T he capacity of patients with serious mental illnesses to consent to research and treatment has been widely debated and has been the subject of national recommendations regarding the protection of human subjects.
1,
2 Studies find that while, on average, schizophrenia patients’ ability to understand, appreciate, and/or reason with information in a consent form is poorer than that of healthy comparison subjects,
3 –
7 there is considerable heterogeneity in patients’ consent-related decision-making abilities. Some of the variability is likely a result of situational factors, but trait factors, such as individual differences in cognitive ability, also appear to be strongly related to decisional capacity.
3,
5 –
9 Less evidence exists, however, for the idea that particular neurocognitive domains (such as attention/working memory, episodic learning/recall, or executive functions) may be differentially related to specific elements of consent-related decision-making. Such a “cognitive model of decisional capacity” has been suggested for Alzheimer’s disease patients,
10 and may be applicable to patients with schizophrenia.
The few published studies that have used a comprehensive neuropsychological battery to examine support for this idea
5,
9,
11,
12 have found evidence for a general relationship between cognition and capacity to consent, but less evidence for specificity. Palmer and Jeste
11 suggest that the use of clinical neuropsychological measures, which often rely on multiple information processing domains within a single test, may make it difficult to detect the relationship of particular domains with elements of consent-related capacity. It has been argued that functional neuroimaging is a more sensitive measure of individual differences among patients with schizophrenia than behavioral measures (e.g., in the realm of genetics).
13 Thus, functional imaging may be a better tool for examining sources of variability in decisional capacity than neuropsychological measures alone.
In this study, we measured decisional capacity using a well-validated instrument, the MacArthur Competence Assessment Tool for Clinical Research (MacCAT-CR). We focused on understanding and reasoning abilities because of the greater degree of measurement reliability and subject variability in these subscales compared with the appreciation and expression of choice subscales.
8 We postulated that two crucial neurocognitive systems underlie some of the observed deficits in understanding and reasoning among patients with schizophrenia. Understanding of consent-related information presumably requires both encoding and retrieval of information about study procedures. Episodic learning and retrieval deficits are prevalent among individuals with schizophrenia,
14,
15 and functional neuroimaging studies have found inferior frontal and medial temporal brain abnormalities during encoding and retrieval among patients.
16 –
21 Reasoning is usually assessed by asking participants to make mental comparisons between potential consequences of participation (including possible adverse effects) and therefore, like a working memory task, would seem to require simultaneous manipulation of information. Working memory abilities are frequently disrupted in schizophrenia,
22 and dysfunction of the dorsolateral prefrontal cortex consistently has been implicated in these deficits.
23 –
25 Thus, we postulated that performance on measures related to the understanding of consent-related information would be associated with medial temporal and inferior frontal brain function, whereas reasoning would be related to brain response of the lateral prefrontal cortex (i.e., middle frontal gyrus). We chose to measure brain response during a verbal learning task because of its relevance to the consent process, and because it would likely challenge both medial temporal and frontal brain regions. We studied middle-aged and older patients because of the increased risk of cognitive deficits that may impair decisional capacity in this population.
26We hypothesized that the functional magnetic resonance imaging (fMRI) response of patients with schizophrenia in the medial temporal and inferior prefrontal cortex would correlate positively with MacCAT-CR understanding scores, whereas lateral prefrontal brain response (i.e., in the middle frontal gyrus) would positively relate to reasoning scores.
METHOD
Participants
We recruited 24 community-dwelling outpatients with a DSM-IV-based
27 diagnosis of schizophrenia consecutively from Board-and-Care homes in San Diego county, Calif. Following an assessment of decisional capacity, five patients were deemed incapable of giving informed consent for the functional imaging study. Scanning was not completed in three additional patients, and data were not usable for another two patients due to excessive motion during the scan. Therefore, data were available for 14 schizophrenia patients.
Assessment of Decisional Capacity
The study was approved by the University of California, San Diego, Institutional Review Board. After presenting consent information for the fMRI study, “Understanding” and “Reasoning” were assessed using a version of the MacCAT-CR
28 tailored to the consent form for the present, nonhypothetical study. Participants were required to achieve a criterion score of at least 16 out of 26 correct
12 on the Understanding portion of the MacCAT-CR (the standard used in a large-scale national clinical trial)
29 in order to be considered capable of giving informed consent. If this was not achieved after one presentation of the consent form, up to two additional presentations of all consent information were made (differing from standard MacCAT-CR protocol, which calls for only one repetition of misunderstood information). Reasoning was assessed only after the first administration of the consent information, consistent with the recommendations of the MacCAT-CR manual.
28Functional Imaging
Behavioral Task
Participants were presented with 32 pairs of associated nouns and instructed to learn “how they go together” for later testing. Half of the pairs were novel and half were familiar as they had been previously presented prior to scanning. Word-pair learning trials were presented in blocks of four trials each, interspersed with blocks of fixation of varying length. Each learning trial lasted for 5 seconds, and participants indicated with a button-press which of the words was capitalized, as a check that they were processing each stimulus. The following measures of performance were assessed: accuracy of indicating capitalization (during scanning) and post-scan cued-recall accuracy.
Scanning Procedure
Participants were scanned in a 1.5T Siemens Vision MRI scanner. Blood-oxygen-level-dependent (BOLD) response during the task was assessed with gradient-recalled echoplanar imaging (EPI) sequence (69 whole-brain images of 32 axial slices, 4 mm thickness, 4×4 mm in-plane resolution, TR=4000 msec; TE=40 msec; flip angle=90°). High-resolution anatomical images were acquired using the magnetization-prepared rapid acquisition gradient echo (MPRAGE) protocol (sagittal slices, 1 mm thickness, 1×1 mm in-plane resolution, TR=11.4 msec, TE=4.4 msec, flip angle=10°).
In all but two participants (whose Run 2 data were excluded due to excessive motion), imaging and behavioral data from two consecutive runs of the verbal learning task were averaged to increase the power of the paradigm.
Image Analysis
Images were analyzed using the AFNI software package.
30 Functional images were aligned across the image time series; time points with remaining visually observable movement after use of the automated algorithm were discarded. Registration between functional and anatomical images was inspected visually and, when necessary, rotated or translated manually into alignment. The time-dependent BOLD signal was modeled using regression with a combination of the following variables: reference vectors representing the occurrence of different stimulus types (i.e., Word pairs or Fixation) convolved with a gamma-function model of the hemodynamic response, motion parameters, a linear trend, and a constant. The magnitudes of the fit coefficient for the general linear contrast in signal intensity (controlling for the other parameters in the model) between Word pairs and Fixation were used as the dependent variables for further analysis. Fit coefficient maps were transformed into standardized atlas space
31 and blurred with an 8 mm FWHM Gaussian filter (for Talairach region of interest [ROI] and whole brain analyses) or left unblurred (for the hippocampal ROI analysis). The fit coefficient maps were then averaged across the two paired-associates learning runs.
Statistical Analyses
Two approaches were utilized to examine our hypotheses regarding the relationship between learning-related brain response and MacCAT-CR performance.
Region of Interest (ROI) Analysis
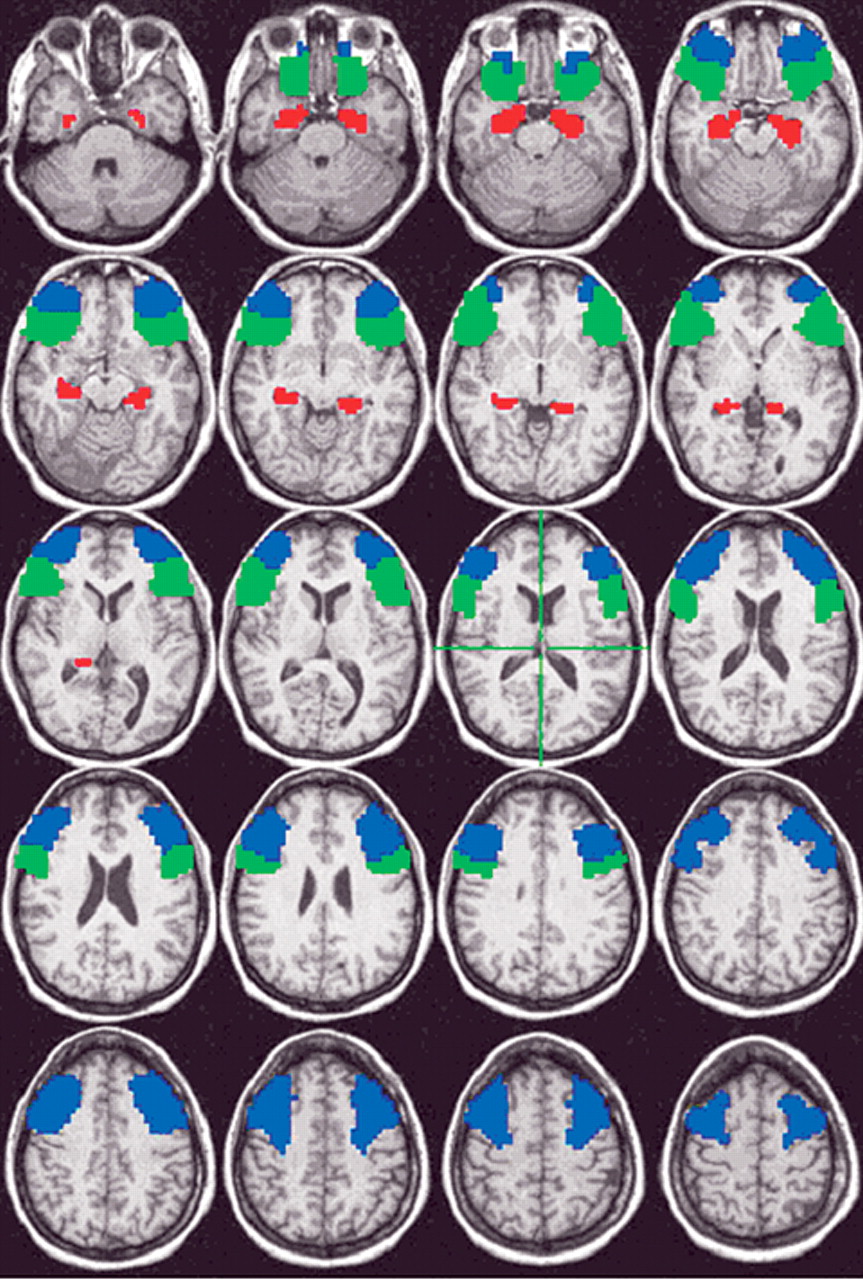
We calculated the mean learning-related brain response in three bilateral ROIs (
Figure 1 ). Inferior frontal gyrus and middle frontal gyrus ROIs were drawn using the AFNI program DrawDataset, which uses information from the Talairach Daemon software.
32 Following the guidelines of Insausti et al.,
33 hippocampal ROIs were hand-traced on each participant’s high-resolution anatomical MR image by two experienced technicians, who achieved >90% agreement on a reliability set of images. The mean fit coefficient in both hemispheres of each ROI was calculated and used in the correlation analysis with MacCAT-CR scores. Pearson’s correlations were used, and considered significant at a two-tailed p≤0.05. Given the exploratory nature of the study and small sample size, no correction for multiple comparisons was made.
Whole Brain Analysis
To see whether other, unhypothesized relationships might be found, the correlation between MacCAT-CR scores and brain response was carried out at each voxel in the entire brain. Clusters of correlated voxels were then identified with the criterion (determined by Monte Carlo simulation) that each significant cluster had to contain at least 160 contiguous voxels, each with a significant correlation (p<0.05). This protected a whole-brain probability of false positive cluster detection of p=0.05.
RESULTS
Participant Characteristics
Patients were middle-aged (mean=44.1 [SD=10.0] years old), high-school educated (12.9 [SD=1.3] years) and predominantly male (93% [N=13]), with a chronic course of illness (duration=22.0 [SD=9.1] years) of moderate severity (PANSS Positive score=10.3 [SD=3.6]; PANSS Negative=14.1 [SD=5.8]; PANSS General=24.2 [SD=5.6]). All were being treated with medications, predominantly with atypical antipsychotics (43% [6] olanzapine, 28% [4] risperidone, 21% [3] other atypicals, 8% [1] typical antipsychotics). Most of the patients were of the paranoid subtype (78% [11]), with the others of the disorganized (14% [2]) or undifferentiated subtypes (8% [1]).
Decisional Capacity
The scores of patients on the Understanding and Reasoning sections of the MacCAT-CR (Initial Understanding [out of 26]: 14.4 [SD=3.8], Trials to Criterion [out of 3]: 1.9 [SD=0.8], Final Understanding [out of 26]: 17.8 [SD=1.7], Reasoning [out of 8]: 6.3 [SD=1.6]) were in the range expected based on previous studies of decisional capacity among patients with schizophrenia.
4 Given that in practice, consent information is generally only presented once, Initial Understanding was used in subsequent analyses.
fMRI Task Performance
Patients were attending well to the stimuli during the scan, as indicated by high accuracy of judgment of capitalization of the words (percent correct: 83.2 [SD=11.5]). Approximately 71% (SD=19.5) of the presented word pairs were recalled correctly after scanning, suggesting that the patients understood the encoding directions and were motivated to try to remember the word pairs.
Correlation Analyses
Regions of Interest
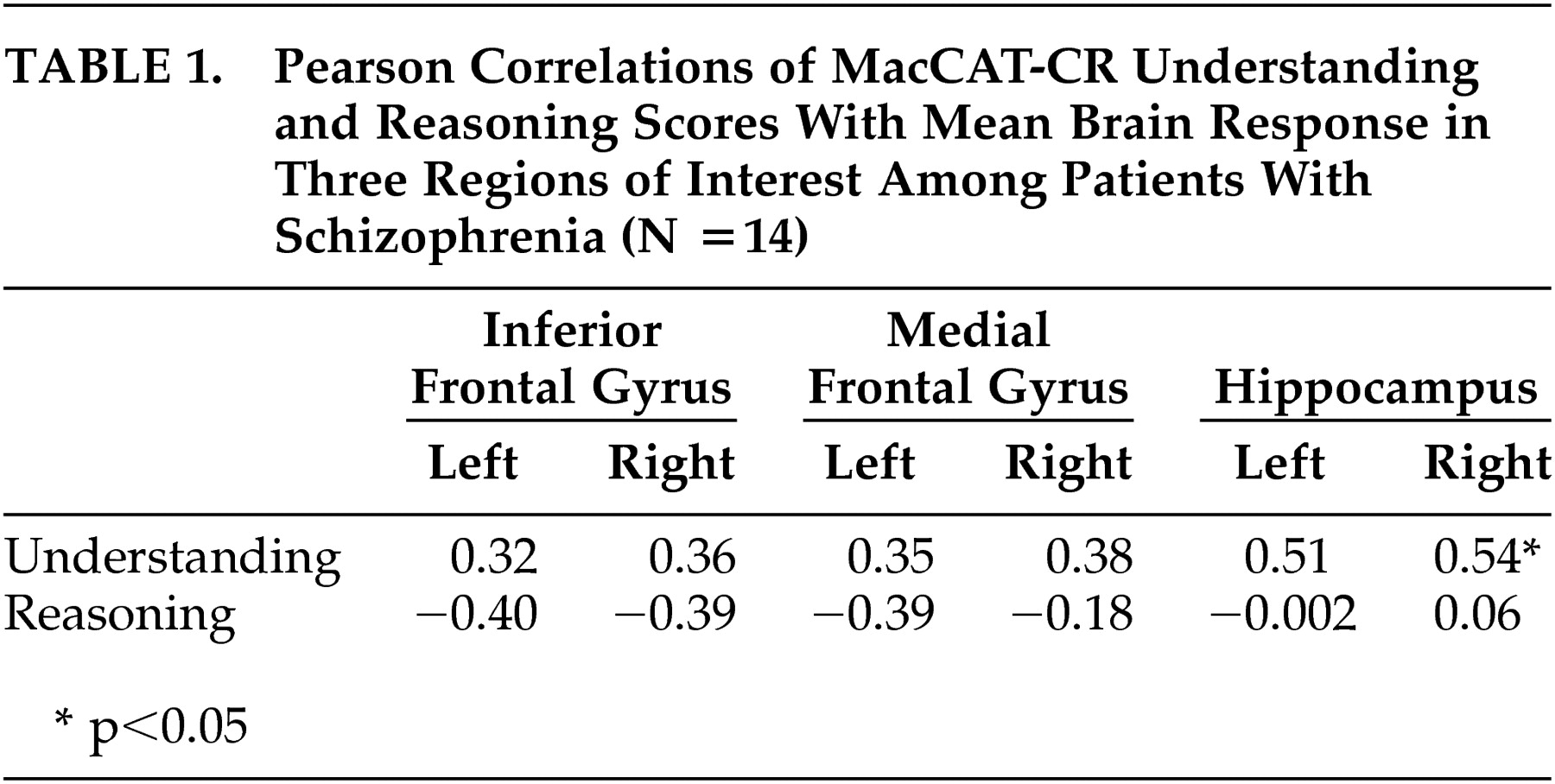
There were no significant correlations between inferior or middle frontal brain response and either Understanding or Reasoning scores (
Table 1 ), but relationships tended to be in the positive direction for Understanding and in the negative direction for Reasoning.
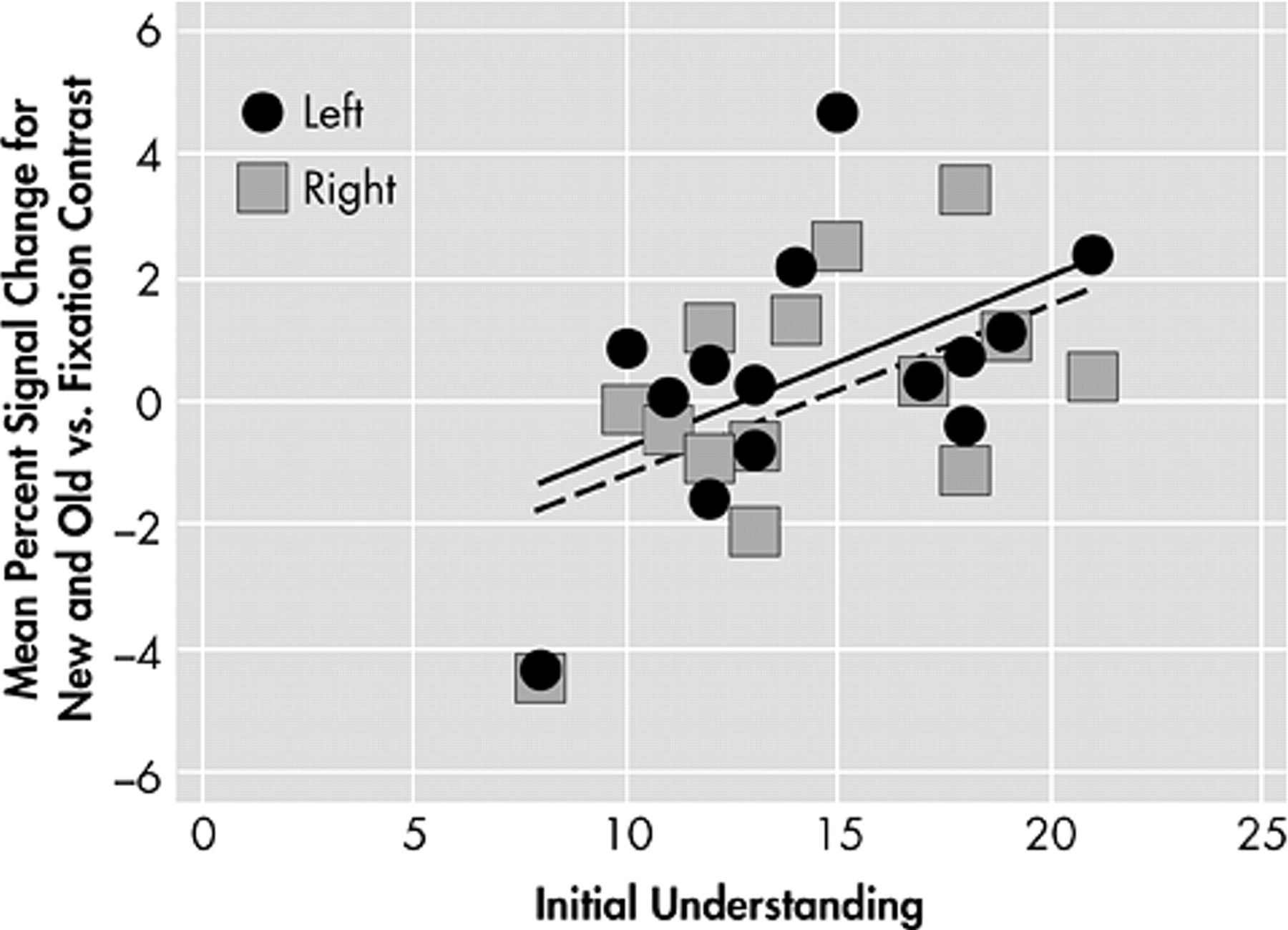
Hippocampal brain response during learning of word pairs was positively correlated to Understanding in the right hemisphere (r=0.54, p=0.04) and there was a trend (r=0.51, p=0.06) toward a relationship in the left hemisphere (
Figure 2 ). No relationship to Reasoning was found in this region.
Whole Brain
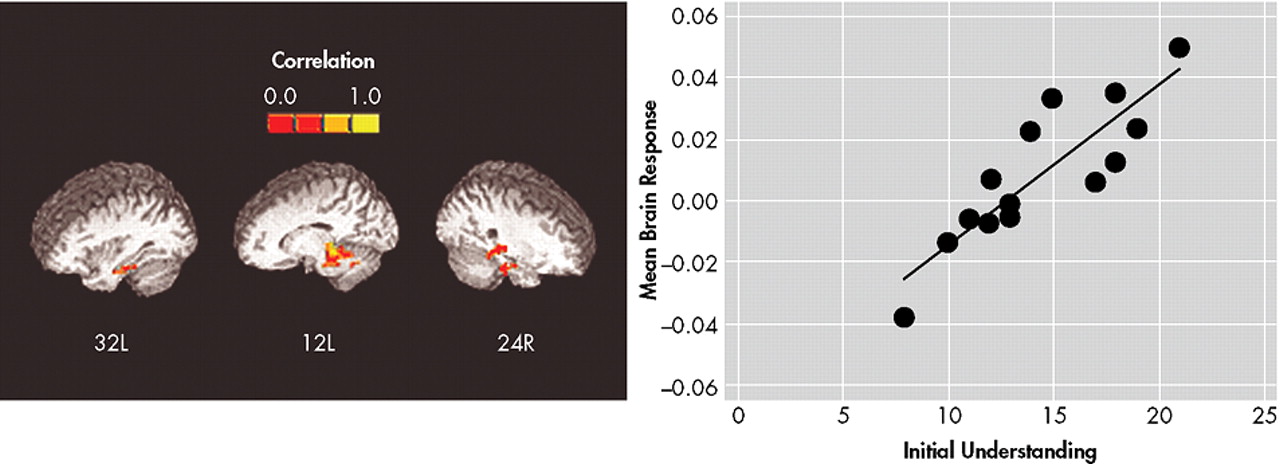
Understanding scores were significantly associated with brain response during learning of Word pairs versus Fixation in a large region (349 voxels, all r≥0.53, p≤0.05; center of mass Talairach coordinates: 0.5 right, 34 posterior, 11 inferior), that included bilateral parahippocampal gyrus and midline culmen of the cerebellum, and extended forward into the bilateral thalamus (
Figure 3 ). No clusters of significant relationship between Reasoning scores on the MacCAT-CR and brain response during learning of word pairs were found.
Potential Moderators
We examined the relationship of MacCAT-CR Understanding scores to demographic, clinical, and task performance data to see if any potential confounding variables might be candidates to moderate either of the significant brain response relationships with Understanding. There were no large or significant correlations between Understanding and age, years of education, duration of illness, PANSS scores, or button-press accuracy during scanning. In addition, we examined the possibility that participant motion may have played a moderating role in the observed relationships. Six summary motion scores (three angles of rotation and three directions of translation) were calculated for each participant to index the degree of within-run movement, and the correlation of each with MacCAT-CR Understanding scores was calculated. All of the correlations were small and nonsignificant (range of r=−0.13 to 0.06, df=12), so there was no evidence that those who had lower Understanding moved more.
Consistent with our assumption that understanding of a consent form is related to an individual’s ability to learn and remember information, there was a significant relationship of MacCAT-CR Understanding with the proportion of Word pairs recalled following scanning, such that participants with better Understanding scores also had better word-pair recall (r=0.62, p=0.02, df=12). As mentioned above, right hippocampal activation during the encoding of Word pairs was significantly related to Understanding scores, as was brain response in a large cluster that included the parahippocampus. Activation of these regions was less predictive of postscan Word pair recall (right hippocampus: r=0.40, p=0.15, df=12; parahippocampal cluster: r=0.49, p=0.08, df=12), although the relationships were similarly positive in direction. Presumably, individual differences in the functioning of the brain in these regions underlie the relationship of Understanding scores with word-pair recall and reflect common information processing demands of the two cognitive activities, although a formal moderation analysis would have been underpowered in this preliminary study. Even if moderation was not supported in a larger sample, however, this would not necessarily imply that the association between Understanding and brain response in these regions was unrelated to verbal encoding processes. Unique features of the paired-associates task (e.g., the high imageability of the words) could have brought other brain systems to bear, slightly weakening the association between individual differences in medial temporal brain response and later recall performance compared to the correlation of Understanding (which involves recall of more abstract and complex material) with brain response in these same areas.
DISCUSSION
As predicted, individuals with the best Initial Understanding scores on the MacCAT-CR had the greatest learning-related activation in the hippocampus, a region thought to be crucial for encoding and recognition.
34 Whole brain analyses also revealed that individuals with good initial Understanding scores showed greater learning-related brain response in a region that included bilateral parahippocampal cortex, cerebellum, and thalamus. Activation of these areas has also been observed during verbal learning tasks.
34 These results suggest that good understanding of a consent form relies, at least in part, on adequate engagement of brain systems known to be involved in encoding verbal information.
Contrary to our hypothesis, however, we did not observe a significant relationship of Understanding to inferior prefrontal function. Prefrontal activation during encoding may reflect use of strategies for rehearsal and semantic elaboration of items.
34 Because the consent-related information was presented in a structured way (as part of a narrative), individual differences in Understanding scores might have been less related to strategic encoding processes (as reflected in frontal activation levels) than to more basic consolidation of information into long-term storage (reflected in hippocampal activation levels).
As expected, middle frontal gyrus activation was not related to Understanding, presumably because heterogeneity in Understanding ability is not driven primarily by individual differences in the functioning of areas involved in working memory. However, we also did not find a correlation between Reasoning scores, which we did hypothesize to be related to dorsolateral working memory systems, and brain response of the middle frontal gyrus. It is possible that the lack of association was due to a restriction of range in Reasoning scores. The verbal learning task also may not have been ideally suited to examine the hypothesized relationship with Reasoning, because it involved fewer demands on working memory.
There are several limitations to the present study. First, the sample size of 14 schizophrenia patients was small and restricted to patients who were mostly male and over the age of 40. Thus, we only had power to detect moderate to large associations, and the results may not generalize to younger or female patient groups. In addition, the number of correlations examined raises the risk of type I error. Second, although the MacCAT-CR scores of this sample were similar to other schizophrenia samples, for ethical reasons we were unable to image those patients (N=5) who did not meet criteria for adequate decisional capacity. These individuals might have shown a qualitatively (rather than simply quantitatively) different relationship, which therefore went unobserved. Future studies using a process of surrogate consent could be helpful in this regard. Third, we chose not to examine brain response correlates of appreciation and expression of choice due to the poor psychometric properties of these subscales. Additional studies using scales specifically designed to assess appreciation, such as the California Scale of Appreciation,
8 would allow us to examine hypotheses about neurocognitive systems related to this component. Fourth, our paired-associate learning challenge task, although designed to involve similar cognitive processes and to evoke brain response of hypothetically important regions, was not a close analogue of the informed consent process. A more realistic informed consent task, although challenging to operationalize in the scanner, would likely yield additional information about brain processes related to heterogeneity in decisional capacity. Finally, we did not examine the correlation of brain response and MacCAT-CR scores within a healthy comparison group. Though it would be interesting to investigate whether the observed relationships are also present in healthy individuals, practical limitations in the variability of understanding and reasoning scores would likely make this comparison difficult. Future studies should address the specificity of these findings to schizophrenia relative to other psychiatric disorders that may involve cognitive impairments.
Despite the study limitations, results of the present study suggest that differences in the function of particular brain systems may underlie differences among individuals with schizophrenia in their ability to understand elements of a consent form. What is not known is whether these specific abnormalities can be remediated with focused interventions. For example, pharmacological treatments that target medial temporal brain functioning might be able to improve not only symptoms but also decisional capacity. Furthermore, interventions that aim at improving the informed consent process itself could be developed to focus on strategies to compensate for possible underlying deficits in new learning. Imaging studies using closer analogs of the consent process during scanning could be helpful to specify further the nature of decisional capacity deficits in schizophrenia and suggest possible ways of ameliorating them.
Acknowledgments
This work was supported by the VISN 22 MIRECC, NIMH grants 5 P30 MH49671-09 and 5 T32 MH19934-07 to Dr. Jeste, and West Coast College of Biological Psychiatry Junior Faculty Award and NARSAD Young Investigator Award to Dr. Eyler. The authors would like to acknowledge the considerable contributions of Jeffrey Gold and Sharon DeCruz in performing the hippocampal tracings. Early results of this study were presented at the West Coast College of Biological Psychiatry Annual Meeting, Seattle, Wash., April 4–5, 2003, and the American College of Neuropsychopharmacology Annual Meeting, San Juan, Puerto Rico, December 7–11, 2003.