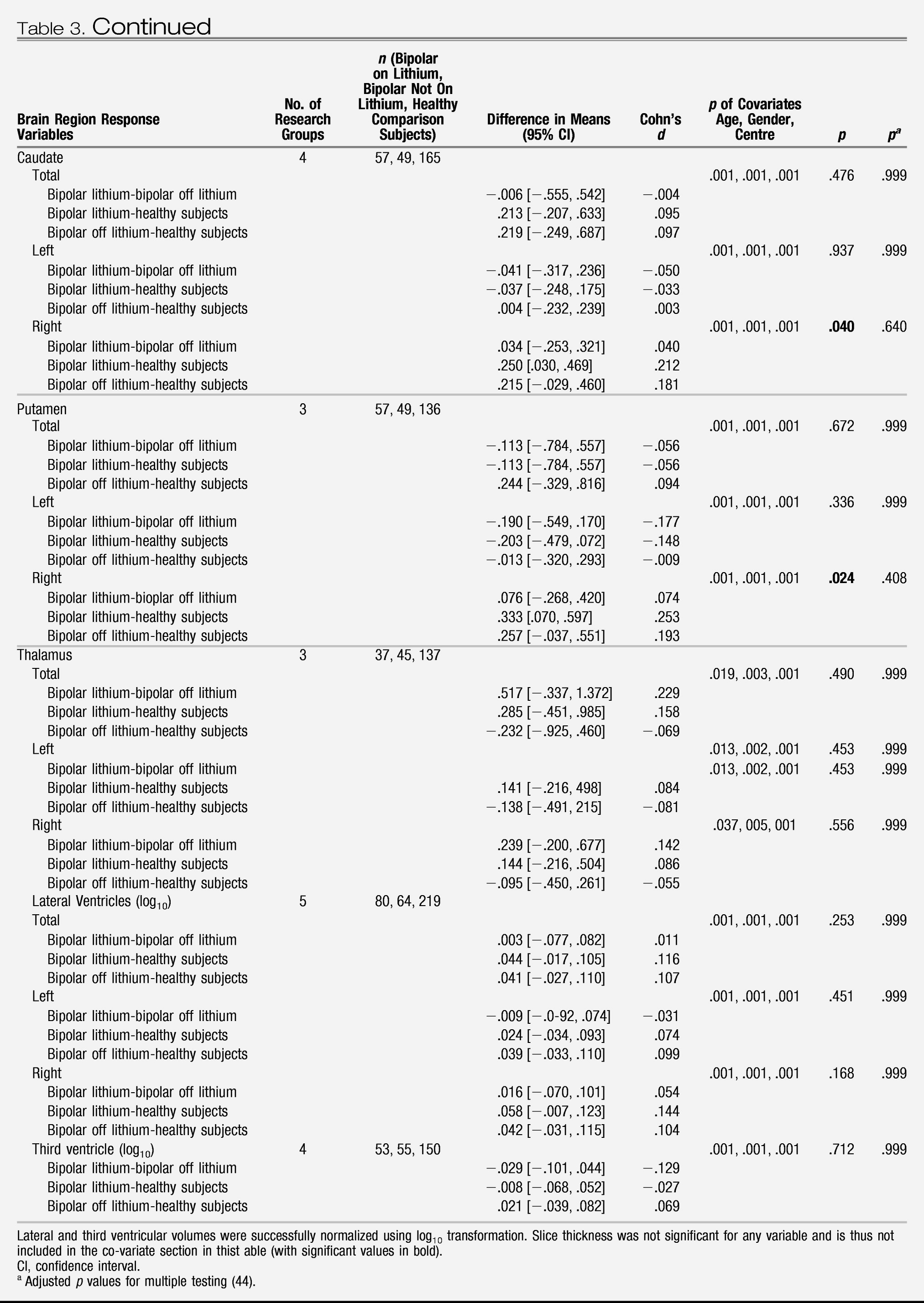
A comparison of regional brain volumes in bipolar patients taking lithium with those not taking lithium and with healthy subjects is provided in
Table 3 Those not taking lithium had a younger mean age (32 years, SD = 12) than both those taking lithium (36 years, SD = 13) and healthy subjects (34 years, SD = 13) (
F = 2.462, df = 2, 750,
p = .037), and there was no significant difference in the duration of illness (
F = 3.112, df = 1, 271,
p = .079) between bipolar patients taking and not taking lithium. No interaction was found between lithium and research center for any brain region. There was evidence of a significant difference in regional brain volume across subject groups. Individuals with bipolar disorder treated with lithium had larger mean total, left, and right hippocampal volume (
p < .001) and total, left, and right amygdala volume (
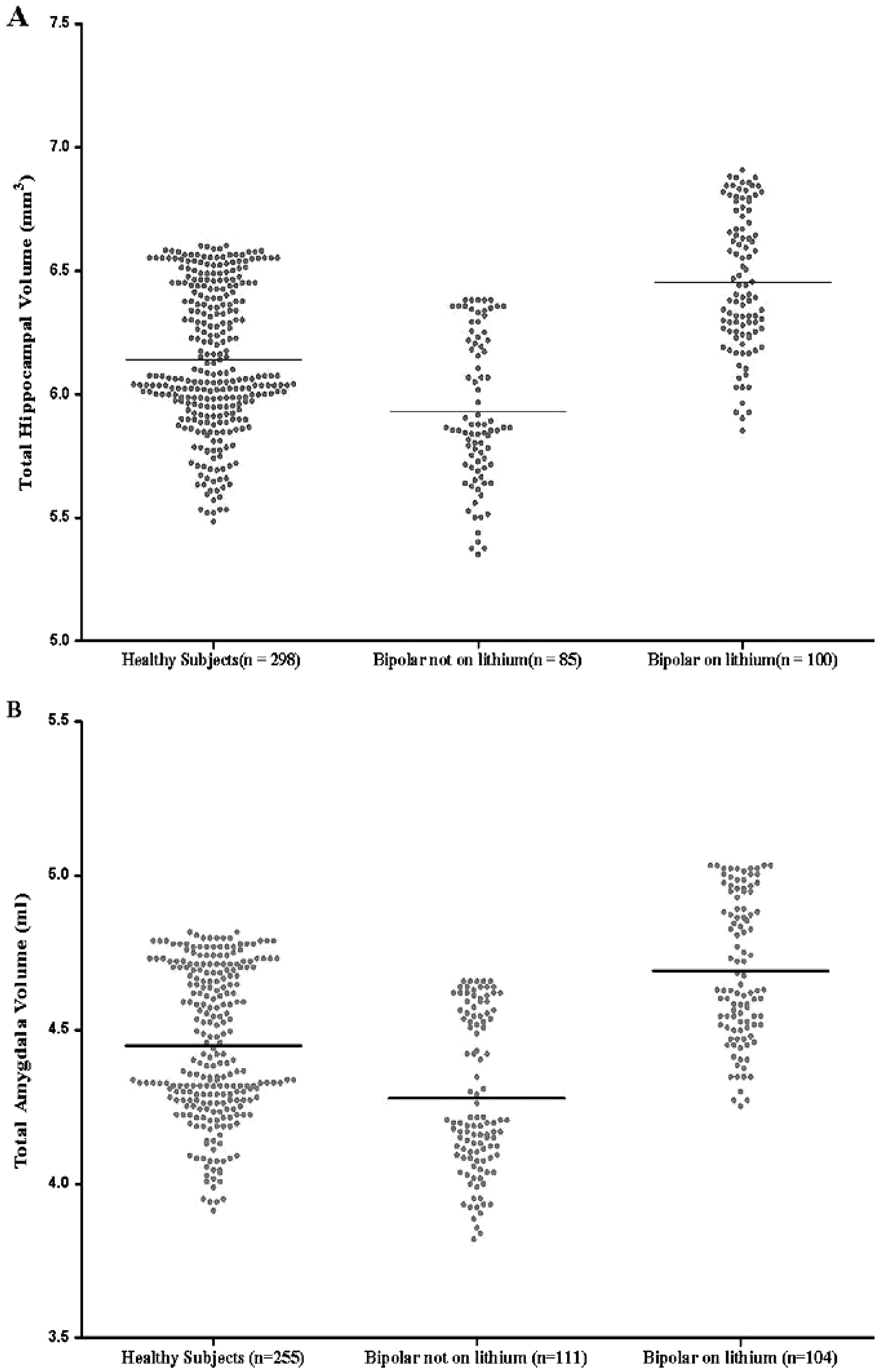
p < .001) than both those patients not treated with lithium and healthy subjects. In Figure S1 in Supplement 1, we present a plot of hippocampal volume and amygdala volume versus age paneled by research center, and in
Figure 1, we present a plot of predicted hippocampal volume and amygdala volume (from the linear mixed model) by the different levels of lithium factor (bipolar individuals taking lithium, bipolar individuals not taking lithium, and healthy subjects), while adjusting for gender, research center, and age. Global cerebral volume was also significantly different across subject groups (
p = .003), with bipolar subjects not taking lithium having a smaller mean volume compared with both healthy subjects and bipolar subjects taking lithium. Bipolar individuals regardless of lithium use had larger total (
p = .003) and left (
p = .0001) temporal lobe volume compared with healthy subjects, although only left temporal lobe volume remained significantly increased in volume after correcting for multiple testing.
Brain volume and other medications
No association was found for individuals with bipolar disorder prescribed valproate or carbamazepine alone at the time of scanning and any regional brain volume compared with individuals not taking these medications. Similarly, there was no difference in any regional brain volume in those patients taking antipsychotic medication compared with those not taking antipsychotic medication. As we only had data for 20 individuals on typical antipsychotic agents and 31 individuals on atypical antipsychotic agents for any brain region, we considered this too small a subset to carry out analysis comparing these individuals to healthy subjects or to each other.
Brain volume and clinical variables
We found an association between reduced mean cerebral volume (B = −4.064%, 95% CI −7.460, −.668; p = .019) and longer duration of illness in bipolar patients with research center, gender, age, and lithium treatment in our regression model. No other brain region demonstrated a significant positive or negative association with illness duration and no association was demonstrated between the number of hospitalizations and any regional brain volume. We similarly examined age of onset and regional brain volumes and found that an earlier age of onset of bipolar disorder was associated with reduced mean cerebral volume (B = 3.615%, 95% CI .304, 6.927; p = .033) and left thalamic volume (B = .054%, 95% CI. 004, .104; p = .035) and increased total (B = −.024%, 95% CI −.046, −.001; p = .039) and left amygdala volume (B = −.014%, 95% CI = −.025, −.002; p = .020). There were no significant two-way interactions identified between age and gender and any regional brain volume.
First episode and psychosis
We only had data from three or more research centers for cerebral (n = 48, six research centers) and amygdala volume (n = 47, six research centers) in relation to individuals with bipolar disorder in their first episode of illness. Cerebral volume (F = 5.731, p = .017) and total (F = 12.162, p = .001), left (F = 6.695, p = .010), and right amygdala volume (F = 14.552, p = .0002) were reduced in volume in first episode bipolar subjects compared with healthy comparison subjects. When we compared these brain regions for individuals in their first-episode bipolar disorder to those who had multiple episodes, we found no difference in cerebral volume (F = .170, p = .680) or total (F = .650, p = .421), left (F = .728, p = .395), and right amygdala volume (F = .471, p = .493). We only had sufficient data to examine the effect of psychosis for cerebral volume (n = 83, three research centers), and no difference was found between bipolar individuals who had or did not have psychosis (F = .011, p = .916).
MRI field strength
Two research sites used MRI field strengths other than 1.5 T and analyzed cerebral hemisphere and temporal lobe volume. When we excluded these research sites from our analysis, no significant differences were noted from our original findings, with increased total temporal lobe (F = 12.029, p = .001), left temporal lobe (F = 19.654, .00001), and right temporal lobe volume (F = 4.394, p = .037) in bipolar individuals but no difference in mean cerebral hemisphere volume between bipolar individuals and control subjects noted. Global cerebral volume remained significantly different across subject groups (F = 7.534, p = .001), with bipolar subjects not taking lithium having a smaller mean volume compared with both healthy subjects and bipolar subjects taking lithium.
Discussion
Similar to meta-analyses of aggregate data (
13–
15), we found that bipolar I disorder is associated with increased right lateral ventricular volume, which suggests a subtle anatomical laterality difference in pathogenesis compared with schizophrenia, where left-sided ventriculomegaly is more prominent (
45). Our findings comparing the entire bipolar group with healthy subjects are also consistent with previous meta-analyses that found a preservation of global cerebral volume and hippocampal volume in bipolar disorder (
13,
14), although a recent meta-analysis noted a global reduction in brain volume (
15). However, the present study provides strong evidence for a substantial contribution of lithium treatment to medial temporal lobe enlargement in patients with bipolar disorder and reveals this phenomenon as a potential source of heterogeneity in published magnetic resonance bipolar studies. The apparent trophic effect of lithium was present across research centers and age and was anatomically specific, most prominently evident in the neuroplastic hippocampus and the amygdala. No such lithium effect was detected for anterior cingulate, lateral ventricular, thalamic, basal ganglia, or temporal lobe volume.
First-episode bipolar disorder patients had reduced cerebral volume and amygdala volume and individuals with bipolar disorder who were not taking lithium had reduction in cerebral and hippocampal volumes compared with healthy comparison subjects—findings consistently reported in the related syndromes of unipolar depression and schizophrenia (
45–
49). This finding raises the intriguing possibility that bipolar disorder may indeed share with schizophrenia and depression the pathogenetic mechanisms associated with medial temporal lobe volume reduction, perhaps induced by glucocorticoid excess (
50,
51), but that these changes are reversed in patients with bipolar disorder alone by the differential use of lithium in this patient group.
Our finding of increased hippocampal volume in individuals treated with lithium compared with those bipolar individuals not treated with lithium (and healthy subjects) is consistent with some other cross-sectional studies not included in the mega-analysis (
21–
23,
52,
53) and two recent longitudinal studies of 1 to 8 weeks and 2 to 4 years duration (
43,
54). Although the mechanism of action of lithium is poorly understood (
55), an important role in neuroprotection and neurogenesis has been suggested (
56,
57). The hippocampus is a particularly plastic brain region (
58) and is one of the few areas to produce neurons postnatally (
59); therefore, it may be more likely than other brain regions to be affected by medication induced neurogenesis (
60). The mechanism of lithium-induced neurogenesis has not been fully elucidated; however, proposed mechanisms include an effect on signal pathways including its ability to upregulate the cytoprotective protein Bcl-2 (
58,
60) and its effect on growth factors including nerve growth factor (
57) and brain-derived neurotrophic factor (
57,
61,
62). Our finding of increased amygdala volume in individuals treated with lithium is consistent with the findings from another recent study (
21) and suggests that the amygdala may also be modified by lithium. Interestingly, these structures are closely interconnected and form part of the anterior limbic system known to be involved in mood regulation and that demonstrate task-related hyperactivity in functional imaging studies of bipolar disorder, possibly related to impaired prefrontal modulation of these regions (
63,
64). In contrast, there was no apparent effect of lithium on striatum, temporal lobes, or lateral ventricular volumes. However, almost all patients in the sample were taking medications and it may well be that alternative mood stabilizing agents had differential effects on other brain volumes. For example, taking lithium or any other mood stabilizer could be related to the temporal lobe and putamen volume increase identified in the present study, as there were insufficient psychotropic naive patients in the sample to assess this. The inclusion of medication-free patients with bipolar disorder and careful longitudinal studies assessing homogenous samples of patients on different medications will be required to elucidate such propositions.
There are some other limitations to this study. It was only possible to acquire individual data from 11 of the 22 research groups identified who satisfied our inclusion and exclusion criteria. Due to this, we were unable to examine anterior cingulate gyrus and intracranial volume between treatment groups. Not all research sites had acquired data on sociodemographic or clinical variables of interest such as socioeconomic class, medication use (two sites did not supply data in relation to medication use; however, these two sites contributed the fewest individuals to the mega-analysis and did not analyze the amygdala or hippocampus), treatment adherence, severity of depression or mania at time of scanning (most individuals were euthymic), and psychotic symptoms. All research sites did, however, supply data in relation to subjects' age, gender, and illness duration. We did not have sufficient data to analyze the duration of medication exposure or medication levels and regional brain volumes. We were also unable to control for intracranial or cerebral volume in our analysis of brain subregions, as not all research groups had acquired these data. We did not have sufficient data to examine if a history of psychosis significantly affected regional brain volumes in bipolar disorder. The different MRI datasets analyzed used different MRI field strengths and pulse sequences and different techniques to delineate anatomical brain regions. While mega-analysis has the advantage of being specifically able to control for research center and thus control for differences in MRI techniques between research centers, it would, of course, be preferable if identical techniques were used by each research center.
Our finding of increased amygdala volume in individuals with bipolar disorder treated with lithium may help to explain some of the inconsistencies in the published literature. Previous studies demonstrating increased amygdala volume in individuals with bipolar disorder have predominantly included individuals treated with lithium (71% and 63%) (
5,
6), whereas studies demonstrating a reduction in amygdala volume included fewer individuals treated with lithium (20%–40%) (
8–
11).
We noted increased temporal lobe volume in individuals with bipolar disorder, with left temporal lobe volume increased in bipolar individuals both on and off lithium. Although this is not a well documented finding, three of the five studies included in our analysis had nonsignificant increases in temporal lobe volume in bipolar individuals compared with healthy subjects (
4–
6). Other studies have noted an increase in left temporal lobe volume (
65,
66). Wilke
et al. (
65) suggested that their finding of increased left temporal lobe volume was due to increased volume of the superior temporal gyrus, and an association between left temporal lobe volume and increasing duration of illness has been reported (
66).
While we had fairly modest power in relation to the putamen, we detected an increased volume of this region in individuals with bipolar disorder, which is consistent with some (
3,
7,
37) but not all previous findings (
26,
67,
68). This increased volume was only noted for the right putamen and may reflect previous findings where shape differences (increased radii) in the right putamen but not left side were noted in drug-naive bipolar subjects compared with control subjects (
69).
Our finding of a reduction in cerebral volume with duration of illness is consistent with a number of studies that have demonstrated reduced total gray matter volume with illness duration in bipolar disorder (
69–
72) and suggests that a neurodegenerative process may be involved in the pathophysiology of bipolar disorder. Further prospective longitudinal studies are necessary to comprehensively elucidate this proposition.
In this study, we demonstrated that adults with established bipolar I disorder display right lateral ventricle enlargement and increased mean left temporal lobe and right putamen volume. The main source of heterogeneity identified by this large individual level analysis of clinical and demographic factors was medication usage. Lithium treatment was differentially associated with a regionally specific increased mean volume of the hippocampus and amygdala. This increased mean brain volume associated with lithium may be due to the neuroprotective effects of lithium, which are possibly mediated by its effect on neurotrophic growth factors.