Subcortical Hyperintensity in Aging
Numerous MR imaging studies have demonstrated that aging is associated with an increased occurrence and severity of SH.
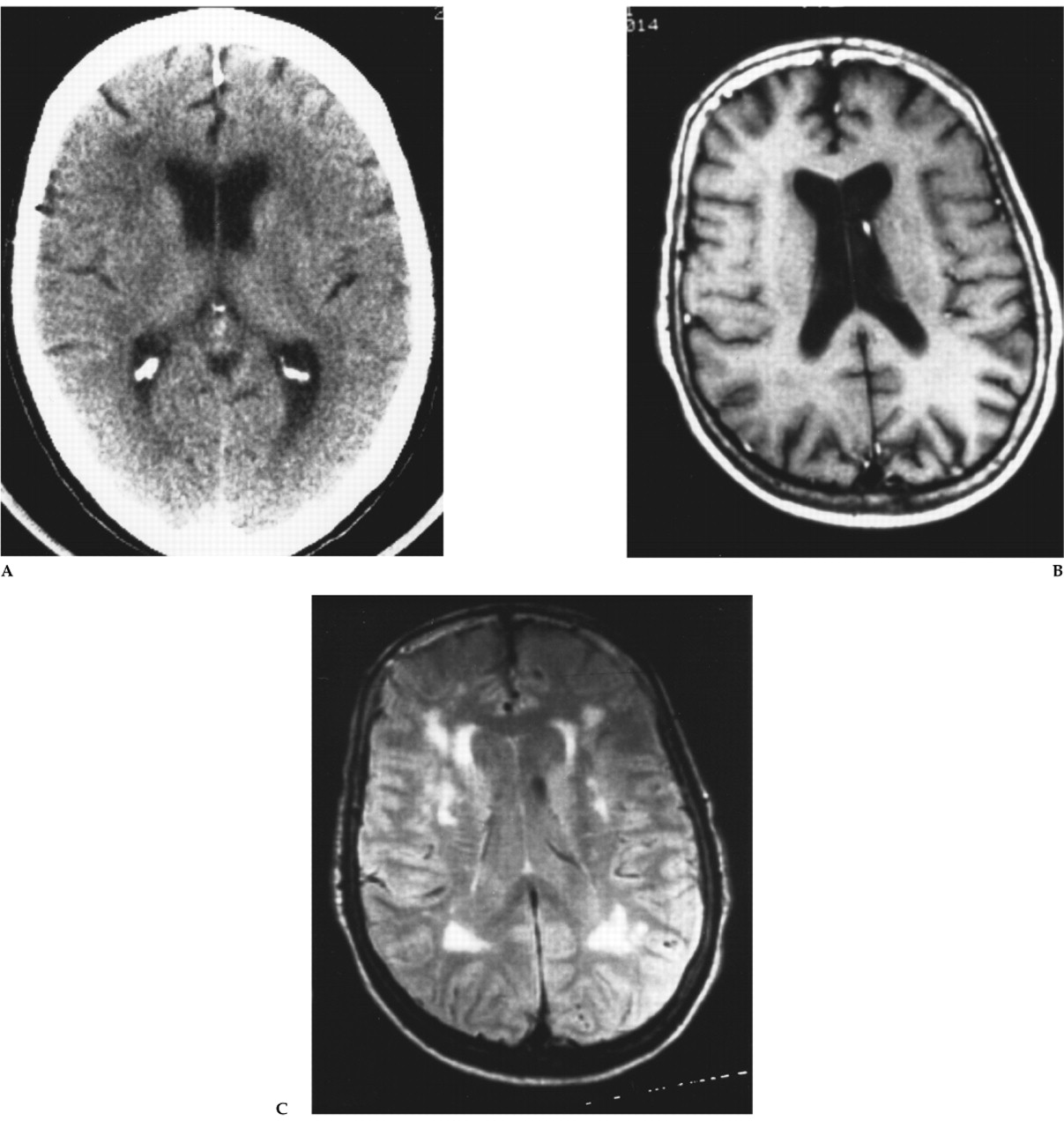
29–33 The precise frequency and distribution of SH in usual or normal aging are difficult to determine, however, given differences between studies in subject sample (age range, health status, etc.), imaging technology, and lesion definition and measurement. In our study of healthy adults with no lifetime history of neurologic or psychiatric illness, SH was present in the deep white matter in 48 subjects (64.0%), in the periventricular white matter in 9 (12.0%), in the basal ganglia in 9 (12.0%), in the thalamus in 4 (5.3%), and in the pons in 16 (21.3%).
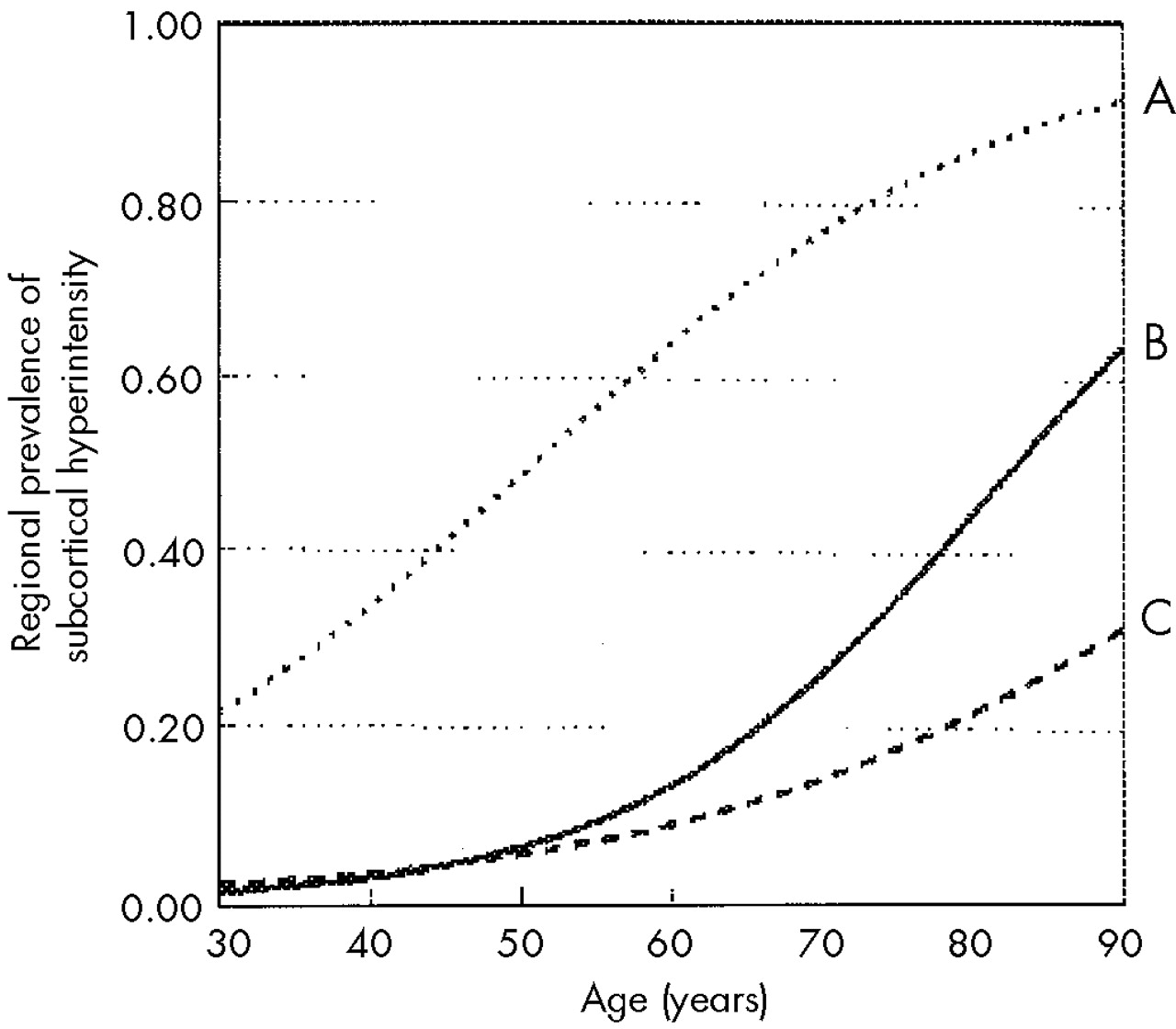
34 We found that the age-specific odds of subcortical hyperintensity increased by 5% to 9% per year of age, depending on the anatomical region involved (
Figure 3). The literature consistently demonstrates that patients with risk factors for vascular disease (e.g., smoking, diabetes mellitus, hypertension) and those with a high medical burden have a greater prevalence and severity of SH. Indeed, evidence on MR imaging of old cerebral “microbleeds” is reported in approximately 6% of neuropsychiatrically normal community volunteers and is associated with more extensive SH.
35 Recent data in twins suggest that genetic factors may also contribute to individual differences in volume of subcortical hyperintensity.
36Little is known about the natural history of SH in usual aging. Lesion progression has been documented in longitudinal imaging studies with follow-up of from 2 to 5 years.
37–39 In about half of the subjects the worsening was minor, whereas in the remainder more extensive changes were observed.
37 Reported risk factors for progression are diastolic hypertension and lesion severity.
37,38An emerging literature suggests that SH may have functional and clinical significance in normal elders. Quantitative EEG studies in normal aging show a relationship between SH and EEG abnormalities, most notably decreased coherence (a measure of shared electrical activity between brain regions) in the frontal and visual networks of connections.
40 In contrast, studies of evoked related potentials found no relationship between SH and P300 latency in normal elderly subjects.
41 Metabolic brain imaging studies have reported reductions in cerebral blood flow and metabolism among healthy elderly volunteers with relatively large volumes of SH.
42–44 These metabolic changes may be especially prominent in the frontal lobes,
42 where the SH lesions predominate. MR imaging has recently been used to examine the functional correlates of SH.
45 On MR spectroscopy, SH has been associated with a decreased ratio of adenosine triphosphate/inorganic phosphate, but not with any changes in phosphocreatine, phosphomonoester, or phosphodiester,
46 and with an increased ratio of choline/
N-acetyl aspartate (NAA), but not with any changes in creatine/NAA or lactate/NAA.
47Most of the research on the clinical significance of SH has focused on vascular events, equilibrium, and cognition. Given its presumed vascular etiology, it is not surprising that in patients with clinical vascular disease, SH is predictive of vascular events,
48 ischemic or hemorrhagic stroke,
49,50 and vascular death.
48 In patients with transient ischemic attack or minor stroke within the past 6 months, SH also predicts risk of hemorrhagic complications from oral anticoagulation with phenprocoumon.
50 Less is known about the impact of SH upon risk of overt cerebrovascular disease in normal elders.
Fibers essential for proper gait and balance course through the periventricular region. Several studies have found relationships between the extent of periventricular SH and impairment in equilibrium among elderly patients with complaints of disturbed balance
51–53 as well as in asymptomatic elderly volunteers.
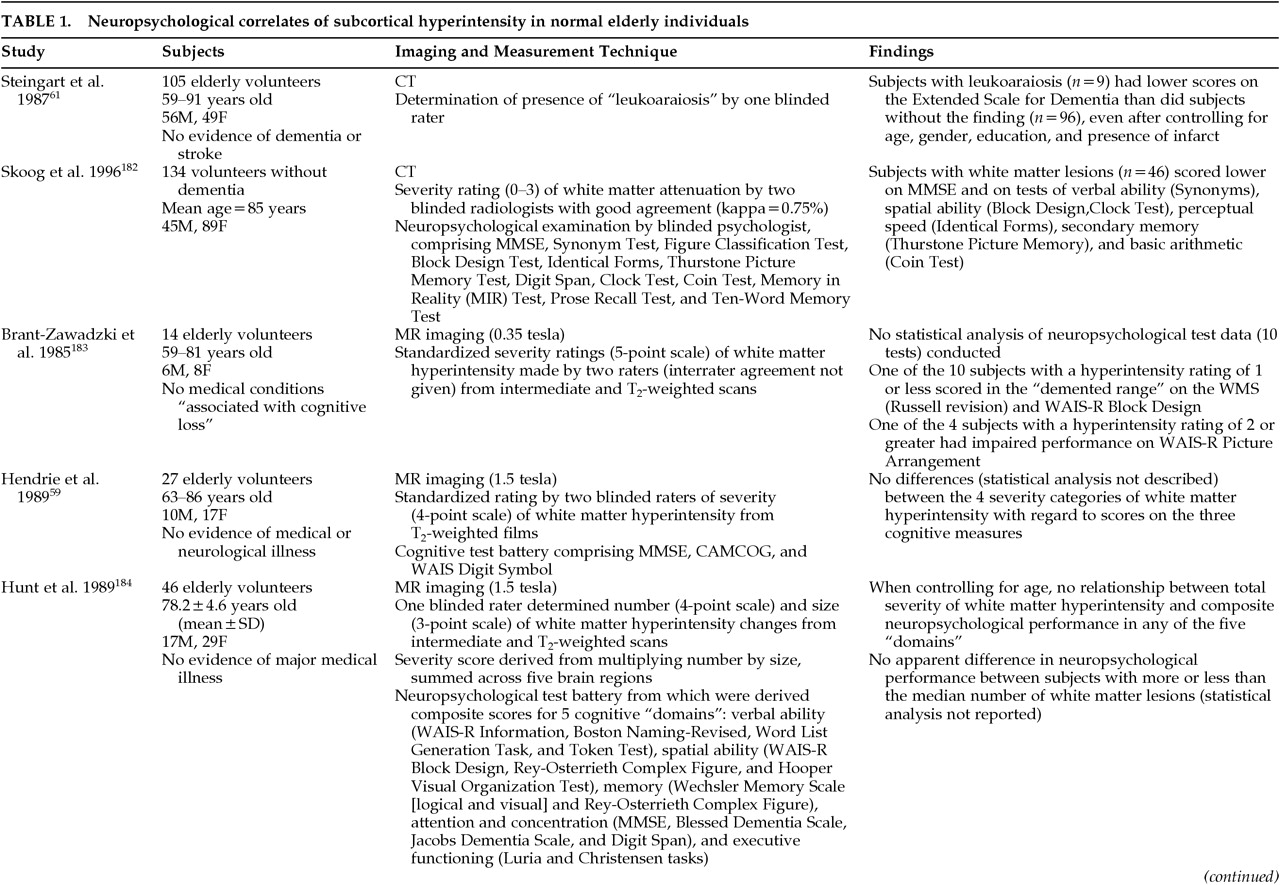
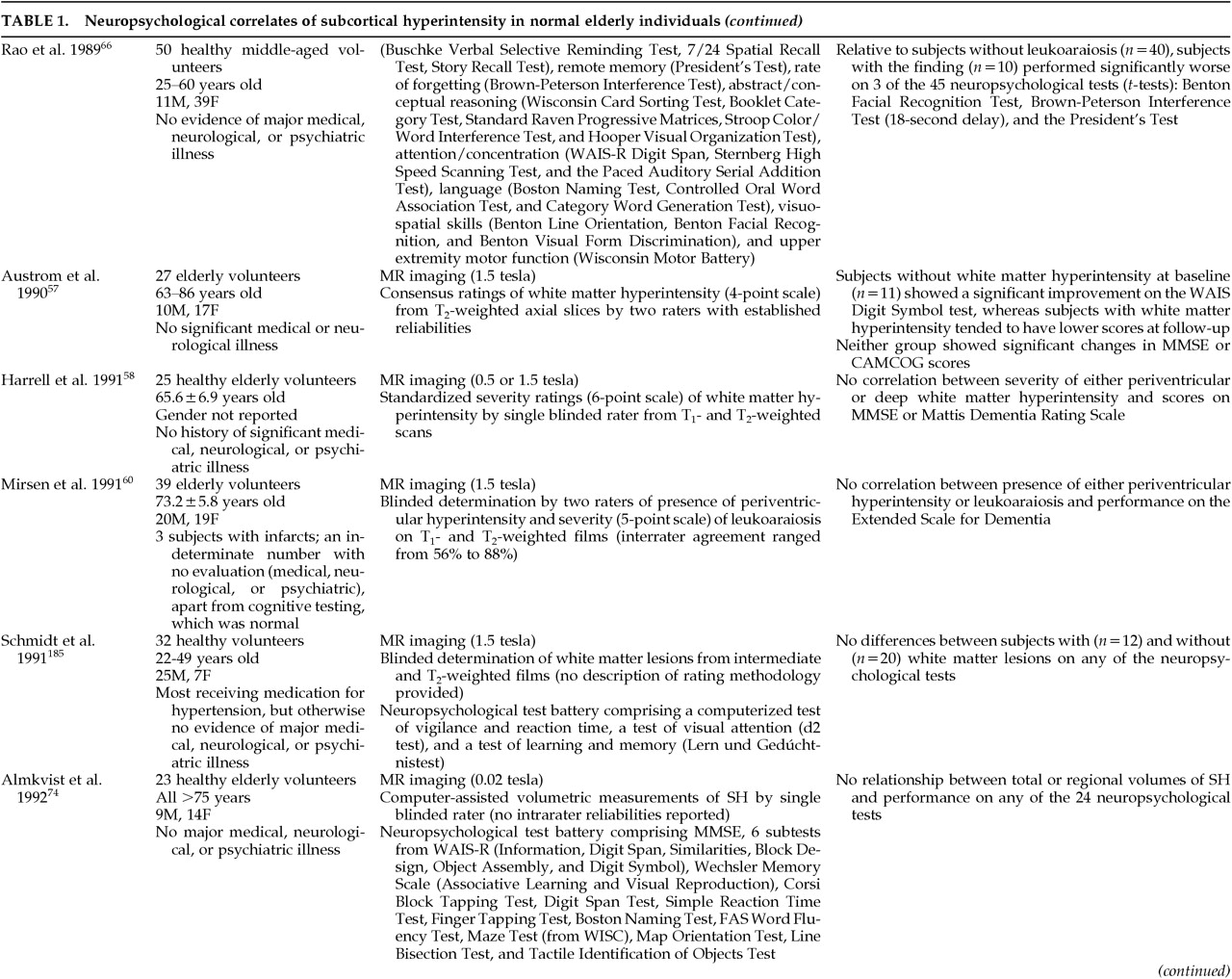
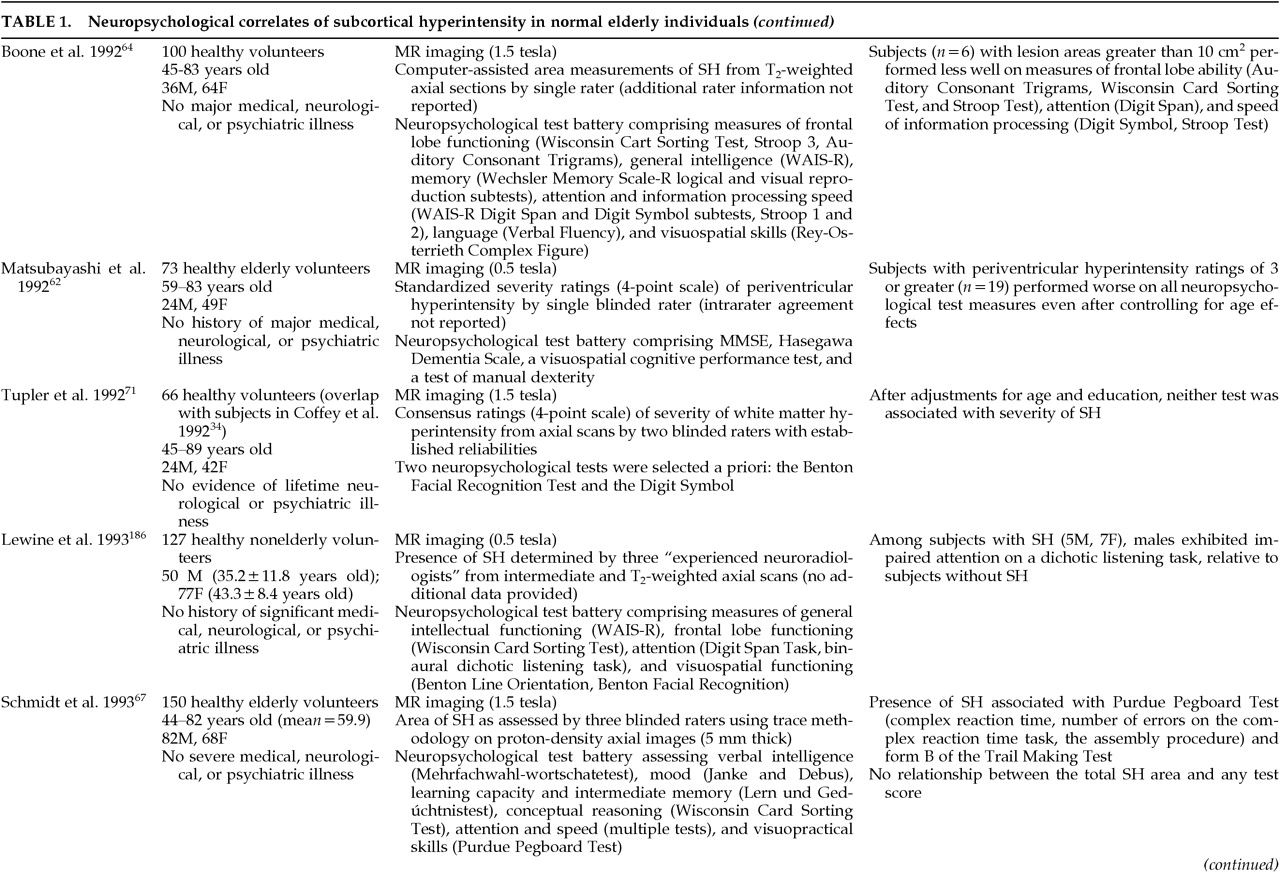
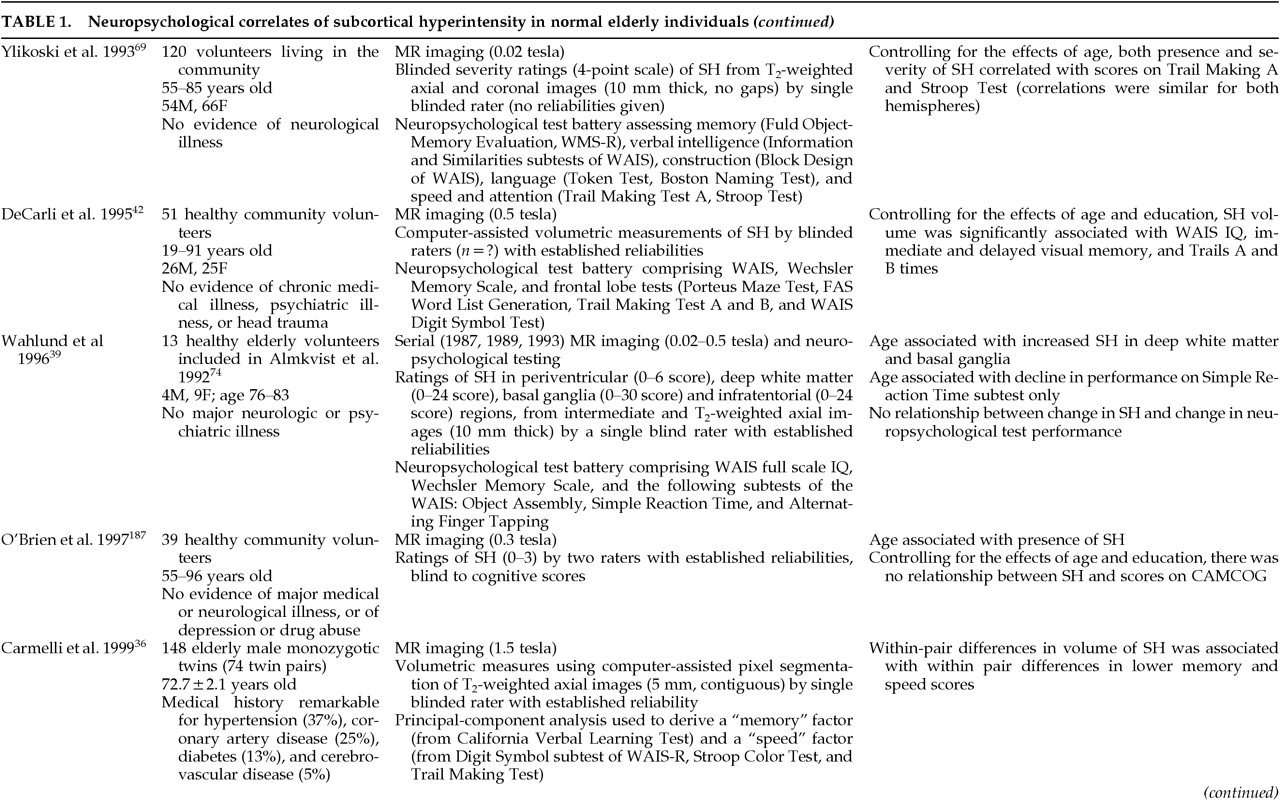
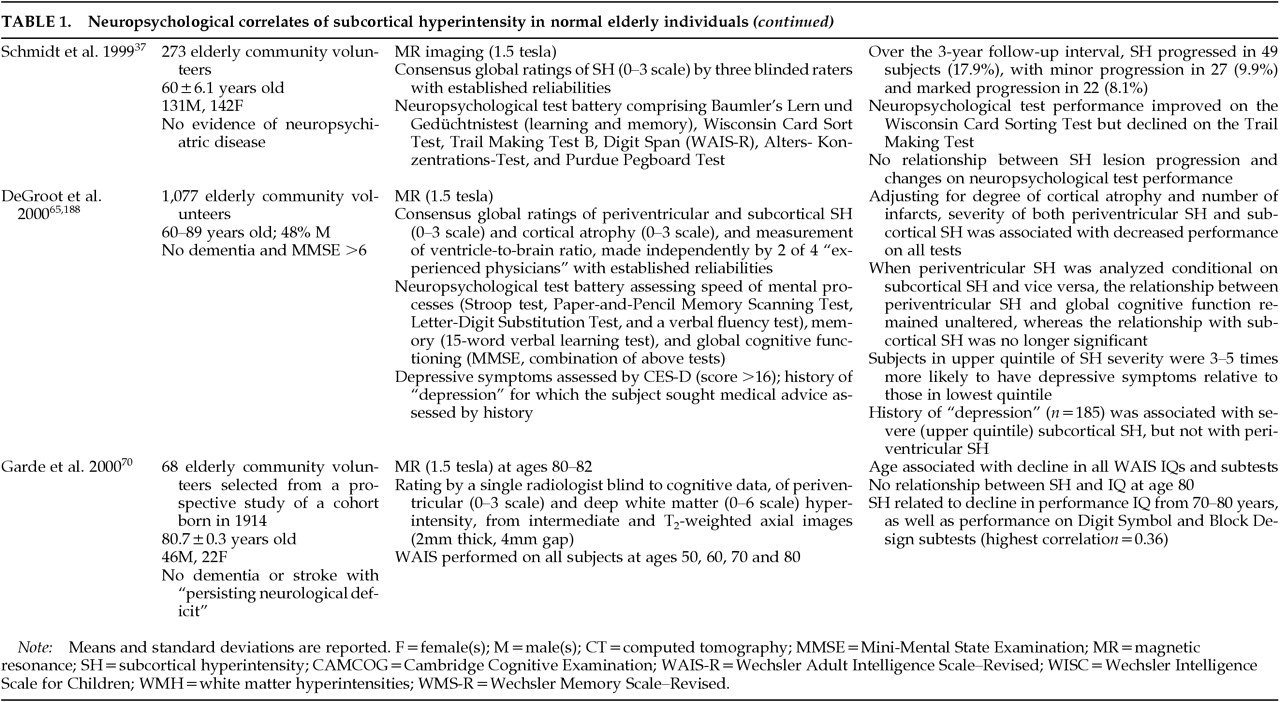
54–56Although a growing literature exists on the relation between cognition and changes in subcortical white and gray matter in normal aging (
Table 1A, Table 1B, Table 1C, Table 1D, Table 1E), these results are conflicting, and the studies are difficult to compare given methodological differences. Most studies find no relationship between SH and scores on dementia rating scales,
57–62 but such measures may be relatively insensitive to subtle changes in cognition. Positive findings have generally been more common among studies using more sensitive neuropsychological assessment batteries, with measures of frontal lobe function demonstrating the closest relationship with SH.
36,37,42,57,63–67,69 Most
57,70 but not all
39 of the small number of longitudinal studies find associations between SH and cognitive decline, but the correlations are generally small and thus account for a relatively small proportion of the variance in test scores (
Table 1A, Table 1B, Table 1C, Table 1D, Table 1E).
In an early study from our laboratory,
71 we examined relationships between SH and two specific neuropsychological instruments: the Benton Facial Recognition Test
72 and the WAIS-R Digit Symbol. The former was chosen because it had yielded the highest level of significance of any test reported to be associated with SH; the latter, because it had been reported to be related to SH by two independent groups (
Table 1A, Table 1B, Table 1C, Table 1D, Table 1E). In addition, both the Benton Facial Recognition Test and the Digit Symbol subtest of the Wechsler Adult Intelligence Scale–Revised (WAIS-R)
73 were favored
a priori because subcortical pathology might be expected to disrupt visuospatial perception and visuomotor execution, respectively. We found that performance on both tests was highly related to age and education, but not to the presence of SH. The majority of our subjects had relatively mild findings of SH, however, and it thus remains possible that more severe changes that reach a certain “threshold” volume might be associated with cognitive dysfunction in otherwise healthy adults.
42,61,62,64,65 Indeed, extensive damage to subcortical white matter tracks would disrupt frontal-subcortical circuitry and possibly provide an anatomical substrate for the mental slowing and disturbed executive functioning seen with aging. Lesion location may also be important, as evidenced by the work of DeGroot et al.,
65 who found relationships between cognitive dysfunction and periventricular SH but not deep white matter SH, when each was analyzed conditional upon the other.
In summary, the occurrence of SH increases with age, and its severity increases in the presence of risk factors for vascular disease or high medical burden. Pathologic correlates of SH vary but appear to reflect the effects of brain hypoperfusion. The presence and severity of SH are associated with changes in brain electrophysiology, blood flow, and metabolism, as well as with dysequilibrium and alterations in cognitive (especially frontal lobe) functioning in normal elderly subjects.
Subcortical Hyperintensity in Patients With Dementia
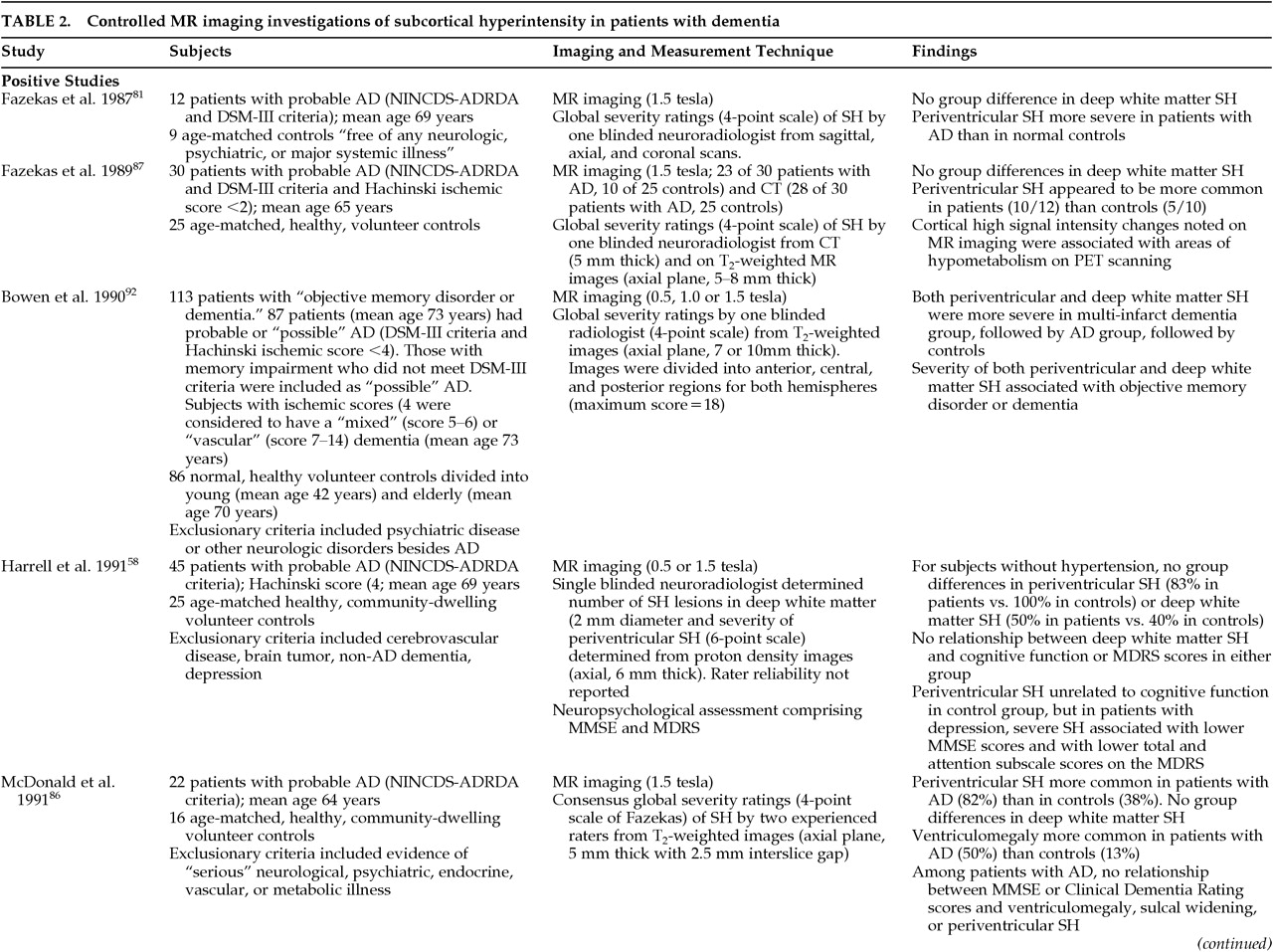
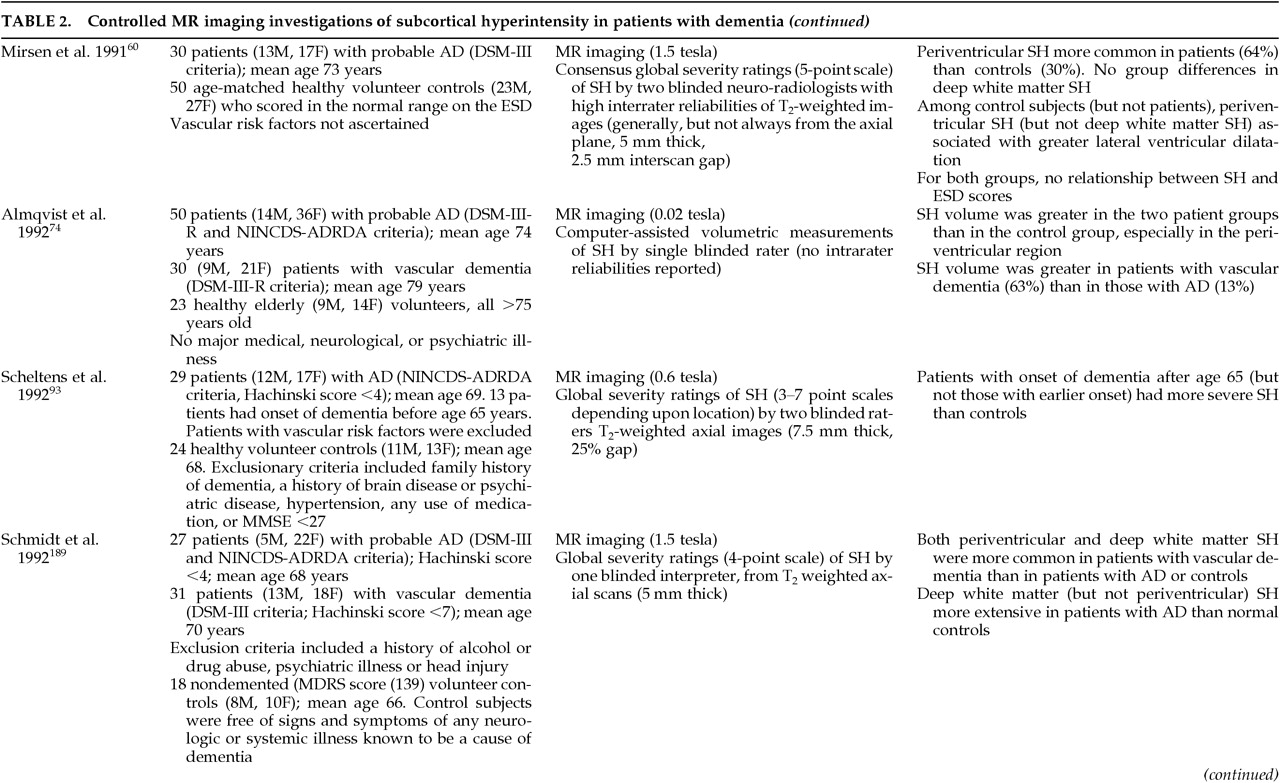
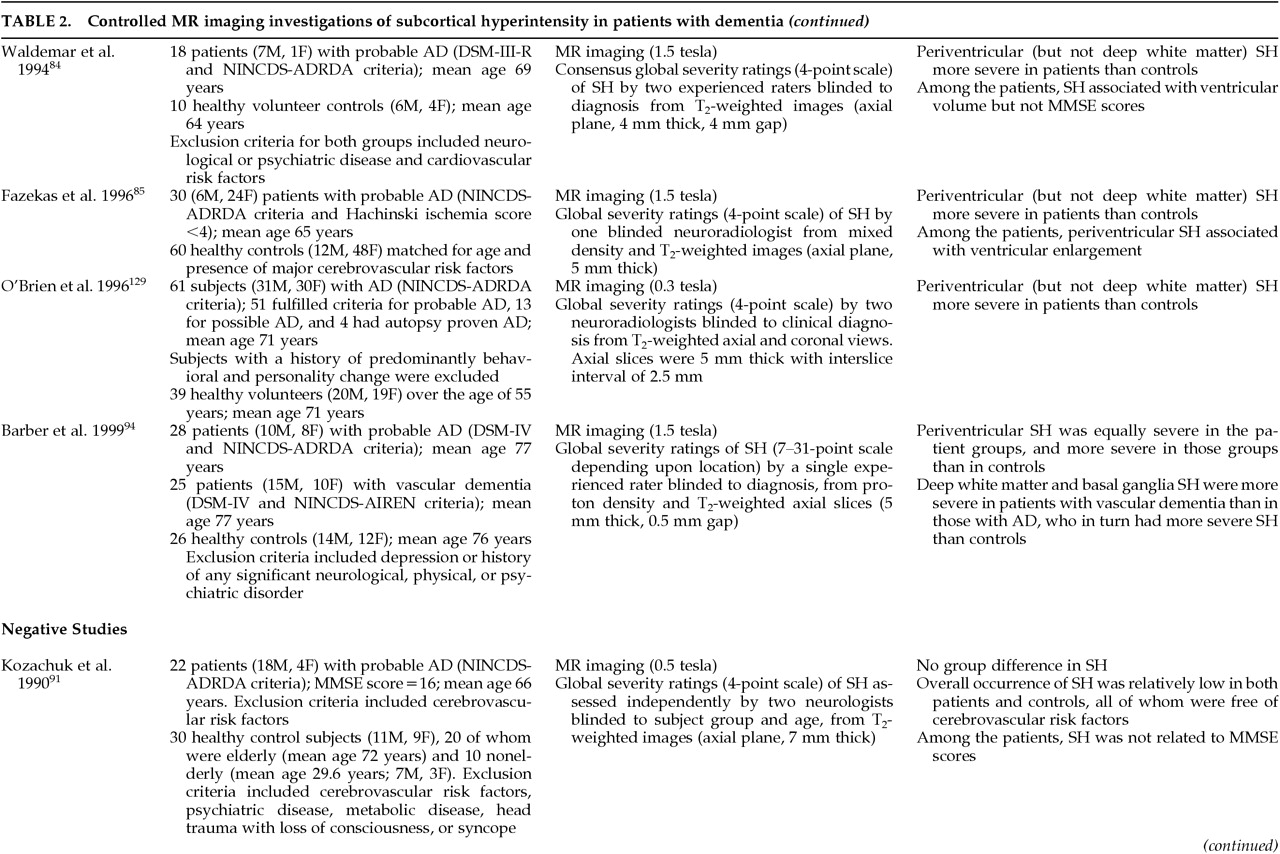
The precise frequency, severity, and distribution of SH in patients with dementia is difficult to determine because of methodological differences between studies in their subject samples (e.g., inclusion of patients with underlying vascular disease), imaging technology, and definitions of SH (
Table 2A, Table 2B, Table 2C, Table 2D). In general, the literature suggests that patients with vascular dementia have a greater frequency and severity of SH (both periventricular and deep white matter) than do patients with Alzheimer's disease or control subjects,
74–83 consistent with the presumed vascular etiology of SH (
Table 2A, Table 2B, Table 2C, Table 2D). Thus, SH has been identified in 33% to 97% of patients with vascular dementia
75–78 compared with 5% to 56% of patients with Alzheimer's disease.
75,76,79–83The data are less clear in studies of Alzheimer's disease, again in part because reports differ in the inclusion of patients with risk factors for vascular disease and in the definition of lesions
58,60,84–97 (
Table 2A, Table 2B, Table 2C, Table 2D). Most studies examining SH in the deep white matter do not find a greater prevalence of SH in patients in patients with Alzheimer's disease than control subjects (
Table 2A, Table 2B, Table 2C, Table 2D). Conflicting findings have been reported for periventricular SH, perhaps due in part to the methodological differences described above (
Table 2A, Table 2B, Table 2C, Table 2D).
In the one published study of dementia with Lewy bodies, Barber et al.
94 found a higher prevalence of SH (both periventricular and deep white matter) in patients than control subjects.
The pathophysiology of SH in patients with Alzheimer's disease is not known but is presumed to be similar to that in control samples, namely a subcortical microvasculopathy.
15,98,99 No relationship has been found between apolipoprotein E E4 allele and the occurrence of SH in patients with probable Alzheimer's disease, vascular dementia, or dementia with Lewy bodies.
100,101Few studies have addressed brain anatomic correlates of SH in patients with Alzheimer's disease.
90,91 Periventricular SH appears to be associated with ventricular dilation (
Table 2A, Table 2B, Table 2C, Table 2D). Fazekas et al.
85 have proposed that ventricular enlargement caused by the loss of periventricular fibers in Alzheimer's disease may disrupt the integrity of the ventricular lining. This disruption may result in increased transependymal flow of CSF into the periventricular white matter with resulting imaging changes of SH.
Data conflict regarding the relationship between SH and cognitive function in patients with Alzheimer's disease (
Table 2A, Table 2B, Table 2C, Table 2D). Studies using global screening instruments such as the Mini-Mental State Examination (MMSE) or Cognitive Capacity Screening Examination generally show no effect of SH on global cognitive functioning.
87,88,90,93,102–104 One exception is Bondareff et al.,
101 who noted a correlation between a volumetric measurement of SH (the “lesion:brain ratio”) and lower MMSE scores. Positive findings are more common among studies that employ a more extensive neuropsychological test battery,
103,105–107 although negative findings have also been reported.
108 Cognitive domains most commonly affected include attention,
107 tactile identification of objects,
103 and frontal lobe function (
Table 2A, Table 2B, Table 2C, Table 2D), although the amount of variance in cognition accounted for by the SH is typically quite small.
105The various functional and clinical consequences of SH in dementia have been examined in several studies. Deep white matter/basal ganglia SH has been associated with reductions in global cerebral perfusion;
109 frontal perfusion;
110 bilateral perfusion in frontal lobe, basal ganglia, and thalamus;
108 and reduced hippocampal perfusion
90 in studies using single-photon emission computed tomography (SPECT). Other SPECT studies, however, show no correlation between SH and cerebral perfusion in patients with Alzheimer's disease.
111 Yamaji et al.,
112 using positron emission tomography (PET), noted significantly lower global cerebral blood flow in their cohort of patients with Alzheimer's disease and SH versus patients without SH. It is of interest that oxygen extraction was increased in involved areas, suggesting adequate compensation for the reduction in blood flow. This finding may account for the number of studies that show little or no cognitive impairment in the setting of SH.
Other reported clinical correlates of SH in patients with Alzheimer's disease include a higher risk of subsequent stroke,
113 higher apathy scores, motor incoordination and gait disturbance,
108 urinary incontinence, and purposeless activity such as wandering.
114Barber et al.
94 reported that frontal white matter hyperintensities were associated with depressive symptomatology in patients with Alzheimer's disease, dementia with Lewy bodies, or vascular dementia. They also observed that occipital white matter hyperintensities were associated with the absence of visual hallucinations.
In a one-year longitudinal study, Lopez et al.
115 found no difference in cognitive change between patients with Alzheimer's disease and periventricular SH versus those patients without SH. In addition, the frequency of major depression, delusions, and hallucinations did not differ between the two groups. However, the presence of periventricular SH did predict the development of clinically significant cerebrovascular disease.
In summary, both periventricular and deep white matter/basal ganglia hyperintensities appear to be more common and generally more severe in patients with vascular dementia than in those with probable Alzheimer's disease or Lewy body dementia, and all three groups may have more extensive changes than healthy age-matched control subjects. In patients with dementia, more extensive or severe SH may be associated with brain structural (especially ventricular enlargement) and metabolic changes; with impairment in cognition, gait, and motor coordination; with depressive symptoms (especially for frontal SH); and with subsequent risk of stroke.
Subcortical Hyperintensity in Patients With Mood Disorders
It has been known for some time that patients with Binswanger's disease may present not only with dementia but also with a variety of other neuropsychiatric symptoms, including delirium, behavioral disturbances, mania, psychosis, social withdrawal, abulia, and depression.
9,11,14,15,17Early clinical reports suggested an increased rate of SH in elderly patients with severe depression referred for ECT
14,15,17,116 or in patients with bipolar illness.
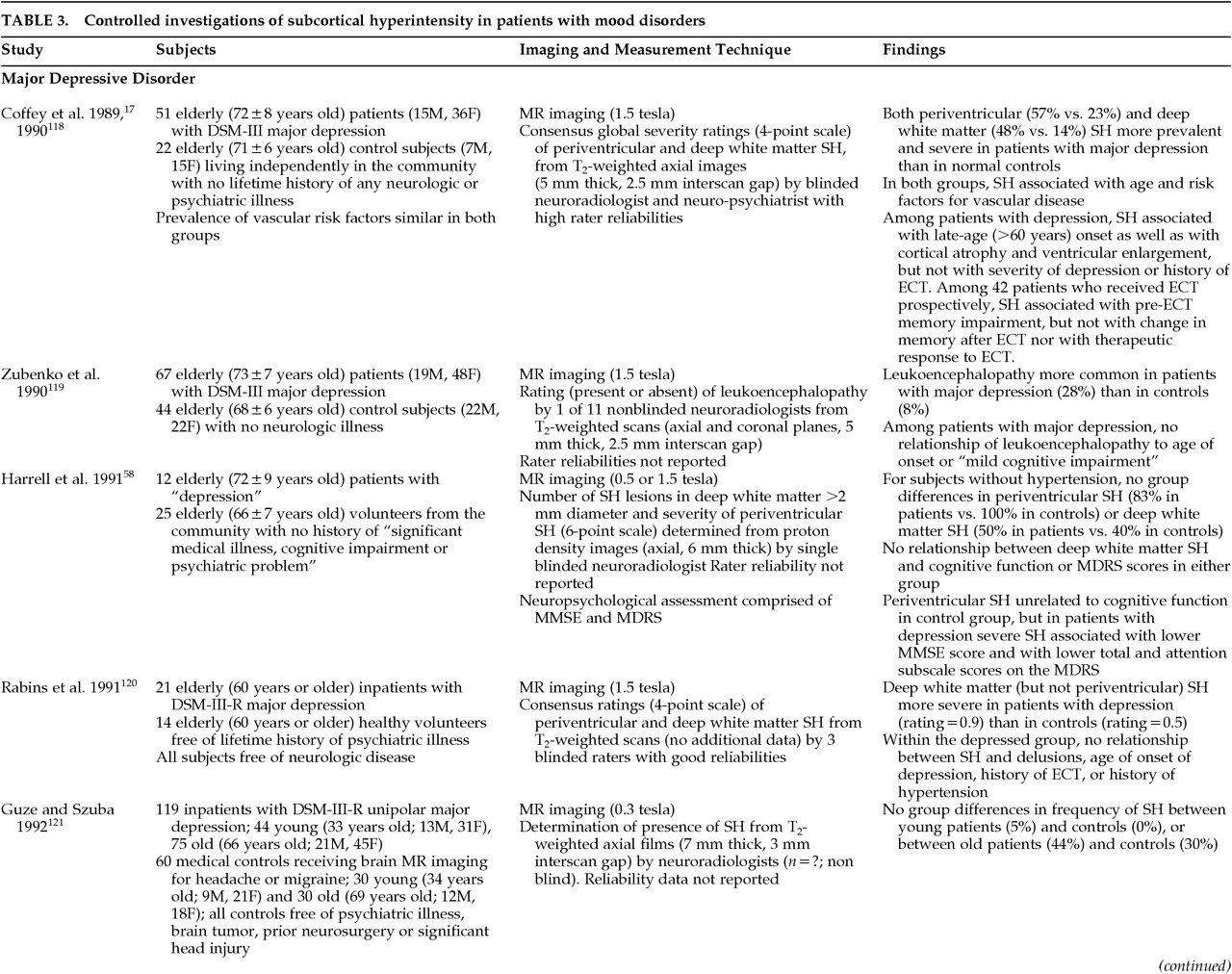
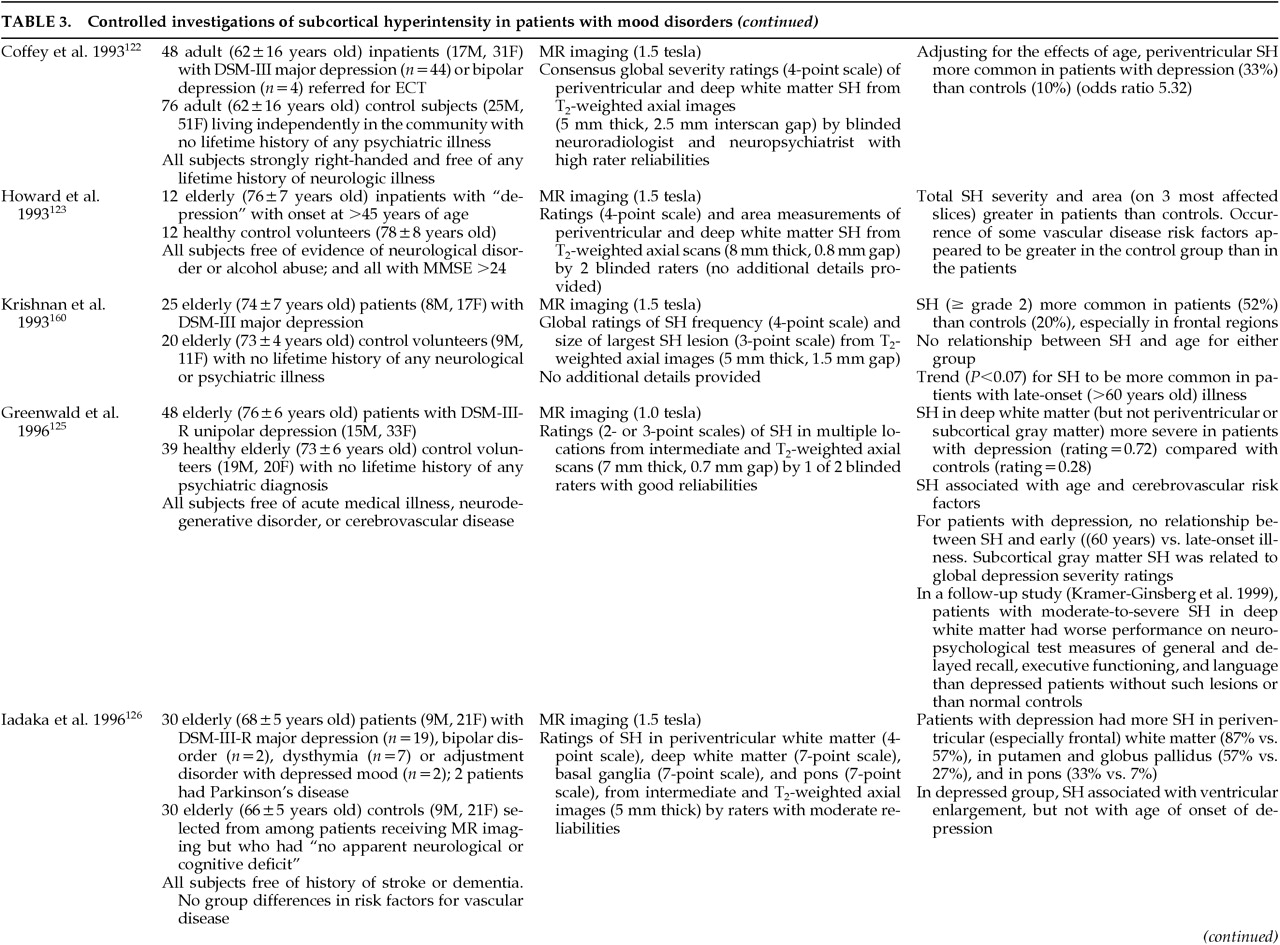
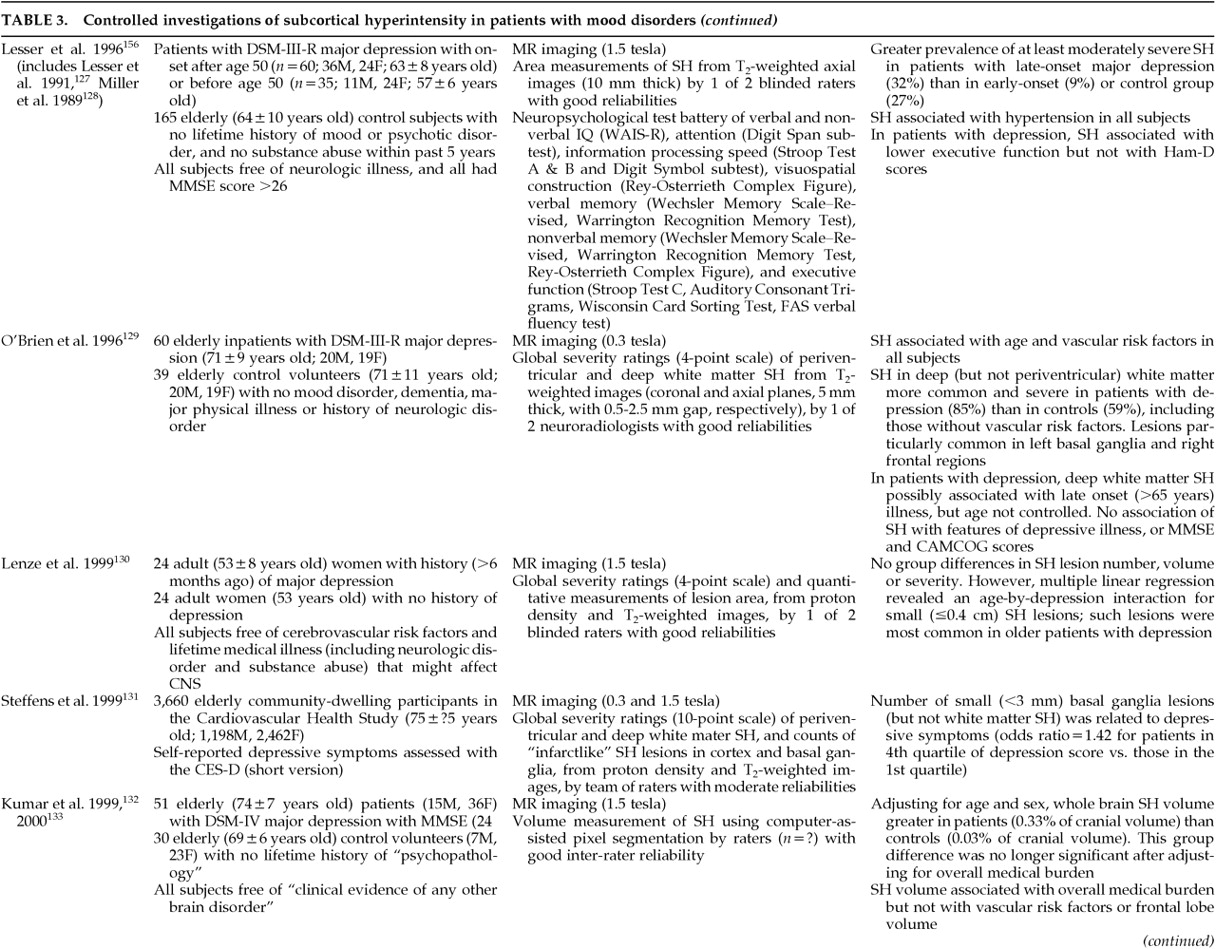
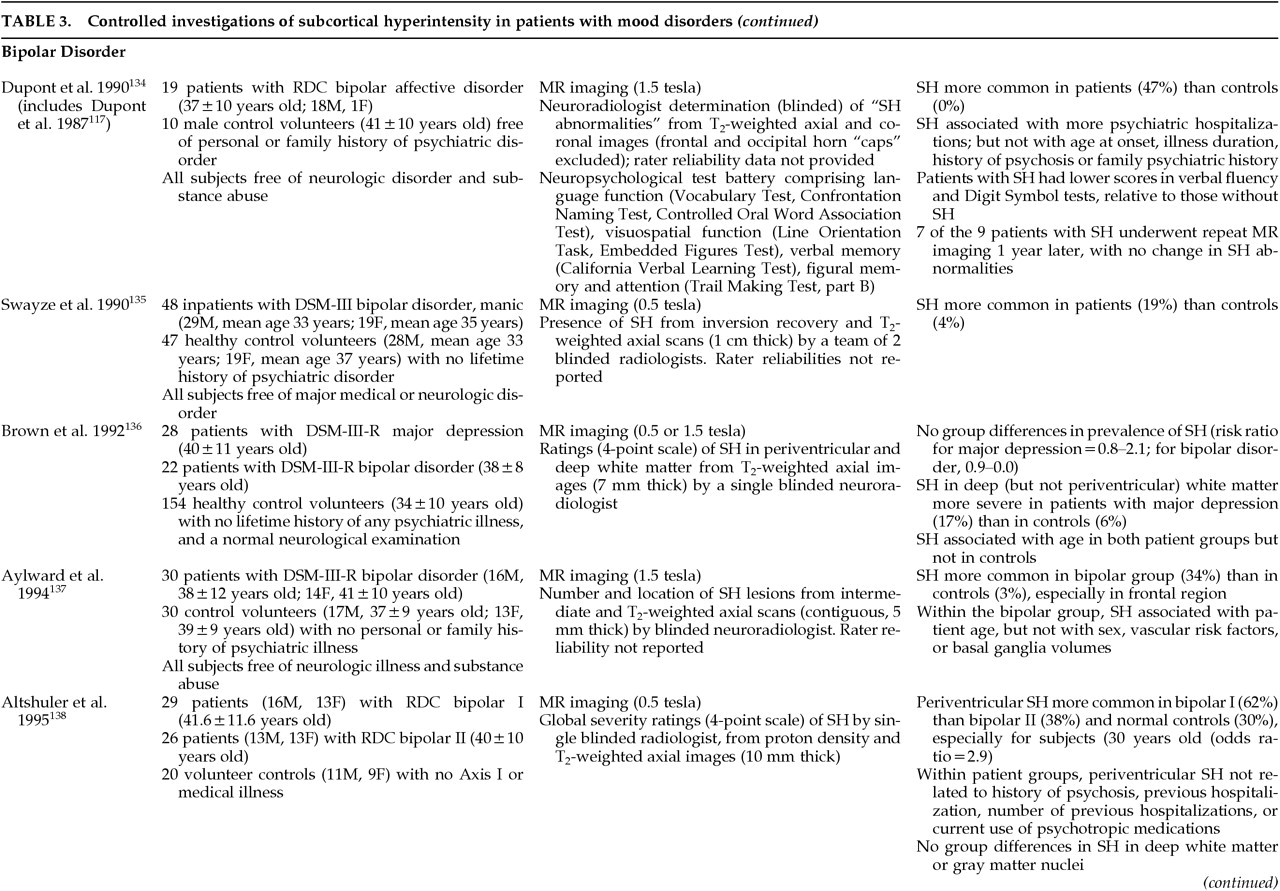
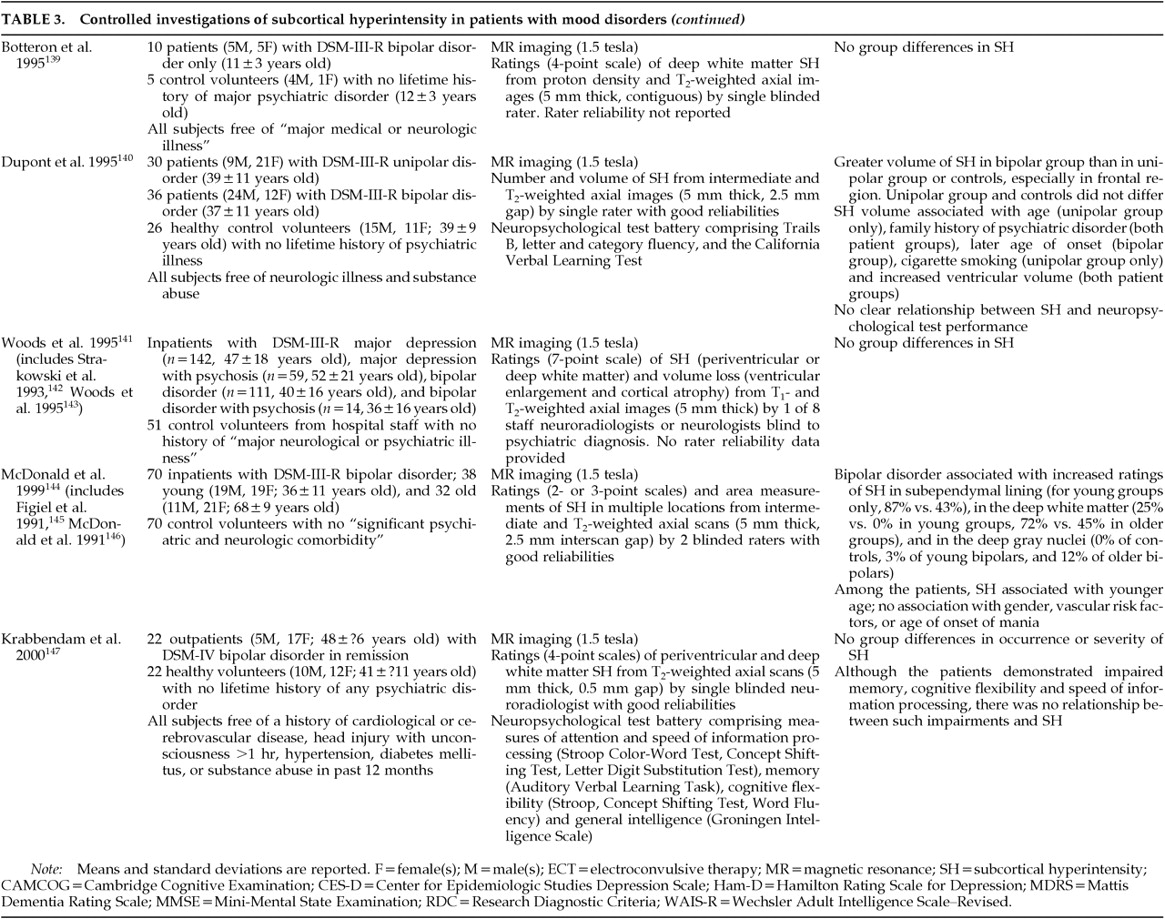
117 Subsequently a large number of controlled investigations demonstrated that SH is indeed more common or severe in patients with major depression or bipolar disorder (
Table 3A, Table 3B, Table 3C, Table 3D, Table 3E118–147). The precise frequency of SH in these populations is difficult to determine, however, given differences between studies in subject samples (e.g., in age, sex, and health status including vascular risk factors or disease), in imaging technology, and in lesion definition and measurement (
Table 3A, Table 3B, Table 3C, Table 3D, Table 3E). A recent meta-analytic study
148 of the extant literature reported a common odds ratio (Mantel-Haenszel technique) of 3.2 (95% confidence intervals of 2.11 and 4.82) for SH in patients with major depression, and 3.29 (95% CI of 2.14 and 5.07) in patients with bipolar disorder. The SH lesions in patients with mood disorders are typically localized to the frontal white matter and the subcortical gray nuclei (thalamus, basal ganglia;
Table 3A, Table 3B, Table 3C, Table 3D, Table 3E). As noted above for nonpatient samples, SH in patients with mood disorders is associated with age and overall medical burden, including risk factors for vascular disease (
Table 3A, Table 3B, Table 3C, Table 3D, Table 3E). As such, SH in patients with mood disorders is also associated with other age- or illness-related changes in brain structure, including global or regional atrophy and ventricular enlargement (
Table 3A, Table 3B, Table 3C, Table 3D, Table 3E). Finally, SH and microinfarction are associated with depression in patients with vascular dementia.
149The pathophysiology of SH in patients with mood disorders is not known but is presumed to be similar to that in control samples, that is to say a subcortical microvasculopathy.
15,98,99 Little is known about the natural history of SH in patients with mood disorders. One study of 7 relatively young adults with bipolar disorder found no changes in SH ratings at 1-year follow-up.
134 In a prospective study of the brain anatomic effects of ECT, we observed an increase in the severity of SH 6 months after a course of ECT in 5 of 35 patients with depression.
150 Such changes were interpreted to reflect progression of ongoing cerebrovascular disease rather than an effect of ECT.
Although studies in control samples have demonstrated functional brain correlates of SH by using quantitative EEG, PET, functional MR imaging, and MR spectroscopy as noted above, very few such data have been reported for patients with mood disorders.
151,152 Ebmeier et al.
153 found a correlation between periventricular SH and widespread periventricular and bilateral temporal perfusion defects on PET among 39 elderly patients with major depression. No relationships were observed for SH in the deep white matter. We observed a relationship between SH in the pons and shortened REM sleep latency in patients with major depression, a finding of interest given that REM sleep is felt to be mediated by systems located in the pons.
154A growing literature has focused on the clinical significance of SH in patients with mood disorders. Onset of major depression at a late age (>60 years old) has been associated with SH in most
15,17,123,155–160 but not all
119,120,125,126 studies of patients with unipolar disease, as described below. Most studies in patients with bipolar disorder find no relationship between SH and age at onset.
134,144,145 Most reports find no relationship between SH and psychotic symptoms
128,134,138,145 or severity of depression.
17,58,129,134,138,156,161 Apathy, anhedonia, and functional disability have been suggested as possible correlates of SH in elderly patients with major depression.
162 No relationship between SH and a family history of mood disorder has been found for patients with major depression,
155 but conflicting findings have been reported for patients with bipolar disorder.
134,140,145,147 Although SH is associated with dysequilibrium in elderly control samples as mentioned above, no study has examined such relationships in elderly patients with mood disorders.
Several studies have found a relationship between SH and cognitive impairment in patients with major depression.
17,58,155,156,161,163 The few studies that have reported negative findings typically used screening measures rather than more sensitive neuropsychological test batteries
119,129 (
Table 3A, Table 3B, Table 3C, Table 3D, Table 3E). Consistent with the effects seen in control samples as described above, the cognitive disturbance is typically manifest as cognitive slowing, memory deficits, and frontal lobe/executive dysfunction (
Table 3A, Table 3B, Table 3C, Table 3D, Table 3E). Conflicting findings have been reported for bipolar disorder.
134,147Little is known about the impact of SH on treatment outcomes in patients with mood disorders. In a small (
N=39) study of older inpatients with severe (mainly psychotic) depression, Hickie et al.
155 found that SH was associated with a poorer response to either pharmacotherapy or ECT. While our experience is consistent with the former finding, we observe a good response to ECT even in depressed patients with extensive SH.
14,15,17,150 We and others have found, however, that the presence or severity of SH may be predictive of treatment side effects, including delirium from ECT
116 or antidepressant medications
164 as well as neuroleptic-induced parkinsonism.
165 Similar observations were reported by Fujikawa et al.
166 in a study of patients with major depression and silent cerebral infarction on brain MR imaging. They found that those patients with silent cerebral infarction (SH or cortical infarct) had a greater frequency of “adverse central nervous system reactions” to antidepressant drugs; these reactions included delirium, parkinsonism, dyskinesia, and akathisia.
With regard to the long-term prognosis of patients with SH and mood disorders, one group found a correlation between SH and number of prior hospitalizations but not duration of current bipolar illness.
134,140 In a longitudinal investigation of mainly older patients with depression, Hickie et al.
167 found that cognitive decline and functional impairment were associated with the severity of SH on MR imaging when SH were noted 6 months to 2 years previously.
The association of SH and mood disorders has led to interesting speculation about the direction of causation. Clearly, the occurrence of SH will be greater in patients with overt vascular disease, but as noted in
Table 3A, Table 3B, Table 3C, Table 3D, Table 3E, the relationship between SH and mood disorders remains significant in some studies even after adjustment for medical burden and traditional vascular risk factors. The association between SH and late-age-onset mood disorders has also led to the suggestion that SH or the vascular disease with which it is associated may be causative of the depression, at least in some patients.
162,168,169 Consistent with this view is the finding of a lack of family history of mood disorder in patients with SH and depression.
155 Indeed, depression is a common symptom of subcortical brain disease (e.g., Parkinson's disease, Huntington's disease, multiple sclerosis) and the frontal predominance of the SH lesions in patients with mood disorders positions such lesions to disrupt (disconnect?) frontal-subcortical circuits that appear to be important in regulation of emotional behavior.
17,170,171 At a neurochemical level, one report suggests that SH in geriatric depression is associated with reduced platelet [
3H]-imipramine binding, a potential marker for presynaptic serotonergic function.
172 Another potential causative mechanism is suggested by the association of SH and cognitive impairment; such impairment might result in limited coping strategies with which to respond to stress, leading to depression.
160There are other lines of evidence to suggest, however, that depression may be causative of cerebrovascular disease. Depression is associated with a variety of pathophysiologic alterations that may increase vulnerability to vascular disease,
173 including increased platelet activation.
174 Indeed, recent prospective data demonstrate an association between baseline depressive symptoms and subsequent stroke as well as stroke mortality,
175–177 even after adjustment for established stroke risk factors. Treatment of depression with medications that induce hypotension could also theoretically cause or worsen SH and cerebrovascular disease,
118 but no such relationships have been found.
134,135,138,140,145 There is no evidence that SH in patients with mood disorders is causally related to treatment with ECT.
17,120,129,145,150Of course, as noted by Videbech,
148 association does not prove causation, and there are other possible mechanisms to explain the relationship of SH and mood disorders. For example, the relationship may be mediated through a nonrelated confounder (e.g., medical burden), or SH could even be a result of treatment of depression (although, as noted above, the data do not appear to support this latter contention). Clearly, our understanding of the relationships between SH and mood disorders requires longitudinal studies of the development of SH and of mood disturbance, using appropriately matched control groups and standardized techniques for lesion assessment.
In summary, the prevalence and severity of SH is increased in elderly patients with major depression, in patients with bipolar disorder, and possibly in non-elderly patients with major depression. The SH in these populations is presumed to reflect subcortical microvascular disease, but the precise etiology of the vasculopathy is unknown. The SH may be associated with late-age onset of the major depression, cognitive impairment, a relatively poorer response to treatment, and an increased risk of cerebral side effects from treatment. The association of SH and mood disorders has led to interesting speculation on the mechanisms of mood disorder in patients with cerebrovascular disease.