F oreign accent syndrome is a disorder of speech output characterized by the emergence of phonetic and phonemic contrasts in an individual’s speech that result in a listener’s perception of the speech as foreign. Approximately 20 cases
1 –
17 have been reported with a variety of accents described. Almost all have occurred subsequent to a lesion in the dominant hemisphere. Many cases have involved mild aphasia or dysarthria. Usually the accent is one to which the patient has not been exposed in the past, although the emergence of a previously learned accent has been described in two patients.
13,
15 Foreign accent syndrome is often persistent but can be transient.
CASE REPORTS
Case 1
A 30-year-old man with a 10-year history of schizophrenia was hospitalized after he stopped taking his medication (olanzapine, 20mg q.h.s.) and developed bizarre behavior. His thought processes were disorganized with looseness of associations. He expressed a variety of grandiose delusions and believed that he had graduated from several universities and could speak several ancient languages, including Greek and Latin. He denied having auditory or visual hallucinations.
His speech was minimally pressured with a melodic “sing-song” accent. He often dropped consonants, such as “d,” from the ends of words (e.g., “fren” for “friend”). Several staff members believed that he sounded Jamaican. The accent was present at all times, including during casual conversation with other patients. There were no other abnormalities of speech or language. He scored 60/60 on the Boston Naming Test. He acknowledged an awareness of the accent and stated that he had grown up in Alabama and had a Southern accent until he acquired the new accent while undergoing training in classical Greek. In reality he had had no such training. Medical history was unremarkable.
Treatment with olanzapine was resumed. Over the first 5 days of hospitalization the accent persisted as did his delusional thinking. On the sixth day the accent resolved. At that point his delusions remained present but were less severe. Olanzapine was continued, and over the next 9 days his thought processes became more organized and his delusions less prominent. He was discharged on the fourteenth day of hospitalization.
Case 2
A 53-year-old woman with a 30-year history of bipolar disorder was hospitalized after threatening her husband with a baseball bat. She had not been taking her medications for several months and had taken two impulsive trips that had lasted several days. After returning from the second trip, she was very energetic, delusional, and sleeping only a few hours per night. A few days later she felt that her husband was plotting against her and threatened him.
Examination revealed an elevated mood with racing thoughts and looseness of associations. She admitted to having auditory hallucinations and related paranoid delusions of people spying on her and trying to have her incarcerated. She believed she had secret siblings that her parents had hidden from her and that she was a genius.
Staff noted that she spoke with an accent that they perceived as “European.” She spoke with a rising inflection at the end of phrases and sentences. She often omitted final consonants, particularly “t” (e.g., “leh” for “let”). Her speech was grammatically correct and she had no difficulty with comprehension, repeating phrases, or word finding. She scored 60/60 on the Boston Naming Test. She was not aware of an accent. When asked, she said she might have one because she was fluent in eight languages and would demonstrate her abilities by speaking what was actually gibberish. Her accent was consistently present regardless of situation.
She had no history of medical problems. She initially showed poor response and ultimately required treatment with a regimen of valproic acid, 1500mg, olanzapine, 20mg, and lithium carbonate, 900mg per day. After 15 days, we noted a decrease in the severity of her delusions and she started to lose the accent. The next day it was barely detectable and the day after that it was completely absent. Delusional behavior, although not as severe, was still present and she could not be discharged until 11 days later.
Case 3
Described below are three episodes of psychosis and foreign accent syndrome in a single individual. The patient had a history of schizophrenia beginning in his early thirties and had been noted on several occasions to have what was perceived as a British accent during episodes of psychosis. Speech was fluent and grammatically correct with no evidence of aphasia or impaired comprehension. He scored 58/60 on the Boston Naming Test. Vowels were often elongated, particularly the “a.” Substitution of vowel sounds included “ei” for “ai” such that “daily” was pronounced “dyly,” and “ah” for “ou” such that “about” was pronounced “abaht.” Consonant variation included substitution of “f” or “v” for “th.” He had lived in the United States his entire life except for 2 years as a soldier in Korea. He was difficult to manage and had been on various medications at different times. At age 66 he had to be placed in a nursing home because his wife could no longer care for him. His medical history included well-controlled hypertension and Parkinson’s disease.
First Occurrence
The patient was admitted from his nursing home where he had apparently been cheeking his medications (quetiapine and carbamazepine) and decompensated. He was hallucinating and delusional, with beliefs that he was in contact with spaceships, surrounded by “legions of angels,” and that several people he knew were the devil. He attached great significance to his middle name being George because that was the name of several kings. Paranoid delusions were expressed and at times he was irritable and agitated.
A prominent accent which multiple independent observers perceived as British was present at all times. The patient was aware of it and stated it was British. He often incorporated British terms into his vocabulary (e.g., “blokes”). He justified his accent by claiming a connection with British royalty and culture.
He was treated with a regimen of carbamazepine, 200mg t.i.d., and risperidone, with 3mg b.i.d. required to affect his psychotic symptoms. Only after about 4 weeks of treatment did he begin to demonstrate improvement of his psychosis and resolution of the accent. Even after disappearance of the accent, grandiose delusions persisted, although not nearly as severe as previously. The agitation and irritability resolved.
Second Occurrence
About 2 years later, the patient had to be readmitted after he became loud and threatening toward staff at his nursing home. The accent was again noted to be consistently present. He was hallucinating and expressed paranoid and grandiose delusions. He believed he had been split into three parts, one of which resided in Buckingham Palace. He often talked of being influenced by spirits.
During this admission he was treated with a regimen of valproic acid, 250mg t.i.d., and olanzapine, 15mg q.h.s. Over the next 9 days, the accent lessened and then disappeared, as did the hallucinations. The delusional symptoms improved but did not fully resolve. His agitation markedly improved, and he reached the point where he was pleasant and interactive.
Third Occurrence
Six weeks later the patient again exhibited psychotic symptoms, apparently after again cheeking his medications. The accent returned and was consistently present. He expressed grandiose delusions about being able to travel through time and having an important role in English history. He believed he was in telepathic communication with a local radio station.
Administration of valproic acid and olanzapine under close supervision was resumed. His delusions lessened and the accent gradually resolved. It was completely absent after 9 days of treatment.
For each of these three patients, there was no significant history of alcohol or drug abuse. None of the patients had ever been directly exposed to the accent they developed. All patients were native English-speaking Americans.
Patient Characteristics When Accent Present and When Absent
Each of the episodes described above was observed in hospitalized patients. For each patient, a complete assessment was performed, including physical examination, laboratory workup, magnetic resonance imaging (MRI), and electroencephalography (EEG). On the day of admission a Global Assessment of Functioning (GAF) rating
18 was determined in each case and a Positive and Negative Syndrome Scale (PANSS)
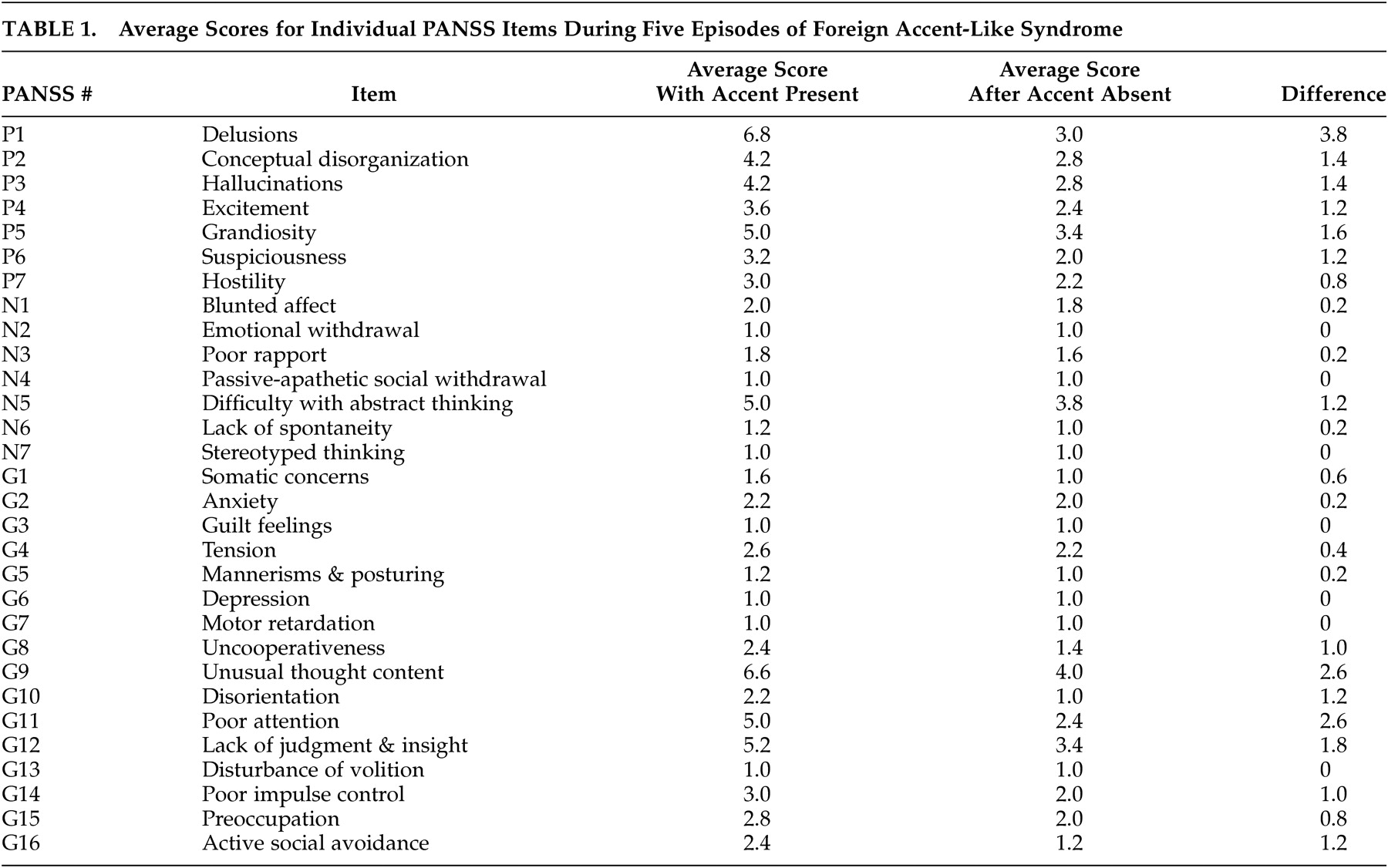
19 administered. The PANSS is a 30-item clinician-administered instrument that assesses the severity of psychiatric symptoms commonly observed in psychotic disorders, with a seven-point rating scale from 1 (absent) to 7 (extreme) for each item. Seven items constitute a Positive Scale, seven a Negative Scale, and the remaining 16 a General Psychopathology Scale (
Table 1 ). Items are summed to yield subscale scores and a total score, with higher scores indicating a greater severity of symptoms. Subtracting the Negative Scale score from the Positive Scale score yields a Composite Scale score with a bipolar index ranging from −42 to +42. A PANSS-derived psychotic symptom item score may be derived from the scores for eight items often associated with psychosis (delusions, conceptual disorganization, hallucinations, grandiosity, suspiciousness, somatic concern, guilt, and unusual thought content).
20Each patient was treated in the hospital as described above. The status of the foreign accent was monitored daily. Three days after complete resolution of the foreign accent, administration of the PANSS was repeated and the GAF was reassessed.
RESULTS
Physical examination, laboratory studies, MRI, and EEG for these patients were generally unremarkable. Single photon emission computed tomography (SPECT) and positron emission tomography (PET) scans could not be obtained. For all of the episodes combined, the average score for each individual item of the PANSS with the accent present and absent are shown in
Table 1 .
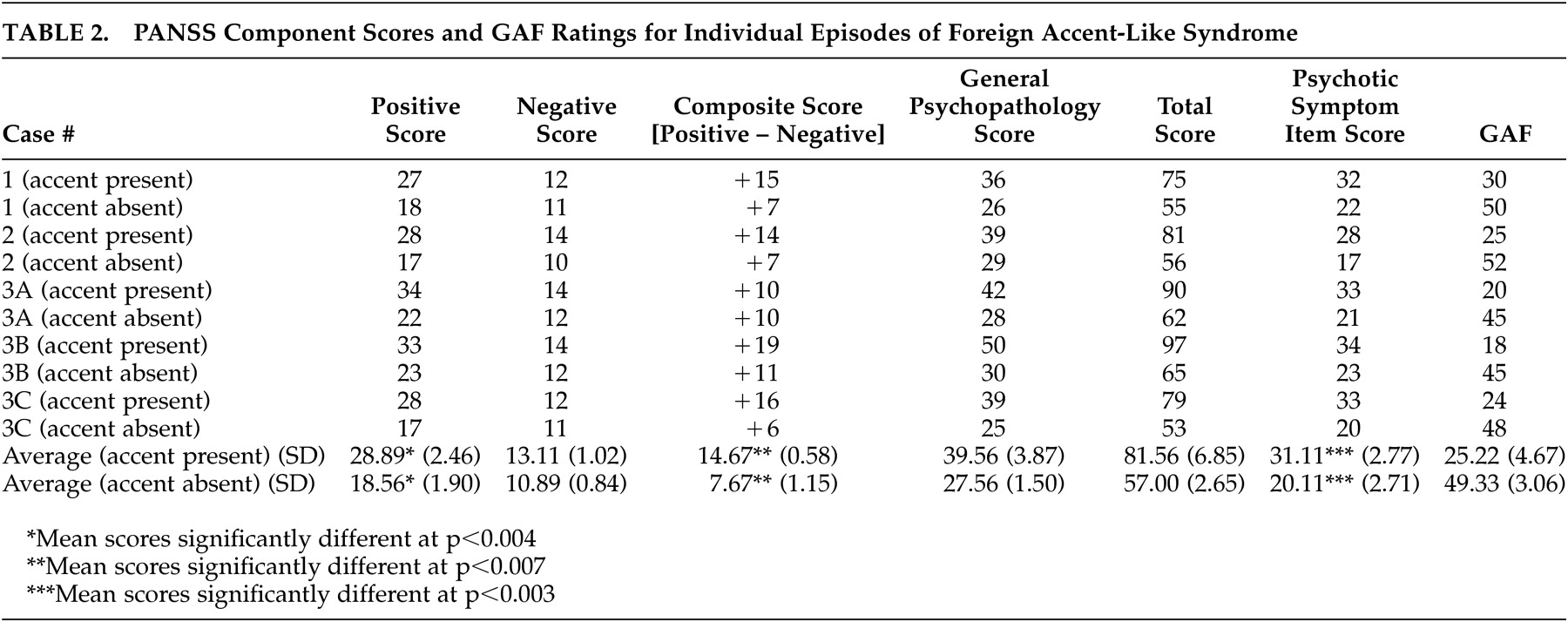
Table 2 shows the PANSS component and GAF scores for the individual episodes and averages for the episodes combined with the foreign accent present and later when absent.
To examine changes in patients’ psychotic symptoms when a foreign accent was present versus absent, a series of paired sample t tests were run on the scores of the PANSS subscales, the total PANSS score, and the GAF score. To address issues of autocorrelation introduced by the fact that three of five observations were from the same patient, t tests for Case 3 used the mean scores across the three admissions for that patient. To control for type I error rates associated with multiple comparisons, the Bonferroni correction was applied and only tests that were significant at p<0.007 (0.05/7.00) were considered reliable.
Consistent with the expressive nature of producing speech with a foreign accent, a paired sample t test run on the PANSS Positive Symptoms subscale score was significant T (1, 2) = 15.50, p<0.004. This finding indicates that patients demonstrated more severe positive symptoms (e.g., excitement, grandiosity) when a foreign accent was present versus absent. Similarly, paired sample t tests run on patients’ PANSS Psychotic Symptom Subscale score, T (1, 2) = 19.053, p<0.003 and Composite Scores, T (1, 2) = 12.12, p<0.007 were also significant, suggesting that when a foreign accent was present, patients demonstrated a greater degree of psychotic symptoms compared to when the accent was absent. Further, the significant Composite Score indicates that the magnitude of the difference between patients’ positive and negative symptoms is greater when they demonstrate a foreign accent.
Paired sample t tests run on the patients’ Negative Symptom, General Psychopathology, and Total Symptom Scale Scores were not significant (p>0.007). A paired sample t test run on the patients’ GAF scores closely approached, but did not achieve, significance (p<0.008).
DISCUSSION
Most previously reported cases of foreign accent syndrome have occurred subsequent to a brain lesion identifiable by conventional neuroimaging. Moonis et al.
15 described a patient who had no abnormalities on MRI but did have perfusion deficits with SPECT. Locations of the lesions producing foreign accent syndrome have been somewhat variable but usually have involved an area involved in speech production, including precentral gyrus, premotor mid-frontal gyrus, left subcortical prerolandic and postrolandic gyri, and left parietal area.
14 However, a recent case with a French accent resulted from an infarction in the body of the corpus callosum, a structure not directly involved in the production of speech.
18 Many cases have involved some degree of aphasia or dysarthria, although Takayama et al.
13 described a case without either. Thus, the mechanism of production of the syndrome is unclear and, in fact, a variety of different lesions or factors may be involved in producing the accents. No identifiable structural lesion or deficit of language production or articulation was present in the psychotic patients described here, suggesting that a lesion, if present, was one of brain function (e.g., neurochemical or electrical) as opposed to brain structure.
In each of our cases the foreign accent gradually disappeared while the psychotic symptoms lessened, as evidenced by the improvement of overall PANSS scores and GAF as the accent resolved. The PANSS items showing the greatest changes (more than 1.5 points pre- and posttreatment) were delusions, unusual thought content, poor attention, lack of judgment and insight, grandiosity, conceptual disorganization, and hallucinations. These items make up six of the eight items used to determine the psychotic symptom item score. Thus, it is not surprising that scores from this scale were decreased at a highly significant degree. It may be seen that the foreign accent was more likely to be present when psychotic symptoms were worse, particularly positive symptoms, such as delusions, hallucinations, and disorganized thinking. Why this would occur is unclear. Language dysfunctions in schizophrenia are often characterized by derailment and disorganization, and bipolar patients may exhibit extravagant or flippant elaborations and intrusions in speech. The severity of language dysfunction in schizophrenia correlates with the severity of overall symptoms of the disorder, suggesting that disordered speech in psychotic patients is not just due to a speech disorder but is part of a broader constellation of psychotic symptoms.
21,
22 However, changes in intonation or accents are not common in these patients and do not appear to be the same phenomenon.
Functional neuroimaging techniques, especially PET and fMRI, have been used to reveal areas of the brain involved in speech production. The dominant hemisphere contains an organized network for language function. Electrical impulses for word-intrinsic word generation are initiated in the dorsolateral prefrontal cortex (DLPFC) and transmitted to the superior temporal gyrus (STG) in Wernicke’s area. From there, information is transmitted forward to Broca’s area which initiates a motor plan that is transmitted to the primary motor cortex to pronounce the words. Functional imaging studies are being used to examine changes in brain activation patterns that occur after onset of aphasia from strokes and during recovery (the right hemisphere is active during recovery and activity may be more bilateral than previously thought)
23 and to assess language disorders related to primarily functional etiologies (dyslexia with findings for the posterior temporal and adjacent occipital and parietal areas;
23 stuttering with cerebral blood flow increased in the right anterior insula and decreased in right Brodmann’s area 21/22 and in an area within the left inferior frontal gyrus
24 ). Because of its multiple functions (e.g., linguistic, attitudinal, affective) and its multiple phonetic cues (e.g., pitch, duration, loudness), the neural substrate of speech prosody remains elusive and controversial with parts of both hemispheres hypothesized to contribute to the final production of prosodic words.
25 For example, PET studies have shown that pitch in linguistic and nonlinguistic contexts, respectively, activates homologous, inferior frontal regions in both the left and right hemisphere.
26 Thus, the brain areas leading to dysprodic speech under a given condition may be difficult to clearly specify. It is likely that in the future, linguists will switch from the idea of hemisphere dichotomies processing speech prosody to that of the development of neural networks subserving speech prosody.
One possible hypothesis to explain the occurrence of foreign accent with psychosis could be that whatever activates positive psychotic symptoms also precipitates the accent. In normal patients, word generation activates the DLPFC and causes deactivation of the bilateral STG.
27 Failure of deactivation of the left STG in the presence of activation of the left DLPFC has been reported to occur in schizophrenia.
28 It appears that left STG dysfunction is related to the actual presence of psychotic symptoms and is not present in asymptomatic patients with schizophrenia and bipolar disorder.
29,
30 This phenomenon may be indicative of a functional disconnectivity between the left DLPFC and the left STG during active psychosis, and this could contribute to the development of a foreign accent-like syndrome in psychotic patients. Another possible hypothesis that might explain the intermittent occurrence of an accent during exacerbations of psychosis could be related to intermittent emergence of suppressed neural circuitry. In this scenario, the normally suppressed circuitry capable of producing speech abnormalities would become active during psychotic exacerbations and again suppressed with control of the psychosis.
The nature of the interaction of the patients’ psychosis and foreign accents is unclear, but there does appear to be a degree of correspondence between them. Certain delusions (e.g., being trained in several ancient languages) might contribute to the development of an accent. On the other hand, it is conceivable that having a speech pattern suggestive of an accent could lead to delusions that would attempt to explain the presence of the accent. A recent report
31 describes a patient who echoed different accents while she was psychotic but not after her psychosis resolved. Because it has been described by two different groups, the occurrence of foreign accents during psychosis, although rare, appears important enough to warrant additional investigation.
A number of questions remain unanswered regarding the occurrence of foreign accent syndrome during psychotic episodes, including its pathogenesis, relationship to the foreign accent syndrome described in the neurological literature, and what clinical implications its presence might have. It would have been desirable to obtain functional neuroimaging in our patients. Further investigation should include PET or fMRI of patients with active symptoms of the syndrome present and later when absent to determine the exact cerebral areas activated in association with the accent. Ultimately, foreign accent syndrome remains a rare and poorly understood phenomenon that requires additional examination. When noted by other clinicians, further reports of the condition should be encouraged in order to definitively describe and characterize the phenomenon.