Modern society places a premium on effective cognitive functioning in both social and professional settings, and even a slight decline in cognitive capabilities can result in significant functional impairment. Head injury is one of the most common causes of cognitive impairment in the young, and the estimated incidence of traumatic brain injury is 200 to 300 per 1 million people in Scotland and the United States.
1,2The majority of head injury is graded as mild, with an initial Glasgow Coma Scale (GCS)
3 score of 13 or higher at first assessment.
4Although there is a relationship between the severity of the injury and the ultimate outcome, even mild traumatic brain injury (mTBI) without a loss of consciousness can lead to long-lasting cognitive sequelae.
5–7 Many patients complain of headache, dizziness, and concentration problems after mTBI, but within a few weeks these symptoms subside and most patients return to their normal activities. However, 6 months after mTBI, 15% to 29% of patients still have persistent problems,
5 and these can continue for years.
Although an at least partially organic origin of the postconcussional disorder is no longer a matter of debate,
4,8 a biological marker is still missing, and little imaging evidence exists for this assumption. Oppenheimer
9 found microscopic lesions that were probably of traumatic origin in the brains of 5 individuals who sustained mTBI and died of other causes. In laboratory animals, mild injuries caused subtle axonal damage in the absence of gross focal lesions such as contusion or laceration.
10Previous imaging studies with computed tomography (CT) have focused on moderate to severe brain injury, mainly because of the limited sensitivity of CT, which makes the technique less suitable for studying mild to moderate traumatic brain injury. In the acute phase of white matter injury, CT has a sensitivity of only 20%.
11 Several studies have shown MRI to be more sensitive than CT,
11–14 especially in the detection of nonhemorrhagic contusion and axonal injury, lesions commonly found in mTBI.
The application of new MR techniques can further increase the sensitivity of imaging subtle posttraumatic changes. We therefore performed an explorative study in patients with persistent postconcussional sequelae to assess the value of a new MR technique.
Magnetization transfer imaging (MTI) provides higher sensitivity than conventional T2-weighted images in identifying parenchymal lesions. With most conventional MR techniques, image contrast is based on differences between tissue in T1 and T2 relaxation time and on proton density. Magnetization transfer (MT) assessment provides information about the tissue that is different from the information provided by T1 and T2 relaxation times.
The physical principle of MTI is based on the interaction between mobile protons and protons associated with macromolecules.
15–17 The MRI signal is derived from the water-associated, mobile protons, and the effect of the macromolecular protons is perceived indirectly by transfer of magnetization to mobile protons. This transfer results in a diminished magnetization of these water protons and therefore in a lower signal intensity on the MR image. The MT effect can be quantified by acquiring two images, one with and one without a specific prepulse that maximizes the MT effect, and calculating a suitable ratio (MTR).
Myelin, which is the main constituent of white matter, is considered to be an important macromolecular structure in MT, and loss of macromolecular structure decreases the MT effect. A decrease in MTR is found in the early stages of wallerian degeneration, where conventional imaging sequences fail to detect abnormality.
18 MTI also detects lesions in normal-appearing white matter in multiple sclerosis and metastasis.
19–21 A recent animal study has shown that MTI is sensitive for posttraumatic lesions: areas in the brain that had an altered MT but a normal appearance on T
2-weighted scans were found to have axonal disruption and secondary degenerative changes on histopathologic examination.
22Typically the MTR is analyzed in a two-dimensional region of interest. Although this will show focal lesions, diffuse brain abnormalities commonly seen in posttraumatic patients are not easily assessed in this way. Histogram analysis allows for the assessment of a volume of brain tissue and for the quantification of both high-contrast lesions and diffuse abnormalities in normal-appearing white matter.
23,24 This method of analysis fully exploits the potential of MTI to detect microscopic lesions.
The present study was conducted 1) to study the relationship between structural brain abnormalities and symptoms after mild to moderate traumatic brain injury, and 2) to assess the potential of MTI for quantifying brain injury. We selected a population with a high a prior risk of abnormalities in order to asses the applicability of this new technique. The subjects were patients with a postconcussional disorder (DSM-IV
25) who presented at a university-based memory clinic and matched control subjects.
METHODS
Subjects
Patients with a postconcussional disorder who attended the Memory Clinic of the University Hospital Maastricht were enrolled in the study. The criteria of the DSM-IV classification were used for the diagnosis of postconcussional disorder.
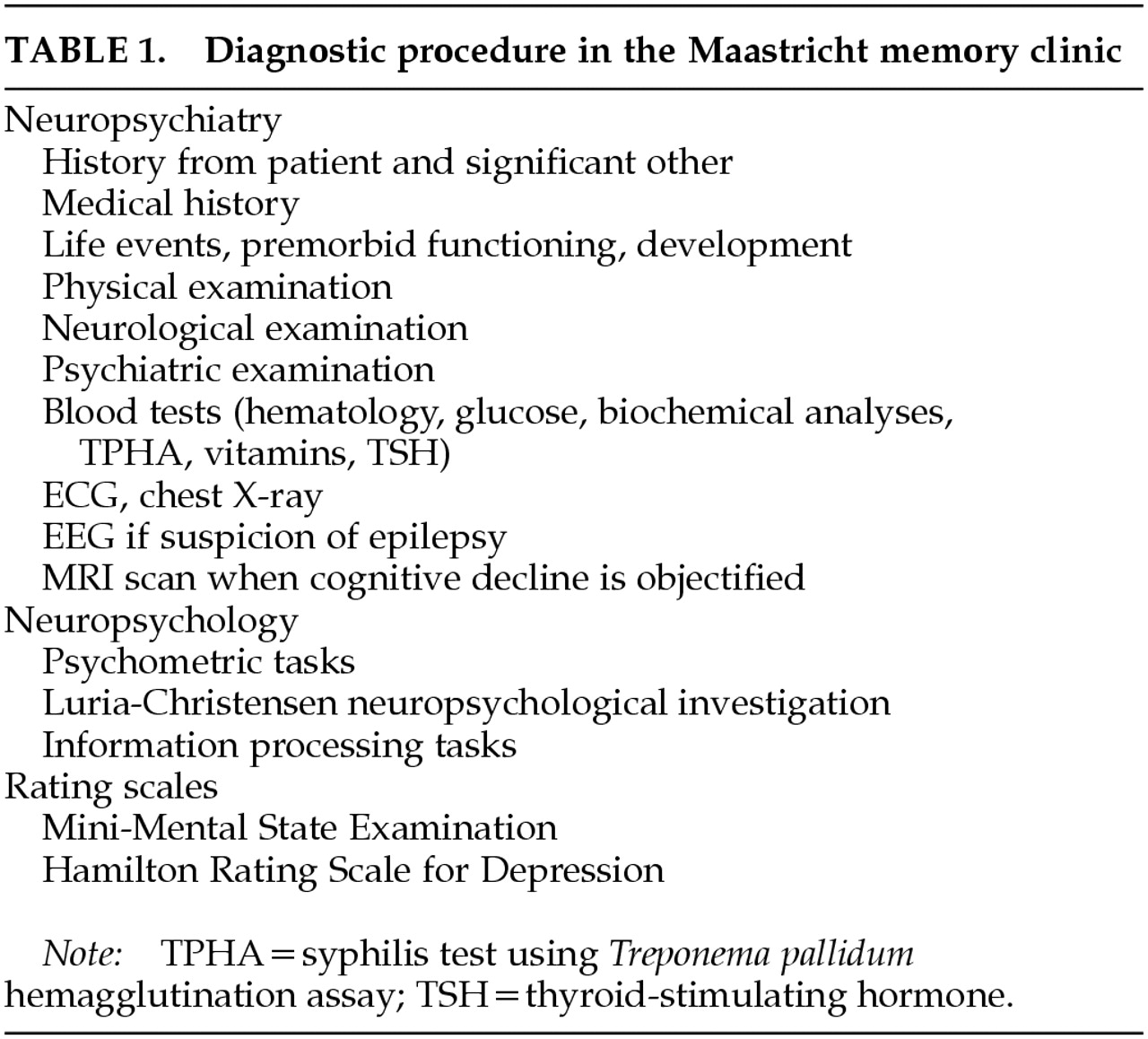
25 These criteria include a history of head trauma that caused significant cerebral concussion; evidence from neuropsychological testing or quantified cognitive assessment of difficulty with attention or memory; and three or more of the following complaints: becoming fatigued easily, sleeping disorder, headache, dizziness, irritability, anxiety, depression, affective lability, personality changes, or apathy. These complaints must have commenced, or substantially worsened, after the trauma, and must have affected social or professional functioning. All patients underwent a standardized diagnostic assessment as described elsewhere,
26 the elements of which are shown in
Table 1. Psychiatric diagnoses were according to DSM-IV criteria.
25 All patients were administered the Hamilton Rating Scale for Depression (Ham-D),
27 which was used both as a structured symptom checklist for depressive symptoms and, in case of depressive disorder, as a measure of severity. Major psychiatric disorders were excluded on the basis of a clinical interview, and for depression and other affective disorders, by absence of core symptoms of depression as measured with the Ham-D. All patients had sustained a closed head injury at least 1 year before they took part in this study. The GCS score
3 recorded in the patient file was used to assess the severity of the trauma. Patients who sustained significant extracranial injury were not included in this study. Furthermore, patients were excluded when a physical, neurological, or psychiatric disorder—including somatic disorders, stroke, epilepsy, neurodegenerative disorders, alcohol abuse, depressive disorder, or psychosis—was diagnosed, or when they used medications with known psychoactive effects. The only psychiatric symptoms accepted were those of the postconcussional disorder. A healthy control group without history of mild brain injury, matched pairwise for sex and age, was recruited from the general population by advertisement in newspapers. The control subjects underwent a neurological and psychiatric examination, and subjects were excluded when a physical, neurological, or psychiatric disorder was diagnosed or when they used medications with known psychoactive effects. Subjects were not reimbursed for their participation. All subjects gave their written informed consent to participate in the study, which was approved by the Medical Ethics Committee of the University Hospital Maastricht.
Neurocognitive Testing
Both the patient and control groups underwent a standardized neuropsychiatric and neuropsychological examination. The neuropsychological assessment included tests for verbal memory, basic cognitive speed, and speed of complex operations. These tests were used because earlier research indicated that these cognitive aspects are most relevant in postconcussional syndromes.
28,29 The Word Learning Task (WLT) is based on the Auditory Verbal Learning Test
30 and evaluates the ability to acquire and retain new verbal information. Susceptibility to perceptual interference was measured by the Stroop Color Word Test (SCWT),
31 which consists of three subtasks: color word naming (I), color naming (II), and naming of color words printed in a different color (interference task, III). The Memory Scanning Test (MST) is designed to study the speed of memory processes.
32 The test is based on the principle that additional time is needed to complete a task when there is a stepwise increase in the amount of information to be kept in memory. It reflects the ease with which information is processed in the working memory.
The test results were reduced to three variables by making composite scores for memory, sensorimotor speed, and cognitive speed.
33 This was done to reduce the number of dependent variables while improving the robustness of the underlying cognitive construct.
31,33,34The memory score was composed of the results of three WLT tasks: total number of recalled words (WLT1–WLT5), the maximum number of words recalled (TOTG), and the total number of words of the delayed recall (DRCLL). The score of cognitive speed was composed of the slope of the memory scanning test for test with three letters (MSTL3), and the Stroop interference task (STR3). The sensorimotor speed score was calculated by using the basic speed of the memory scanning test (% task MSTPT), the reading speed of the Stroop test (STR1), and the basic speed of memory scanning test of one letter (MSTL1). For transformation into
z-scores, the means and the standard deviations of the normative data of different age groups published by Houx
34 were used as reference. Care was taken to match the study population with the reference population, but because both groups were compared with the same reference population, the absolute difference between the patients and the control group is independent of the reference population.
Neuroimaging
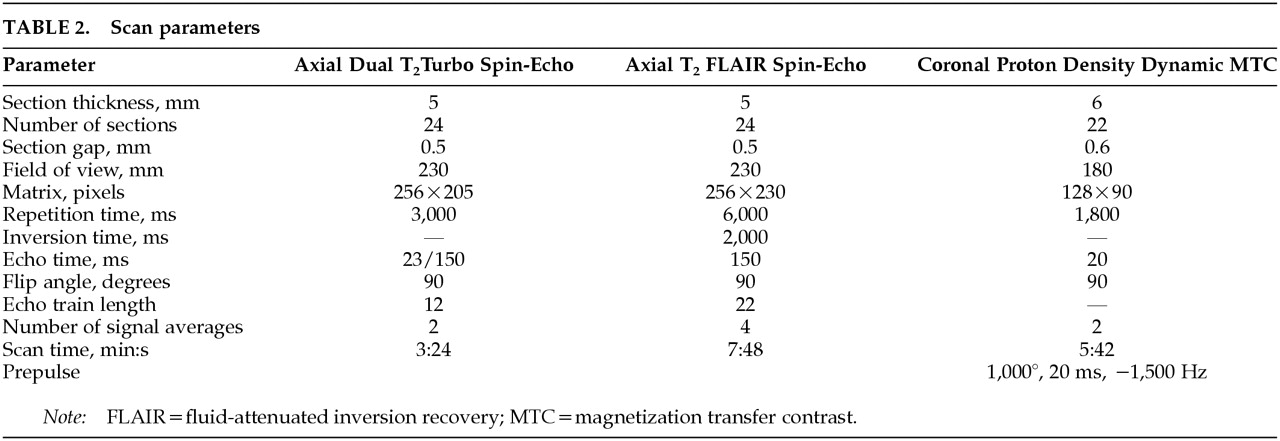
MR images were acquired on a Philips ACS system operating at 1.5 tesla. A scout sequence was used to align the subsequent scans. The MR examination protocol consisted of an axial proton density and T
2-weighted fast spin-echo (FSE) sequence and an axial T
2-weighted fluid-attenuated inversion recovery (FLAIR) sequence (
Table 2). MTI was performed with a spin-echo proton density–weighted sequence, with and without an off-resonance prepulse (
Table 2). The patients were also studied with a T
2-weighted gradient echo sequence (T
2 FFE) to detect hemosiderin depositions.
Lesion Analysis
The hard copies of the MRI studies were screened for abnormalities by a neuroradiologist. The lesions were scored on a semiquantitative scale as proposed by Scheltens et al.
35 This formal rating scale uses a score of 0–6, with separate scores for each of the cerebral lobes, the periventricular, the subcortical regions, and the infratentorial brain structures. The maximum possible cumulative score for the cerebrum is 24; the maximum score for one region is 6. Perivascular spaces were disregarded. The rater had no knowledge of the clinical data. The reliability of this rating scale was assessed in a previous study.
36Image Processing
The MT images were transmitted to a separate workstation (PowerPC, Apple Macintosh), and we used our own software to calculate an MTR image according to the formula
37MTR=(Moff−Mon)/Moff
where Moff and Mon represent the signal intensity with the saturation prepulse off and on, respectively. In the resulting image, the pixel grayscale value equals the local MTR. From the coronal data set, the slices anterior to the splenium of the corpus callosum were selected for further analysis. This was to ensure that the data set of each individual included the same anatomical regions.
MTR is typically measured in a region of interest (ROI), and the results depend on the position of the ROI. Another approach is to analyze the entire data set by presenting the MTR data as a histogram.
23 This method introduces a bias because the MT data of both gray and white matter are analyzed together and a change in gray/white ratio causes a change in the MTR histogram that is unrelated to a change in the MTR. A new postprocessing technique to circumvent this problem has been developed. White matter is segmented from cerebrospinal fluid, gray matter, and extracerebral tissue, and subsequently the histogram of the normalized white matter MTR distribution is analyzed. To characterize this histogram we fitted a Gaussian function to the data, and thus the MTR histogram is characterized by the amplitude, the mean MTR, and the curve width.
24Statistics
Statistical analysis was performed by using nonparametric and parametric tests as appropriate. Significance was tested with two-tailed tests, and a P-value of less than 0.05 was considered significant.
RESULTS
Demographics
Thirteen patients (7 men, 6 women) met the criteria for inclusion in the study. The mean age was 40 years (range 21–62 years, SD=13.17). The mean interval between the trauma and presentation was 4 years (range 1–12 years), and the median initial GCS score was 14 (9–15). The median duration of posttraumatic amnesia was 2 hours (0–336), and the median duration of loss of consciousness was 10 minutes (0–1,200). Patients and control subjects were comparable with regard to level of education on a 7-point scale
38 (patients 3.9, control subjects 4.2,
P>0.1). Although many patients had complaints of mildly lowered mood, only 1 patient had a score on Ham-D in the range of clinically relevant depression (i.e., score >17; mean Ham-D=12.4, range 6–19). The patient with a Ham-D score of 19 had complaints of affective lability, lowered mood, and anxiety, but had no other clinical signs of major depressive disorder.
The subjects of the control group were matched for sex (7 men and 6 women) and age (mean age 40 years, range 20–62 years, SD=13.76; t=0.01, df=24, P=0.99). None of the subjects in the control group had sustained a head injury.
Neuropsychological Tests
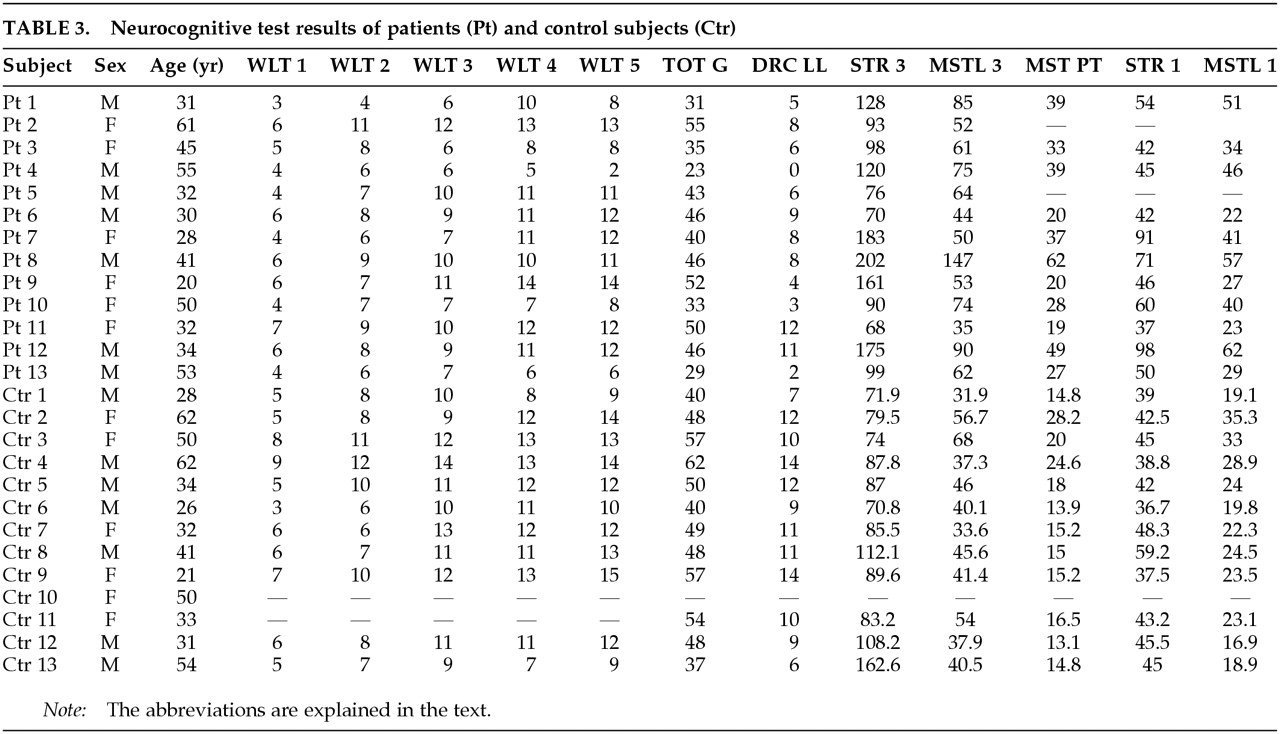
The neurocognitive data used to derive the combined
z-scores are presented in
Table 3. The combined ratings for memory resulted in a
z-score of –1.07 (SD=0.98) for the patients and 0.03 (SD=0.93) for the control subjects. The
z-scores for sensorimotor and cognitive speed were –4.45 (SD=3.59) and –2.60 (SD=2.83) for patients and –0.32 (SD=0.71) and –0.16 (SD=0.73) for control subjects. The results of the two groups were significantly different on all three cognitive domains (memory:
t=2.82, df=22,
P=0.01; cognitive speed:
t=2.9, df=21,
P=0.009; sensorimotor speed:
t=3.18, df=16,
P=0.006).
Lesions
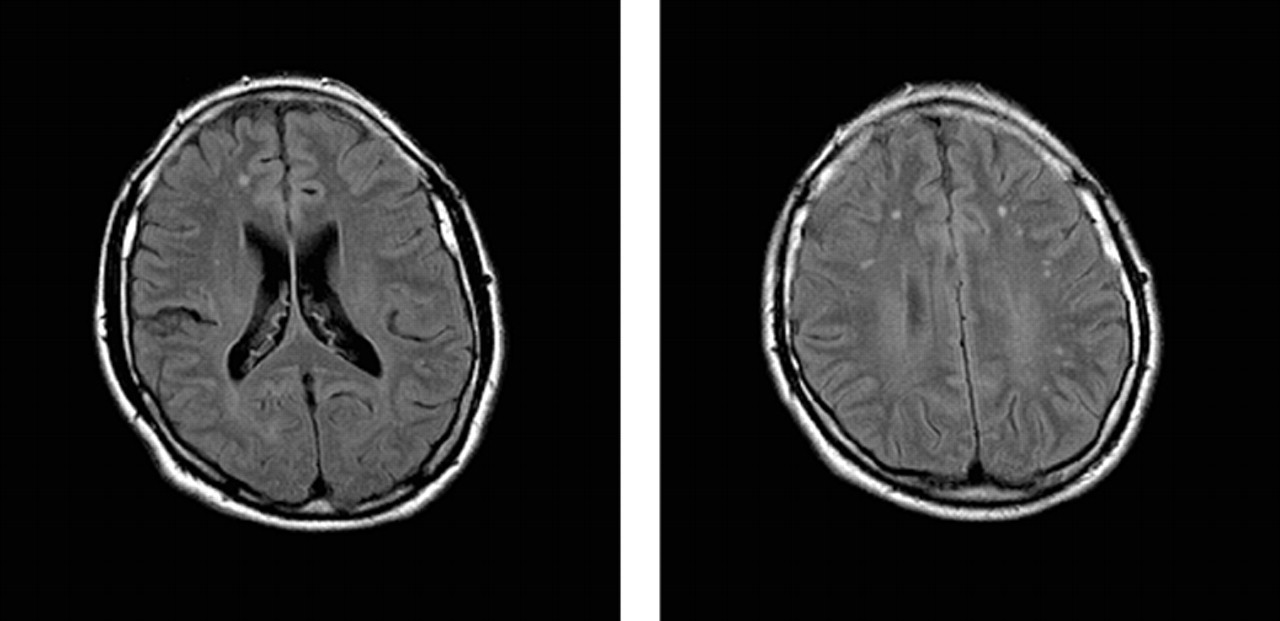
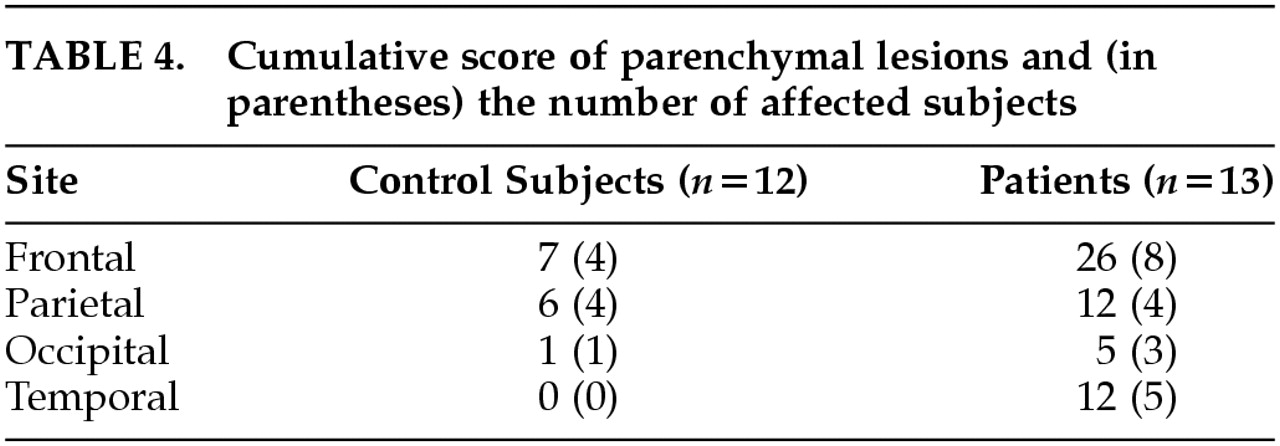
The analysis of lesions focused on the frontal, temporal, occipital, and parietal lobes. There were too few lesions in the subcortical gray matter and the infratentorial brain to make any inference. In one patient, only the MTI sequence was performed and thus there was no information available about parenchymal lesions. The T
2-weighted FFE sequence showed no hemosiderin depositions. The cumulative scores for the different regions showed the frontal–temporal region to be affected most often (
Table 4 and
Figure 1). The median scores for parenchymal abnormalities in the patient and control groups were 3 and 1, respectively; this difference was significant (Wilcoxon signed-ranks test,
z=–2.25,
P=0.02). The lesion load in patients is therefore higher than in the control group. Patients had a higher prevalence of parenchymal lesions than control subjects (77% vs. 38%; χ
2=3.38, df=1,
P=0.066), but this did not reach statistical significance. To assess the effect of age on the volume of parenchymal lesions, the data for the patients and control subjects were combined in an analysis of variance. There was a significant main effect of patient versus control (df=1,
F=14.857,
P=0.001), and an independent effect of age (df=2,
F=9.086,
P=0.002). There was also a significant group by age interaction (df=2,
F=4.467,
P=0.026).
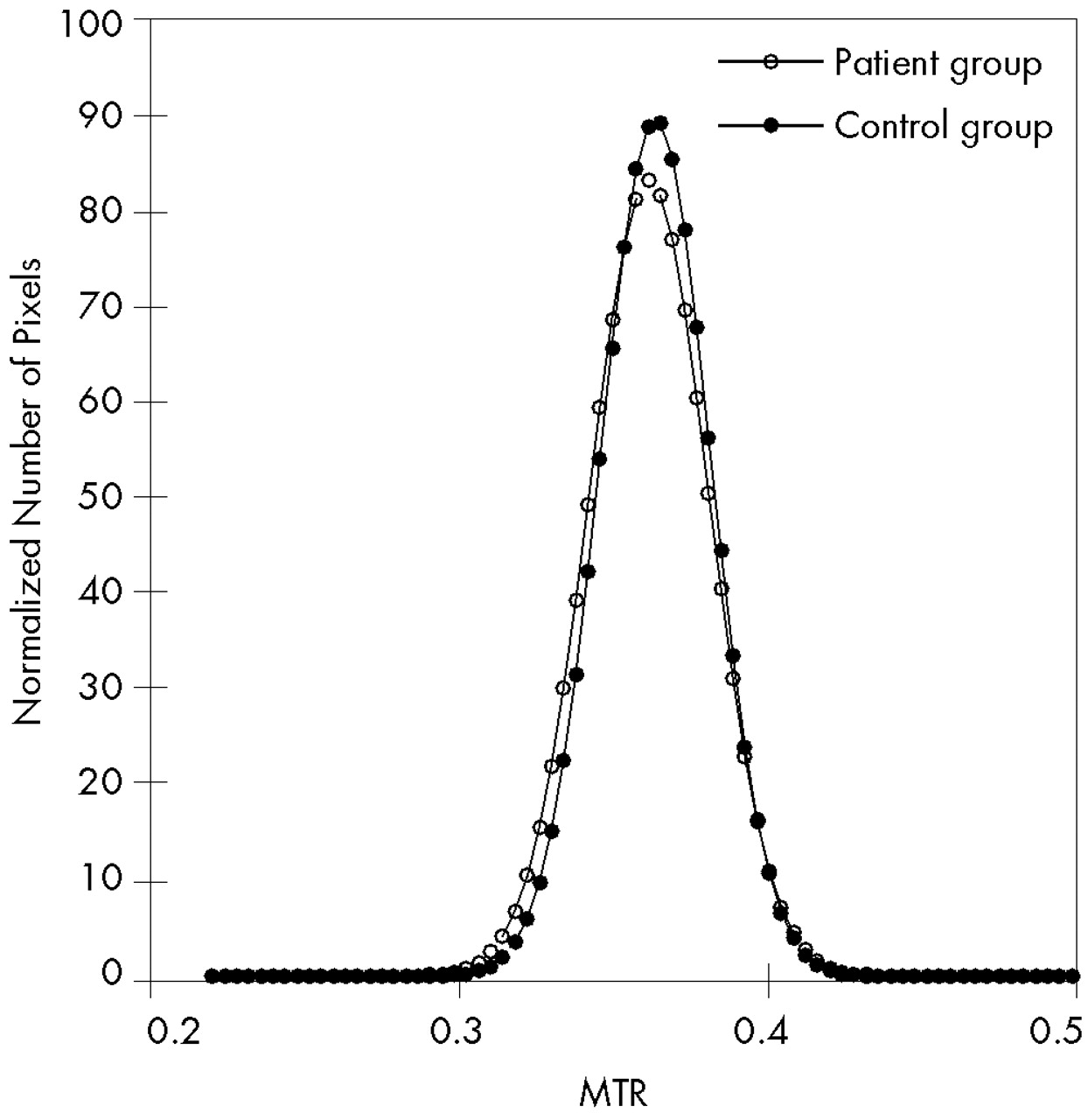
Magnetization Transfer Data
The mean histograms for control subjects and patients are shown in
Figure 2. The curve amplitude of the white matter histogram was 83.28 for the patients and 89.76 for the control subjects (
Table 5). This difference was statistically significant (
t=2.95, df=24,
P=0.007). The width also differs significantly between the two groups, but after histogram normalization it contains the same information as the amplitude. The mean MTR for the patients is lower than for the control subjects, but this difference is not significant.
Interaction With Neurocognitive andClinical Parameters
There was no correlation between neurocognitive parameters and the lesion volume or the histogram parameters (
Table 6). There was a significant correlation between the lesion volume and the duration of unconsciousness (Pearson correlation coefficient 0.63,
P=0.038), and the correlation with duration of posttraumatic amnesia is near significance (Pearson correlation coefficient 0.61,
P=0.06).
DISCUSSION
The main finding of our study is an increased lesion load in patients one year or longer after a mild to moderate traumatic brain injury, as evidenced by the lesion load, as well as a significant decreased curve amplitude of the MTR histogram in patients with postconcussional symptoms as compared with matched control subjects. Even in a small group of only 13 patients, these differences were significant. This finding is of importance because it is the first MRI study to provide evidence for an organic etiology of a postconcussional disorder. Jacobs et al.
39 showed a correlation between posttraumatic cognitive complains and SPECT findings, but their patients were studied within one year after the trauma, whereas one year was the shortest interval in the present study.
The application of new imaging techniques has shown beyond doubt that mild head injury may lead to brain injury in a much higher percentage than previously thought. In a group of mTBI patients with a negative CT, Mittl et al.
14 found 30% abnormal MRI studies, and another study of unselected mTBI patients showed that 77% of the patients had abnormal findings on MRI or SPECT imaging of the brain.
40 Even CT reveals hemorrhagic lesions in up to 10% of mTBI patients.
41 We provide data that these lesions may persist and are associated with persistent symptoms.
There has been continuous debate on the organic or psychogenic etiology of a postconcussional disorder, and it has become clear that other factors do influence the outcome after a mTBI.
42–45 Secondary gain and psychosocial factors are important in the etiology of a postconcussional disorder. Clearly, a balanced integrative neuropsychiatric approach is warranted, taking into account all biological, psychological, and environmental factors and their mutual interactions. Because previous imaging showed no abnormalities, it was very difficult to test the hypothesis of brain lesions as an explanation for a postconcussional disorder. However, the current study has added the factor organic brain damage as an etiologic factor for a postconcussional disorder. A prospective study with a larger, unselected sample including patients with mTBI but no complaints is needed to confirm our findings and to establish causality between a postconcussional disorder and traumatic brain lesions.
Demyelination, edema, and posttraumatic changes decrease the MTR,
19,20,22 causing a shift toward the left and flattening of the histogram peak. The decreased curve amplitude of the MTR histogram of our patients can therefore be explained by the existence of macroscopic and microscopic lesions. It appears that the curve amplitude is more sensitive to cerebral changes than the mean MTR, since the decreases in the mean MTR were not significant. Histopathologically these lesions are most likely areas of focal axonal loss, demyelination, and astrocytosis.
46 Animal studies have shown that mTBI causes mitochondrial swelling, edema, and subtle axonal damage in the absence of gross focal lesions, contusions, or laceration.
10,47 This has also been shown in patients who died of a non–CNS-related injury shortly after a minor head trauma.
9 The MTR analysis is also more sensitive to cerebral changes than the analysis of the focal lesions. A post hoc analysis shows that after excluding the two subjects with the longest posttraumatic amnesia, reducing the range to 0–48 hours, the difference between patients and control subjects remains significant for the curve amplitude but becomes nonsignificant for the focal lesions.
Our analysis of focal lesions shows that patients with a postconcussional disorder have a higher lesion load than matched control subjects, and that these lesions are mainly located in the frontal and temporal regions. This last finding is in agreement with previous studies.
48–51 The prevalence of focal lesions in our patient group is 77% as compared with 38% in the matched control group. This is high considering the time elapsed between the trauma and imaging. Parenchymal lesions decrease in size and number after the trauma, especially during the first 3 months.
51 MRI studies performed shortly after mTBI show a prevalence of abnormalities ranging from 30% to 77%, depending on the patient selection and scanning technique.
14,51,52 The present patient population comprised individuals with a DSM-IV-classified postconcussional disorder with neurocognitive complaints who presented at a university-based memory clinic. This strong selection bias might explain the relatively high prevalence of frontal-temporal lesions. Even though the control subjects had a prevalence of 38% of parenchymal lesions, the patients had both a higher prevalence and a higher lesion volume. It is an interesting finding that differences between patients and control subjects were larger in the older population, as demonstrated by the significant group versus age interaction in the analysis of variance. This finding illustrates the increased vulnerability of the aging brain.
Although lesions were located most predominantly in the frontal and temporal lobes, the size and precise location differed considerably among patients. This heterogeneity is most probably due to differences in trauma mechanisms. The neurocognitive data also showed a heterogeneous image; different cognitive domains were more or less severely affected. It is likely that there is an association between the site of the lesions and the neurocognitive deficit. Levin et al.
51 showed an association between lesion location and performance on memory and planning tasks in a group of head injury patients. The majority of patients in that series, however, had sustained moderate head injury. The heterogeneity of both organic lesions and neurocognitive deficits may explain why an association between these was not demonstrated. Posttraumatic amnesia and loss of consciousness are global measures of traumatic brain injury and are known to correlate with the extent of brain injury.
53 Therefore, our finding of a correlation between these two measures and the lesion volume is in support of a traumatic origin of the brain lesions.
Our results cannot be extrapolated to all patients with postconcussional symptoms without due consideration. Although we carefully matched for age and education, and excluded patients with concomitant injuries and neurologic or psychiatric disorders, we cannot exclude the effect of other confounding factors, such as litigation.
Interestingly, recent evidence from experiments with healthy individuals who had sustained mTBI a long time ago shows that these subjects suffer from impaired cognitive functioning compared with that of healthy subjects who had not sustained traumatic brain injury.
28,54 This finding suggests that mTBI may have long-term subclinical effects that become apparent upon neurocognitive testing. It is tempting to hypothesize that these subtle dysfunctions are due to changes in brain structure similar to those found in our patient group.
CONCLUSIONS
This study provides evidence of posttraumatic brain alterations in patients who sustained a relatively mild traumatic brain injury one or more years before presentation with cognitive complaints at a memory clinic. Our results support the hypothesis of an at least partially organic etiology for postconcussional symptoms in these patients; however, more study is needed to establish causality between a postconcussional disorder and traumatic brain lesions. We are currently carrying out a prospective study to investigate this matter further.
Histogram analysis of MTR data seems a useful method for the detection of diffuse brain injury. The method has the potential to detect macroscopic as well as microscopic lesions and, like every automated analysis, is less prone to observer variation.