Retrospective Studies With Autopsy-Proven DLB
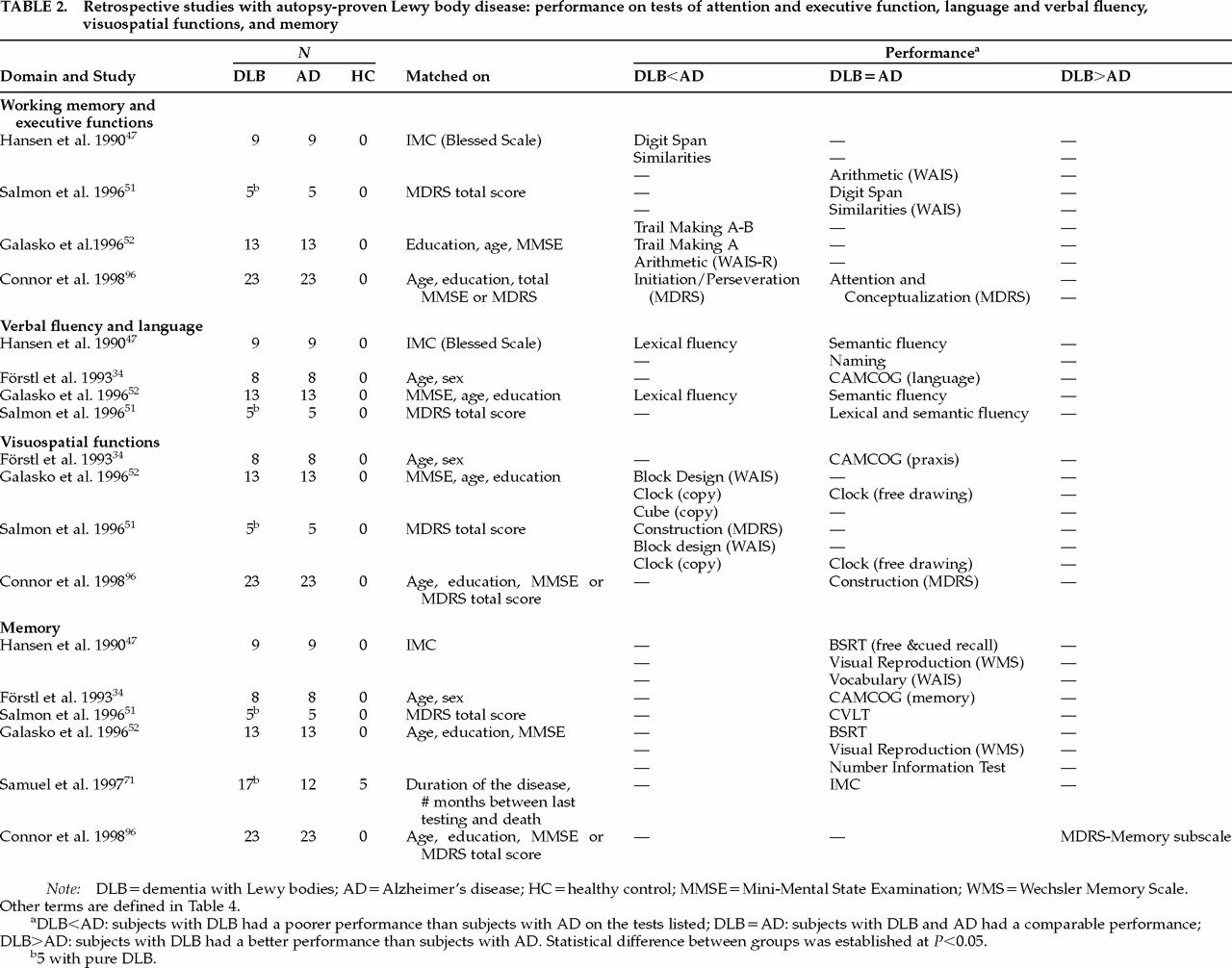
Six retrospective studies, with cross-sectional data, have compared small groups of subjects (mean number of DLB subjects per group=12.51, range 5–23; mean number of AD subjects per group=11.51, range 5–23) using different matching procedures: the Information-Memory-Concentration subtest score of the Blessed scale;
93 the MMSE
94 or Mattis Dementia Rating scale (MDRS)
95 total score, alone or in combination with age, gender, and education; the duration of the disease; and the number of months between last testing and death (see
Table 2).
34,47,51,52,71,96 These subjects were mildly
51,96 to moderately
47,52 demented. In two studies, the subjects with Lewy Body Variant (or DLB) and AD were severely demented,
34,71 whereas the 5 subjects of Samuel et al.,
71 with pure DLB, were moderately demented. Only one study included a healthy control group (of 5 subjects).
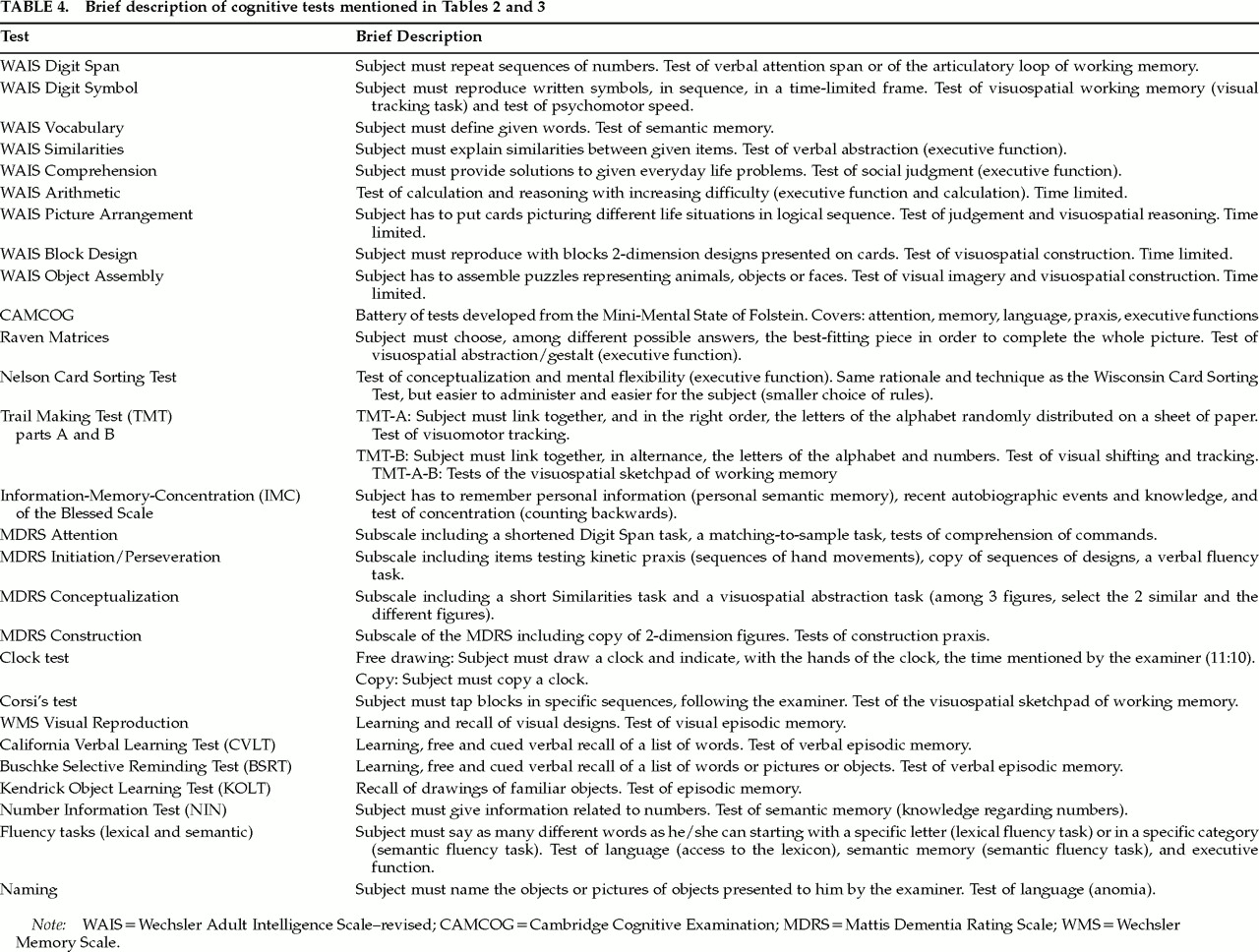
71Table 2 (tests described in
Table 4) indicates that mildly and moderately demented patients with DLB perform more poorly than patients with AD on tests of visual tracking (Trail Making Test A) and visual attention shifting (Trail Making Test B)
51,52 that rely on working memory (WM).
97,98 Working memory is the system necessary for holding and manipulating information while performing various tasks including learning, reasoning, and comprehending. The central executive system (CES) is the supra component of this model. It is assumed to be an attention controller and to have, among other roles, that of coordinating and distributing attention resources between the two slave subsystems of WM. The visuospatial sketchpad is the slave subsystem that maintains information under a visuospatial code. The other slave subsystem, the articulatory loop, maintains phonologically encoded material in primary memory through short-term storage and translates, when applicable, visually presented material into verbal material.
97,98 Regarding verbal attention (articulatory loop) capacities, two studies with mildly demented patients have reported that patients with DLB and AD were equally impaired in performance on the Digit Span subtest of the Wechsler Adult Intelligence Scale–revised (WAIS)
51 and on the Attention subtest of the MDRS.
96 Another study, with moderately demented subjects, described a poorer performance of patients with DLB when compared with AD subjects on the Digit Span task.
47 In respect to verbal and motor initiation capacities (
Table 2), mildly and moderately demented patients with DLB are more impaired than patients with AD.
47,52,96 The most sensitive tests in this regard have been the lexical fluency tasks
47,52 and the Initiation/Perseveration subtest of the MDRS.
96 One study
51 reported that subjects with DLB and AD perform equally poorly on the lexical fluency tasks. However, this study had a very small number of subjects per group, and they were matched on the MDRS scores.
51 The MDRS includes tasks of verbal fluency and tests of other frontal functions as well, thus potentially masking differences that might otherwise have been found. Performance in tasks of semantic fluency and knowledge (naming) were equally impaired in mildly, moderately, and severely demented DLB and AD patients.
34,47,51,52Regarding executive functions such as abstraction capacity (
Table 2), the performance of mildly demented subjects with DLB and AD is equally poor on the Conceptualization subtest of the MDRS and the Similarities subtest of the WAIS.
51,96 The performance of moderately demented patients with DLB is more impaired than that of patients with AD on the Similarities subtest of the WAIS.
47 The two studies assessing moderately demented subjects reported different results on the Arithmetic subtest of the WAIS. According to Galasko et al.,
52 patients with DLB have a poorer performance than patients with AD on the Arithmetic subtest, whereas according to Hansen et al.,
47 these two groups perform equally poorly on the Arithmetic subtest. The subjects did not differ enough between the two studies in regard to demographics (education, age) and EPS features to account for the different results. These two studies
47,52 both included only a small number of subjects in each group (see
Table 2). They both performed several analyses on several variables, sometimes with nonparametric statistics (Mann-Whitney
U-test), but often with parametric statistics like analysis of variance and Student's
t-test, without any correction for the number of analyzed variables. Thus, some results could have been inappropriately identified as significant, or significant results might have been missed, because of the lack of statistical power.
Regarding visuospatial functions,
Table 2 shows that mildly and moderately demented patients with DLB perform more poorly than patients with AD on visuospatial praxis tests such as the Block Design subtest of the WAIS and drawing tasks such as the Clock.
51,52 Mildly and moderately demented patients with DLB have been found to be more severely impaired on the copy part of drawing tasks (Clock-copy and the Construction subtest of the MDRS), as opposed to the free drawing part, when compared with AD subjects.
51,52 However, some authors have described no difference between the two groups, in mildly and severely demented subjects, regarding visuospatial praxis capacities (drawing in two and three dimensions) and the copy part of these tasks (Cambridge Cognitive Examination [CAMCOG]-visuospatial praxis and the Construction subtest of the MDRS).
34,96 Connor et al.
96 and Salmon et al.
51 obtained different results on the Construction subtest of the MDRS (copy of two-dimensional designs). Both studies assessed mildly demented subjects. The DLB subjects of Connor et al.
96 had neuropathological changes associated with AD as well as cortical Lewy bodies, whereas the DLB subjects of Salmon et al. had only cortical Lewy bodies. Given also that subjects of Connor et al. had slightly inferior total scores on the MDRS to the subjects of Salmon et al., one would have expected to find more severe deficits in Connor and colleagues' DLB patients. However, it was not the case. The two patient groups of Connor et al. performed equally badly, whereas the DLB patients of Salmon et al. had a poorer performance than the AD patients. The samples of Connor et al.
96 (where the two groups performed equally) were larger than the ones of Salmon et al.
51 (where the DLB patients performed worse), and therefore the study of Connor et al.
96 had better power than the one of Salmon et al.
51Table 2 (last section) shows that most of the studies found performance on episodic and semantic memory tests to be equally impaired in subjects with DLB and AD with mild,
51,96 moderate,
47,52 and severe dementia.
34,71 The data have been collected with the Buschke Selective Reminding Test (SRT),
47,52 the California Verbal Learning Test (CVLT; episodic memory tests with free and cued recall paradigms),
51 the Visual Reproduction of the WMS (visual episodic memory test),
47,52 the Vocabulary subtest of the WAIS,
47 the Number Information Test (NIN; semantic memory tests),
52 the CAMCOG Memory subtest,
34 and the Information-Memory- Concentration subtest (IMC; attention, semantic and autobiographical memory) of the Blessed Scale.
71 However, some caution is in order regarding these findings. The results of Hansen et al.
47 might have been prone to masking effects, since the two groups of patients were matched for overall severity of dementia with a measure of memory (IMC of the Blessed Scale). Statistical analyses have not been applied to the data of Salmon et al.
51 collected with the CVLT, because the studied groups were too small (
n=5 subjects per group). Finally, in the study of Förstl et al.,
34 dementia as measured with the MMSE, was more severe in patients with AD (MMSE score=7.5±6.1) than in patients with DLB (9.8±6.7). Only one study, with mildly demented patients, has described better performance in subjects with DLB than in subjects with AD on the memory subscale of the MDRS.
96 Although this subscale gives some information on short-term free recall and forced-choice recognition capacities, it does not assess short- and long-term cued recall or long-term free recall and recognition capacities. These paradigms are crucial to differentiate between subcortical and cortical types of dementia, especially in the mild stage of dementia.
99,100 Unfortunately, Connor et al.
96 did not use other measures of memory.
Studies With Antemortem Clinical Criteria
Eight studies have compared relatively small groups of subjects (mean number of DLB subjects per group=12.6, range 7–26; mean number of AD subjects per group=18.5, range 10–52), using the following matching procedures: the MMSE total score, the Clinical Dementia Rating Scale (CDR),
101 or the CAMCOG global score,
102 in combination with age, gender, education, the duration of the disease, or the premorbid IQ.
56,83,103–107 These subjects were mildly
103–107 and moderately
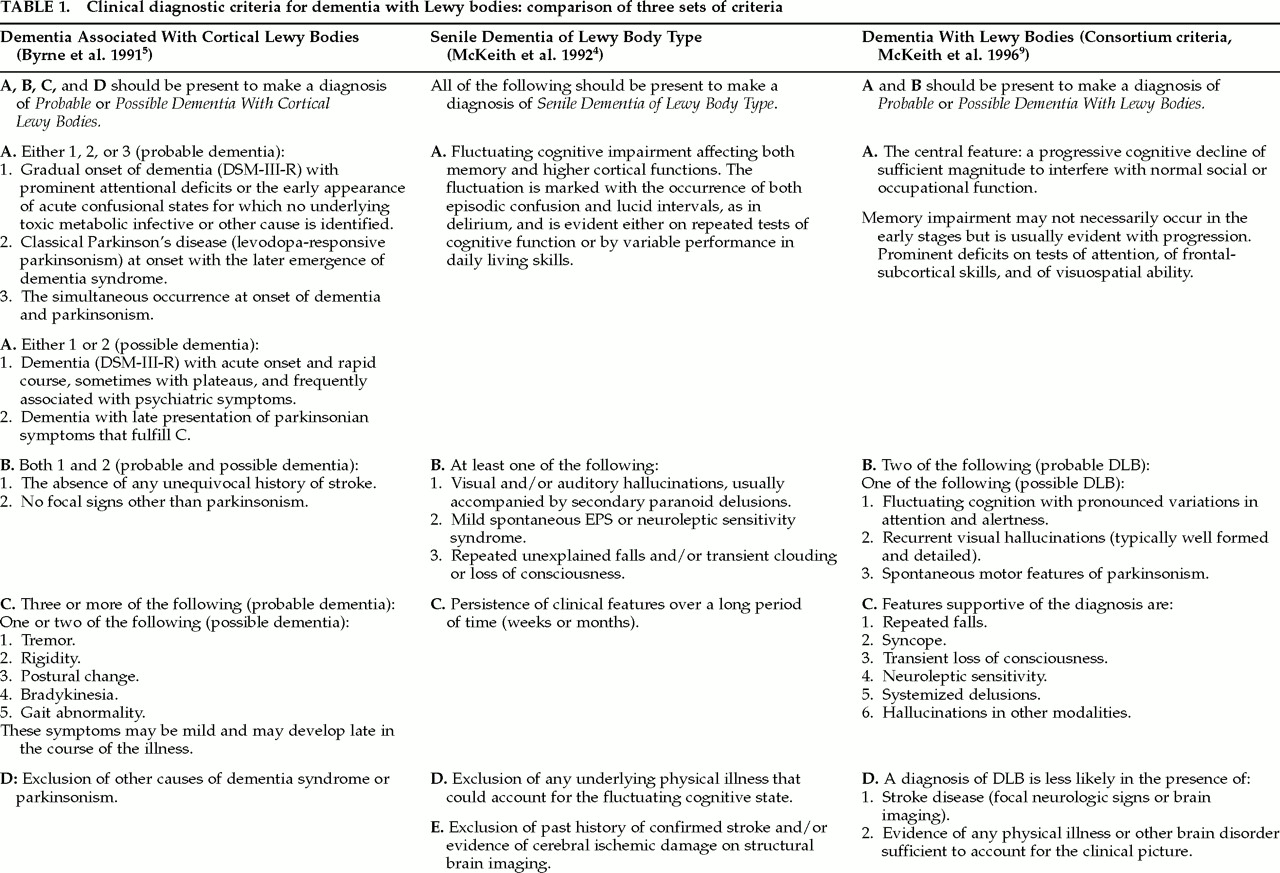
56,83,108,109 demented. No severely demented subjects have been assessed. Criteria for Senile Dementia of Lewy Body Type
4 have been used to enroll patients with DLB in 7 of 8 studies
83,103–108 (see
Tables 1 and
3). Gnanalingham et al.
83,108 also used the criteria of Byrne et al.
5 (see
Table 1)
4,5,9 for Cortical Lewy Bodies. Only Shimomura et al.
56 used the criteria for probable DLB per McKeith et al.
9 The NINCDS-ADRDA criteria for probable Alzheimer's disease have been used in order to include patients with AD in 8 of 8 studies.
56,83,103–108 Five studies also included a healthy control group, matched with the patients by age
106 and premorbid IQ,
103–105 and/or by education.
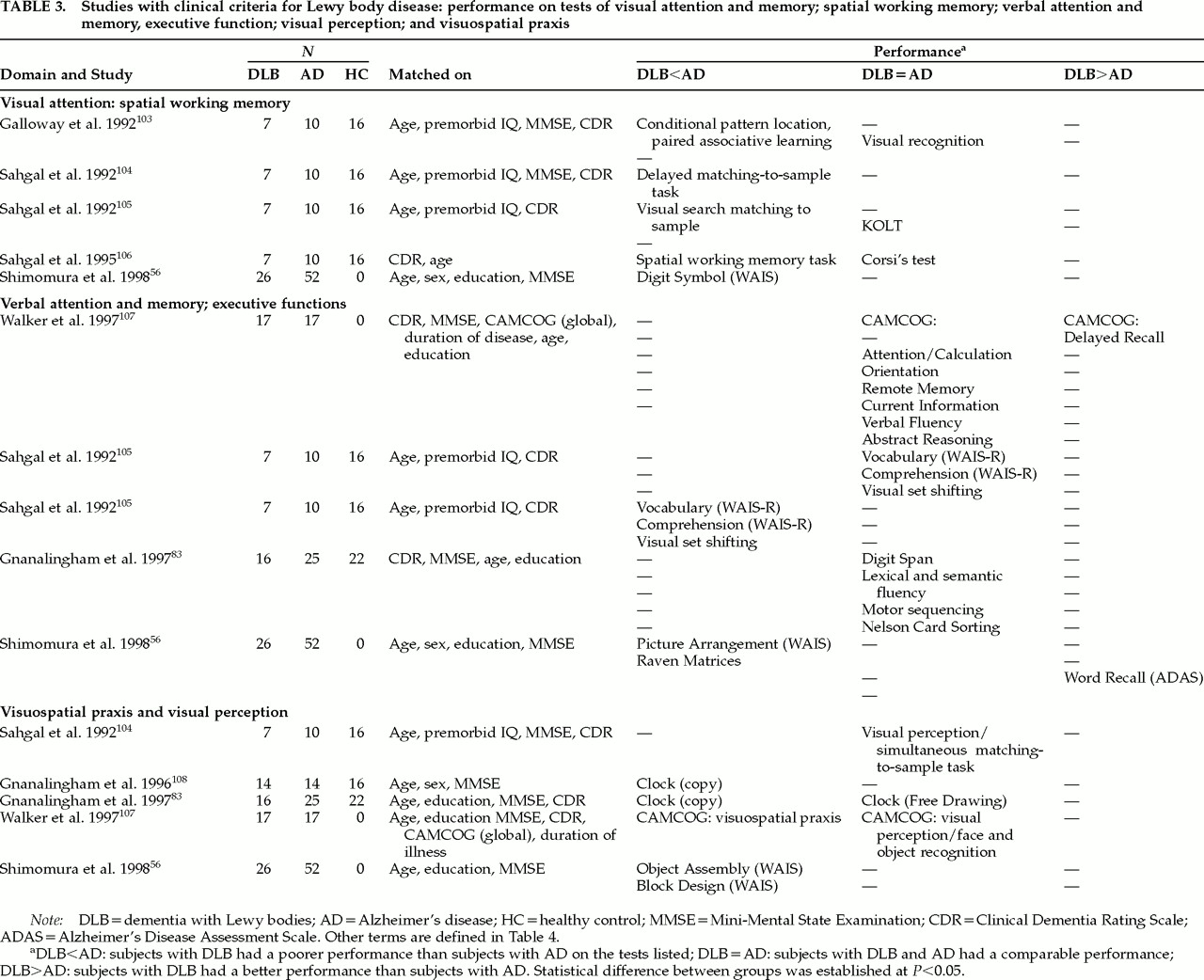
83,108Table 3 (tests described in
Table 4) shows that mildly
103–106 and moderately
56 demented patients with DLB are more impaired than patients with AD on some tests of visuospatial working memory
56,103–106 and are impaired to the same extent as AD patients on other tests of visual memory and attention. Galloway et al.
103 showed that mildly demented patients with DLB perform significantly worse than subjects with AD on the conditional pattern-location paired-associate learning task (spatial working memory). On a task with similar demands, the Digit Symbol subtest of the WAIS, moderately demented subjects with probable DLB performed more poorly than patients with AD.
56 However, the impairments of DLB and AD subjects on a visual recognition memory test (abstract designs) did not differ.
103 Sahgal et al.
104,105 have assessed visual attention, learning, and memory capacities of DLB and AD patients. They have reported worse deficits for patients with DLB on a delayed-matching-to-sample task
104 and on a visual search matching-to-sample task,
105 both relying on spatial working memory. Patients with DLB and AD performed equally badly on a semantic learning task, the Kendrick Object Learning Task (KOLT).
105 Sahgal et al.
106 have reported worse deficits in mildly demented DLB subjects compared with AD subjects on the spatial working memory task testing visuospatial planning abilities, one of the attributes of the central executive system in the working memory model.
97,98,110 This spatial working memory task has been previously described as very sensitive to frontal lobe impairment
111,112 as well as Parkinson's disease,
113–115 even in mild stages of PD,
114,115 and to frontal lobe impairment in patients with amygdalo-hippocampectomy.
112 However, the two patient groups of Sahgal et al.
106 performed equally poorly on the Corsi's block test, a visuospatial span task assessing the visuospatial sketchpad of working memory.
106 Regarding verbal attention and memory capacities (
Table 3, section 2), the results of three studies suggest that mildly and moderately demented patients with DLB are as impaired as patients with AD on some verbal attention and memory tests, but less impaired than AD subjects on some tasks of episodic memory. Mildly and moderately demented subjects with DLB and AD have been equally impaired on the Attention/Calculation subtest (counting backwards and serial subtractions) of the CAMCOG
107 and the Digit Span subtest of the WAIS.
83 Mildly demented subjects with DLB have been as impaired as AD subjects on tests of semantic and autobiographical memory such as the Vocabulary subtest of the WAIS
105 and the Orientation, Remote Memory (semantic memory), and Current Information (public episodic memory) subtests of the CAMCOG.
107 Mildly and moderately demented patients with AD have been more impaired than DLB patients on tests of verbal long-term free recall such as the CAMCOG delayed recall
107 and the word recall of the ADAS-COG.
56Regarding visuospatial praxis (
Table 3, last section), four studies have reported that patients with DLB are more impaired than patients with AD on various visuospatial tasks. Mildly demented patients with DLB have demonstrated poorer performance than patients with AD on the visuospatial praxis subtest (two- and three- dimensional drawing) of the CAMCOG.
107 Moderately demented patients with DLB have performed more poorly than both AD and PD patients on the Copy part of the Clock Test.
83,108 The two studies of Gnanalingham et al.
83,108 and a third study
109 (not included in Table 3 because it involved only one subject with DLB, compared to 64 subjects with AD) investigated the differential performance between the Copy (C) and Free Drawing (D) parts of the Clock Test. They found that patients with DLB also performed equally poorly on the Copy (C) and the Free Drawing (D) parts of the Clock Test, whereas patients with AD and PD performed more poorly on the D part than on the C part of the test.
83,108,109 However, the three patient groups in the study of Gnanalingham et al.
83 were not matched for severity of dementia. Patients with DLB and AD were moderately demented, whereas patients with PD, in the mild stage of dementia, were significantly less cognitively impaired, as measured with the MMSE. Gnanalingham et al.
108 have found a low sensitivity but a high predictive value for DLB with individuals presenting higher scores on the D part than on the C part. This finding has, however, been based on only 3 cases with DLB.
108,109 Moderately demented patients with DLB have also performed more poorly than patients with AD on the Object Assembly and Block Design subtests of the WAIS.
56 Regarding visual perception, two studies have shown no difference between mildly demented subjects with DLB and AD
104,107 on tasks depending on the functioning of the occipital and parietal lobes (object, design, and face recognition tasks).
Regarding executive functions (
Table 3, section 2), the only difference between patients with DLB and AD has been found in moderately demented patients, on tasks of visuospatial conceptualization and visuospatial judgment. The capacities of visuospatial conceptualization and judgment, as measured by the Raven Progressive Matrices and the Picture Arrangement subtest of the WAIS, have been more disrupted in moderately demented patients with DLB compared to patients with AD.
56 However, mildly and moderately demented patients with DLB and AD performed equally badly on two tasks of mental flexibility, a test of visual set-shifting,
105 and the Nelson Card Sorting Task.
83 Nevertheless, subjects with DLB and AD were more impaired than PD and control subjects on the Nelson test.
83The capacities of verbal conceptualization and judgment, as measured by the Abstract Reasoning subtest of the CAMCOG
107 and the Comprehension subtest of the WAIS-R,
105 have not differed between mildly demented subjects with DLB and AD.
105,107 Other executive functions, such as the motor (motor sequencing task) and verbal (lexical and semantic fluency tasks) initiation capacities, have been equally impaired in mildly
107 and moderately
83 demented patients with DLB and AD.
Longitudinal Studies
Four of the six longitudinal studies assessed demented patients at the baseline evaluation by using a short cognitive test, the MMSE.
94 Another study used the short assessment CAMCOG, from the CAMDEX,
102 which is an elaborated version of the MMSE. Only one longitudinal study followed patients with an end diagnosis of DLB confirmed at autopsy.
116 Of the remaining five studies, only one
117 recruited patients with DLB by using criteria for DLB or SDLT.
4 Four studies enrolled patients with the diagnosis of AD with EPS and/or hallucinations.
118–121Twenty-four of the 81 AD patients followed by Miller et al.
118 had non–neuroleptic-induced extrapyramidal symptoms. Patients with EPS deteriorated 67% faster on the MMSE (4.5 points per year) than patients without EPS (2.7 points per year). All of the subjects were matched at baseline for age and MMSE total score (mean scores of 18 and 20).
118 Chui et al.
120 reported that 85 of 135 patients reached the individual end point of a 6- point decline on the MMSE. Among these 85 patients, 46 were mildly demented and 39 were moderately demented at baseline. Significant predictors of cognitive decline were hallucinations and agitation in the mild dementia group, and the presence of non–neuroleptic- induced EPS at baseline in the moderate group.
120 In another study, the EEG at baseline, but not the presence of hallucinations, was the best predictor of more rapid cognitive decline in moderately demented patients, as measured by the MMSE.
121 Nevertheless, hallucinations predicted a more rapid functional decline.
121Only one longitudinal study has given more information about the cognitive deterioration of subjects with AD and EPS compared with 1) subjects with AD lacking EPS and 2) subjects with PD and dementia.
119 At baseline, no significant difference on the formal neuropsychological testing was found between the three groups, with the exception that patients with AD (with and without EPS) had more false positive targets on the recognition paradigm of the word learning task compared with PD patients. After a year of follow-up, the difference between the AD and PD patients regarding the false positive targets remained the only significant distinction between AD (with and without EPS) and PD. Nevertheless, 14 subjects with AD+EPS had greater deficits on tests of verbal comprehension, automatic speech, semantic fluency, and praxis than 16 AD subjects without EPS.
119 This study presents a methodological problem of importance. The two groups of patients with AD were not properly matched at baseline, the subjects with AD+EPS being significantly more impaired at baseline than the group without EPS as measured on the Brief Cognitive Rating Scale of Reisberg et al.
122 The AD+EPS patients also tended to be more impaired at baseline than the group without EPS as measured on the Clinical Dementia Rating Scale (which showed that 57.14% of subjects with AD+EPS, versus 31.25% of AD subjects without EPS, were moderately demented).
Ballard et al.
117 followed, for one year, subjects with Alzheimer's disease, vascular dementia (VaD), and dementia with Lewy bodies, using, respectively, the NINCDS-ADRDA criteria for probable and possible AD,
74 the Hachinski scale for vascular dementia,
123 and the criteria for SDLT.
4 The total CAMCOG scores of the 116 moderately demented subjects with AD, VaD, and SDLT did not differ significantly at baseline, having respective means of 42.68, 44.50, and 47.67 (total possible score on the CAMCOG=106). Nevertheless, patients with DLB had a better performance than patients with AD on the recent memory subtest and a better performance than patients with VaD on the visual memory subtest. After one year, approximately 70% of the patients were reassessed. The 7 patients with DLB tended to deteriorate more rapidly on only the CAMCOG total score versus the 53 AD subjects and the 14 VaD subjects (mean deterioration=27±19.77, 13.21±12.61, and 13.29±13.48 points, respectively). However, a logistic regression analysis showed that patients with DLB deteriorated significantly more than patients with AD and VaD on the verbal (semantic) fluency subtest, and also more than patients with VaD on the Remote Memory subtest of the CAMCOG.
117 There was no significant difference among the three groups of patients on the other subtests of the CAMCOG: Orientation, Comprehension, Expression, Praxis, Recent Memory, Visual Memory, Attention and Calculation, Perception (Agnosia), and Abstract Thinking.
117More recently, Olichney et al.
116 reviewed the autopsied cases of 40 patients with Lewy body variant and 148 patients with Alzheimer's disease. The two groups of moderately demented patients were matched according to their age, education, and MMSE scores (mean MMSE scores: LBV, 18.2; AD, 17.8) at baseline. They found that LBV subjects had a rate of cognitive decline significantly more rapid and severe than the rate for AD subjects as measured by MMSE scores. The average rate of decline was –5.8±4.5 points per year in LBV compared with –4.1±3.0 points per year in AD (
t-test,
P<0.01). The LBV group declined a similar amount on the MMSE over a significantly shorter time interval than did the AD group (1.9 vs. 2.7 years;
P<0.005). The LBV patients presented significantly more parkinsonian signs at entry compared with AD patients (30% vs. 14%;
P=0.02). The patients with LBV had a shorter survival time from the onset of cognitive symptoms and a shorter mean survival after baseline.
116Summary and Discussion Related to the Cognitive Changes of DLB
In this review, 9 studies have assessed mildly demented patients,
51,96,103–107,118,120 11 studies have assessed moderately demented patients,
47,52,56,83,108,109,116,117,119–121 and 2 studies have assessed severely demented patients.
34,71 More than one-third (36.36%) of studies with moderately demented patients used comprehensive neuropsychological batteries, compared with 11.11% of the studies with mildly demented patients. The other studies used short assessments such as the MMSE,
34 the CAMCOG,
102 or the MDRS.
95 Nearly one-half of the studies (44.44%) with mildly demented patients specifically focused their cognitive assessment on tasks of spatial working memory. The 2 studies with severely demented patients used only short assessments. As a result, more cross-sectional and longitudinal information, regarding different aspects of cognition, is available in moderately demented subjects with DLB and AD than in mildly and severely demented subjects.
All of the longitudinal studies demonstrated a significantly
faster cognitive or functional decline in patients with DLB
116,117 or with AD plus EPS (or hallucinations/agitation)
118–121 over a period of 1,
116–119,121 2,
120 3,
119 or 8 years,
121 when compared with patients with AD. The MMSE has been sensitive enough to capture the more severe deterioration over time of subjects with DLB compared with subjects with AD. The MMSE is also sensitive to fluctuations in cognition over a 6-month period of time.
60 However, specific data regarding the cognitive profile of deterioration over time are lacking. The only specific longitudinal data available are coming from only two studies. Their findings will be summarized throughout this section.
This review has shown that the most consistently found cognitive deficit in mildly and moderately demented patients with DLB, compared with AD patients, is the impairment of
spatial working memory that relies on the
central executive system (CES) of working memory. Clinically, this impairment can be tested by using the computerized spatial working memory of Galloway, Sahgal, and co-workers
103–106 and also by using the Trail Making Test part B. This deficit has been reported in 5 antemortem and 2 retrospective studies. Spatial working memory tasks have been shown to be sensitive in mild and moderate Parkinson's disease without dementia
113,114 and in patients with amygdalo-hippocampectomy,
112 and to be dose-dependent on clozapine,
124 which acts as an adrenoceptor agonist. Because the pathological processes of DLB involve a dysfunction of the aminergic systems, as well as neuronal loss or abnormalities in the amygdala and hippocampus (see section above on pathological changes), comparisons between patients with DLB, AD, and PD on spatial working memory tasks will be necessary in the future.
An examination of the central executive system of working memory using the dual-task paradigm has not yet been done in subjects with DLB. The dual-task paradigm, one of the most widely recognized measures of the CES,
110,125–129 has been devised to measure the capacity of the CES to distribute attentional resources between a visual tracking task (visuospatial sketchpad) and a verbal rehearsing task (articulatory loop and phonological buffer). Subjects with AD, even in mild stages of the disease, have deficits on the dual task
110,125,127 and deteriorate on it,
125 whereas the single-task performance is maintained over time (over a period of 6 to 12 months). The dual task has been shown to be very sensitive in frontal patients with a dysexecutive syndrome, but not in frontal patients without a dysexecutive syndrome.
128,129 It has been hypothesized to rely on the cingulate and orbital frontal areas
130,131 and to depend at least on the integrity of the DA nigrostriatal and mesocorticolimbic systems,
126,132,133 and also, possibly, on the integrity of frontal cholinergic systems
134 in nondemented patients with PD. Given the pathological process involved in DLB (LB in anterior frontal and cingulate areas, neuronal loss in frontal lobes), the assessment of DLB subjects with the dual-task paradigm seems highly appropriate.
The impairment of the
visuospatial sketchpad, a subsystem of working memory, in mildly demented subjects with DLB needs further study. A retrospective study has found a more severe deficit (in DLB) on the TMT-A,
51 and an antemortem study has reported no difference between the performance of DLB and AD on Corsi's blocks test.
106 Two retrospective studies
51,96 and one antemortem study
83 have found that mildly demented patients with DLB were as impaired as patients with AD on tests of the articulatory loop of working memory (verbal attention). The impairment of verbal attention in moderately demented patients with DLB and AD needs to be investigated because two studies in these populations have obtained different results for verbal attention: one retrospective study described a poorer performance of DLB compared with AD patients,
47 whereas an antemortem study found no difference between the performance of the two patient groups.
83 In the present state of knowledge, the clinical assessment of the visuospatial sketchpad and the articulatory loop of working memory, using simple span tasks such as Corsi's blocks and the Digit Span task, would add nothing of real value to the process of differential diagnosis in the mild stage of dementia.
The second most important field where more severe deficits have been reported in subjects with DLB compared with AD has been the area of
visuospatial functions. Two antemortem studies and one retrospective study with moderately demented patients, and one retrospective study with mildly demented patients, found more severe impairment in DLB than in AD on the copy part of the Clock Test. Two retrospective studies assessing mildly demented patients had contradictory results: one described poorer performance of subjects with DLB,
51 whereas the other reported no difference between DLB and AD
96 on the Construction subtest of the MDRS. The free drawing part of the Clock Test has been used in two antemortem studies with mildly and moderately demented subjects with DLB and AD, and no difference between the two groups of patients has been found. Moderately demented patients with DLB were found to be more impaired than patients with AD in one retrospective and one antemortem study, using the Block Design subtest
52,56 and the Object Assembly subtest
56 of the WAIS.
Moderately demented patients with AD and EPS (possible DLB) have also deteriorated more rapidly on tests of
visuospatial and ideomotor praxis.
119 Mildly demented subjects with DLB have been reported to be more impaired than subjects with AD in a study using the Block Design subtest of the WAIS. A number of studies have used the Block Design and/or the Object Assembly subtest of the WAIS to compare the visuospatial capacities of patients with DLB and AD. However, the WAIS was not designed to be used with a neurological population.
135,136 In the standard administration and scoring of the Block Design and Object Assembly subtests, time to accomplish the task is as important as the correctness of the execution. The use of these tests with patients having EPS puts examiners at risk of measuring slowing that is actually due to rigidity and bradykinesia found in DLB.
80–83 Therefore, one would not know to what extent higher functions (depending on associative right parietal and bilateral occipital and frontal areas), such as mental rotation, planning, visuospatial organization, synthesis and perception, are involved in the impairment. On the praxis subtest of the CAMCOG, one antemortem study with mildly demented patients has found a more severe impairment in DLB compared with AD, whereas one retrospective study with severely demented patients with DLB and AD found no difference between the two patient groups. Despite the above- mentioned methodological problems, the use of some construction tasks without time limits, such as the Clock Test (especially the copy part), could be of some clinical diagnostic value.
Visual perception has been assessed in only 2 antemortem studies with mildly demented subjects; in each, the two patient groups were equally impaired on tasks of matching designs and object and facial recognition. Clinically, it seems likely that classic tasks of visual recognition (objects and faces) will not allow an early differential diagnosis between DLB and AD. The evolution, over time, of visual perception impairment in DLB remains unknown, as well as the involvement of visual perception impairment in the construction praxis deficits in moderately demented DLB patients. To clarify the visual perception issue, the performance of patients with DLB and AD should be studied, in longitudinal designs, on tasks of “pure” visuospatial perception such as the Benton Judgment Line Orientation Test that measure functions related to the integrity of the right parietal and bilateral occipital areas.
The results related to
verbal and motor initiation capacities are controversial. Three retrospective studies have found mildly and moderately demented patients with DLB to be more impaired than patients with AD on tests of lexical fluency or on the Initiation/Perseveration (verbal fluency, motor initiation and sequencing, serial drawing) subtest of the MDRS. However, one retrospective study with mildly demented patients
51 and one antemortem study with moderately demented patients
83 found that DLB and AD patients performed equally poorly on the lexical fluency tasks and the motor sequencing tasks. The performance on tasks of semantic fluency (category fluency) and knowledge (naming) was equally impaired in mildly, moderately, and severely demented subjects with DLB and AD in four retrospective and two antemortem studies. However, moderately demented patients with DLB deteriorated more than patients with AD (and VaD) on the semantic fluency tasks,
117,119 and also more than patients with VaD on the task of remote memory.
117,119 One study also found a more severe deterioration over time in speech and language capacities, such as comprehension and production of speech.
119 The problems with speech production in fluency and expression tasks can be due to the increased severity of EPS affecting the articulatory process, at the level of motor control, as well as to the deterioration of semantic knowledge and/or semantic access, under cognitive control. Unfortunately, none of the studies assessing verbal fluency and expression have controlled for the motor component of the task in order to isolate the nature of the problem. No study has correlated the EPS of DLB patients with their language performance. Clinically, verbal fluency tasks, and especially lexical fluency tasks such as the FAS, might be useful to detect DLB in the early stages of the disease. Semantic fluency tasks might be useful to follow the cognitive deterioration over time in DLB.
Regarding executive functions, one antemortem study has demonstrated a greater impairment in moderately demented DLB patients, compared with AD patients, on tasks of visuospatial abstraction and judgment. The capacity of verbal abstraction, principally assessed with the Similarities subtest of the WAIS, was found, in two retrospective and two antemortem studies, to be equally impaired in mildly demented patients with DLB and AD. However, moderately demented patients with DLB registered a poorer performance in verbal abstraction in one retrospective study. The mental flexibility capacity has been found to be equally impaired in mildly and moderately demented subjects with DLB and AD. Clinically, tests such as the Progressive Matrices of Raven, testing visuospatial abstraction, could be relevant in a process of differential diagnosis in moderate stages of dementia, patients with DLB being more impaired than patients with AD.
The functioning of episodic, semantic, and autobiographical
memory has been found to be equally impaired in mildly demented patients with DLB and AD in two retrospective and two antemortem studies. Four retrospective studies also reported the same degree of impairment in moderately and severely demented patients with DLB and AD. However, one antemortem study with mildly demented patients,
107 and another antemortem study with moderately demented patients,
56 found that DLB subjects had a better performance than AD subjects in tests of verbal episodic memory (delayed recall paradigm)
56,107 and personal semantic memory (name and address, in the CAMCOG).
107 Clinically, tests of episodic and semantic memory, such as the California Verbal Learning Test or Visual Reproduction on the Wechsler Memory Scale, will not distinguish patients with DLB from patients with AD because the performance of both populations will be equally impaired on most measures of these tests, with the exception of the free recall paradigm. Subjects with DLB might perform better on this paradigm than would be expected for patients with AD in the mild and moderate stages of dementia.