Structural neuroimaging is becoming increasingly important for neuropsychiatry.
2,3 However, it is not uncommon for patients to present with neuropsychiatric symptoms consistent with brain pathology yet without clearly identifiable lesions on either computed tomographic (CT) or magnetic resonance (MR) structural images. There are no reliable estimates of how frequently this apparent absence of lesions in the presence of symptoms is likely to occur. Stroke may be missed (false negative) in 5% to 30% of cases.
4–6 A study of primary progressive aphasia found CT was normal in 50% and MR in 17% of the cases.
7 Similarly, systemic lupus erythematosus may present with extensive neuropsychiatric symptoms but without MR-visible abnormalities.
8 It has been suggested that many types of pathology may be difficult to visualize because they are small or diffuse in nature.
9Adding a method of
functional neuroimaging to the clinical examination may provide a way to identify such abnormalities. A recent study at a neuropsychiatric tertiary referral center found that 40% of the study population had normal MR or CT studies. Most of these (77% of patients with normal structural neuroimaging) had abnormal cerebral blood flow (CBF) images.
10 Even when structural brain imaging shows lesions are present, functional neuroimaging may provide a better assessment of brain dysfunction. Changes in cognitive symptoms closely correlated with changes on functional neuroimaging (CBF and cerebral glucose uptake), but not necessarily with structural neuroimaging, in recent studies of vascular dementia.
11,12 Thus, functional neuroimaging may provide useful information for clinical management.
Until recently, functional neuroimaging techniques were available only in a research-oriented environment and were quite expensive to perform. Now, with the maturation of xenon-enhanced computed tomography (Xe/CT), the imaging of CBF has the potential to become widely available and may become a valuable diagnostic tool. Xe/CT is based on the use of stable xenon gas as an inhaled contrast agent for CT imaging, possible because it is radiodense and lipid-soluble. When inhaled, it dissolves into the blood and passes into the brain parenchyma. The patient inhales a mixture of xenon (usually 26%–33%) and oxygen for several minutes via a face mask. CT scans are acquired prior to inhalation (providing a baseline) and during this inhalation time (a “wash-in” study). More scans may be acquired following inhalation, as well (a “wash-in/washout” study). Standard CT scanners can acquire three to four brain slices per Xe/CT study. The new spiral CT systems, which are rapidly replacing the standard scanners, can acquire eight to ten slices. This is sufficient for reasonable coverage of the brain. Several sets of scans are acquired at each brain level, allowing calculation of a xenon arrival curve for each pixel of each slice. This information, along with the concentration of xenon in the expired air (an indirect measure of arterial concentration), is required to calculate CBF for each pixel.
13–15Initial Xe/CT studies were limited by the side effects of xenon gas and the time required to acquire and compute the CBF images. Advances in technology have brought the time to compute the images down from hours to seconds. Xenon is a narcotic gas, more potent than nitrous oxide. Inhalation of 71% xenon is sufficient for anesthetic effect in 50% of patients. Present studies use much lower doses than this, as noted above, but some euphoric or dysphoric side effects are seen (which may cause a temporary exacerbation of neuropsychiatric symptoms), as is somnolence. Mild nausea can also occur; thus the patient must take nothing by mouth for 4 hours prior to scanning to reduce the risks of emesis and aspiration. Very rarely, patients experience apnea, reversible by an instruction to breathe. Like other narcotic gases, xenon also causes mild cerebral vasodilation. Overall, approximately 10% of patients experience unpleasant side effects, all of them transient.
15–17As with any imaging examination, the patient must remain still. In some cases sedation will be required to achieve this. Bone artifacts, which impair CT imaging of areas very near bone, can be reduced by correct angulation of the patient's head.
There are several advantages of this technique over other methods of imaging CBF. Stable xenon gas is not radioactive, so the only radiation exposure is that required for the CT scan itself. This means radiation exposure is limited to the most radiation-resistant areas of the body. With other methods, a radioactive tracer is injected, so the entire body is exposed. The image resolution is good, and there is direct anatomic correlation with the baseline CT scan. The study can be repeated in 15 minutes, after xenon gas is eliminated from the body by breathing room air. Thus, it is possible to perform sequential studies with the patient in different states (i.e., after administration of a drug challenge). It is important also to note that the technique is inexpensive (the additional cost per study is less than $100), fast (it adds only 10 to 15 minutes to a routine CT exam), and a billable procedure when considered medically necessary.
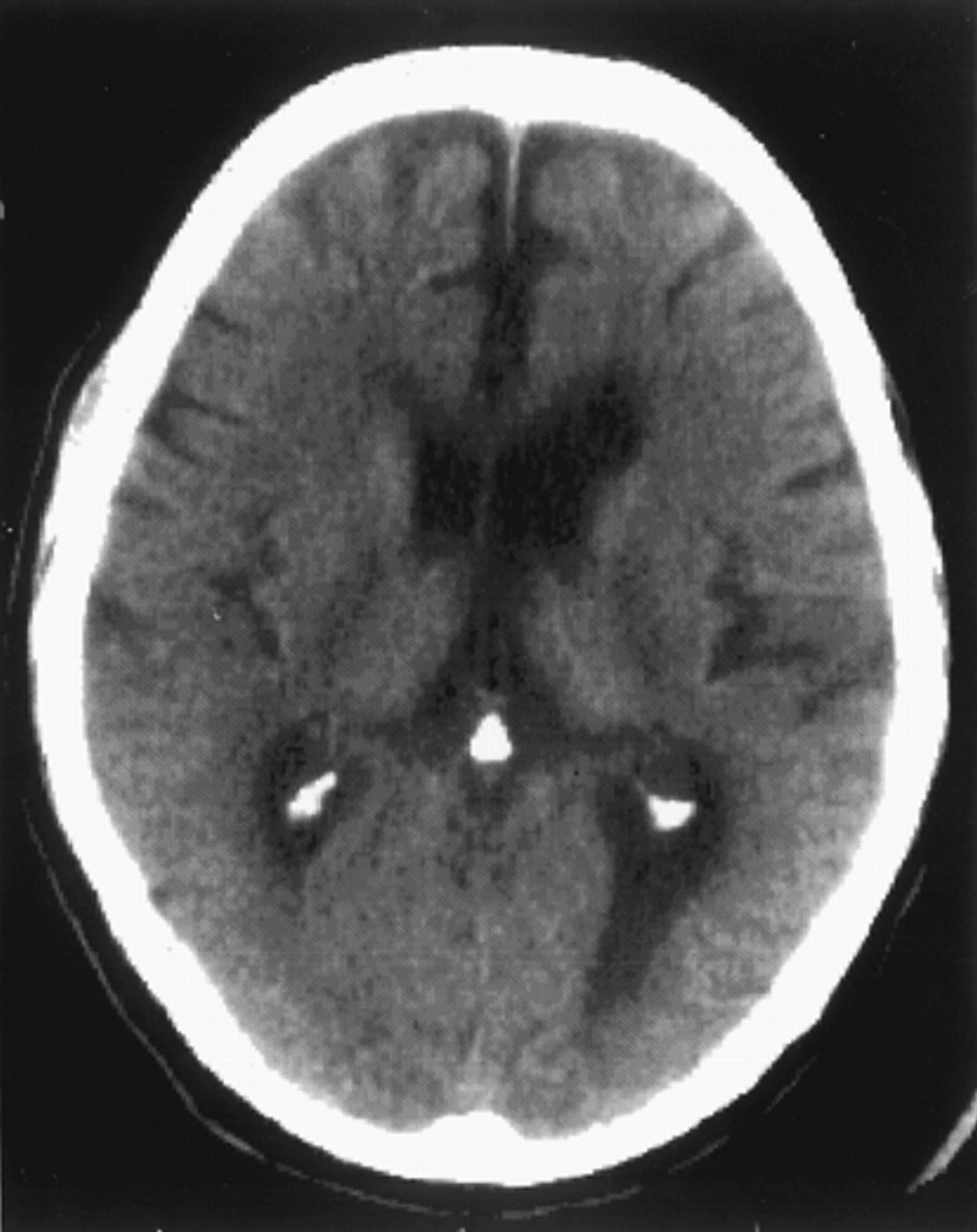
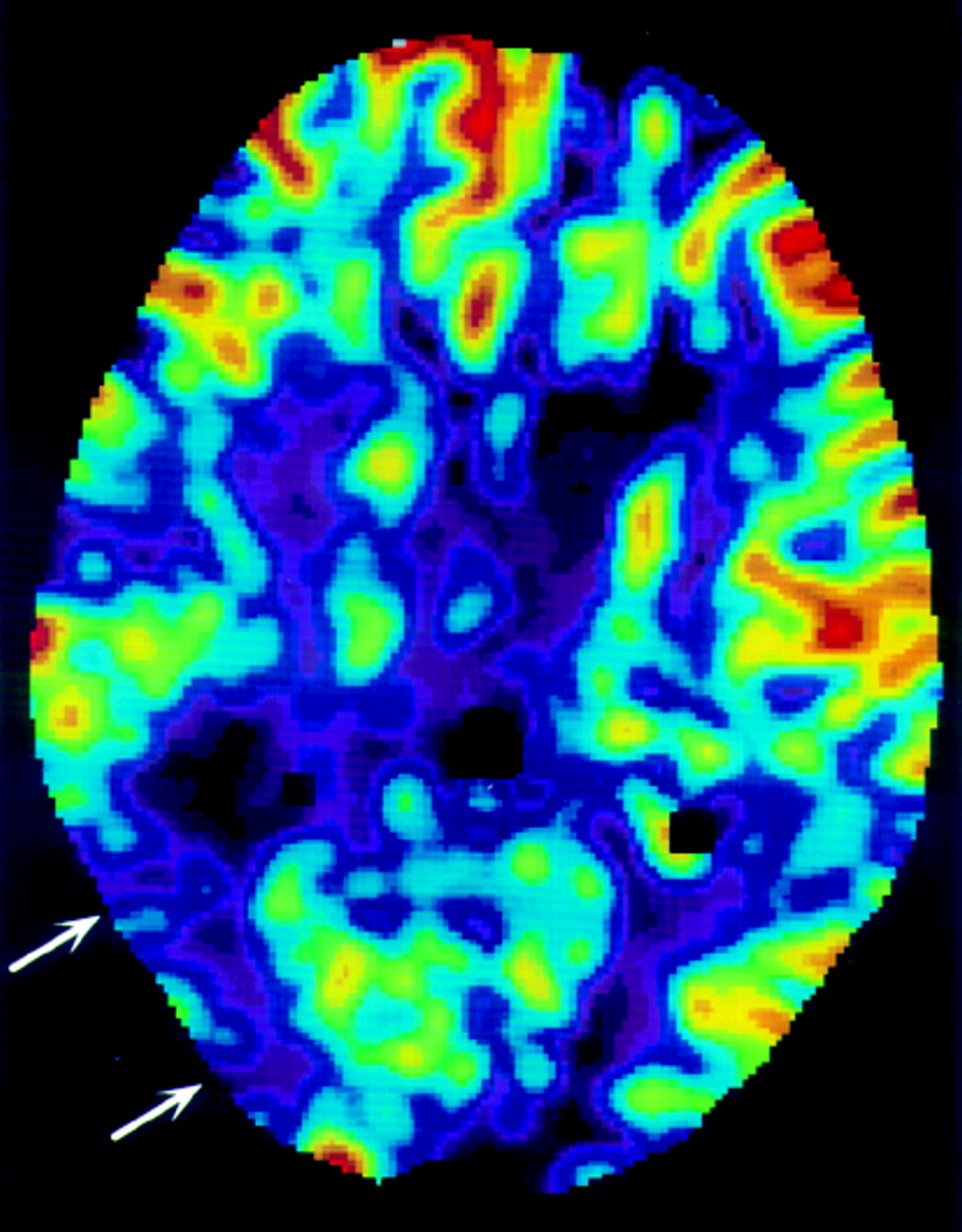
15,18In the case presented here, the patient failed to respond to therapy based on working diagnoses of Alzheimer's disease and major depression. Neuropsychological testing was done, leading to the suspicion of cerebrovascular disease or stroke with bilateral hemispheric involvement. Neither CT nor MR imaging of the brain could explain the clinical deficits. The finding of decreased CBF on the Xe/CT examination was consistent with a cerebrovascular accident (CVA). As a result of this finding, the diagnoses changed from probable Alzheimer's disease and major depression to dementia secondary to CVA. The psychiatric day treatment program and donepezil administration were discontinued. Patient and family education focusing on poststroke management was initiated. In a study by Velakoulis and Lloyd,
10 the functional imaging finding of altered CBF changed the clinical management in almost 10% of the patients. Thus, availability of CBF imaging can have an impact on clinical management in a significant number of patients presenting with neuropsychiatric symptoms.