Differential Diagnosis
The differential diagnosis of mood disorders and dementia, especially in the early stages of disease, requires expertise on the part of the caring specialist. It remains difficult despite numerous efforts to delineate the two disorders.
50 Depression is frequently misdiagnosed as dementia and up to 32% of patients referred to special departments for dementia evaluation actually suffer from depression.
51 On the other hand, depression often occurs in the early stages of dementing diseases. Early detection of dementia prepares the ground for delaying cognitive decline and gives the caregivers time to adjust to the new circumstances.
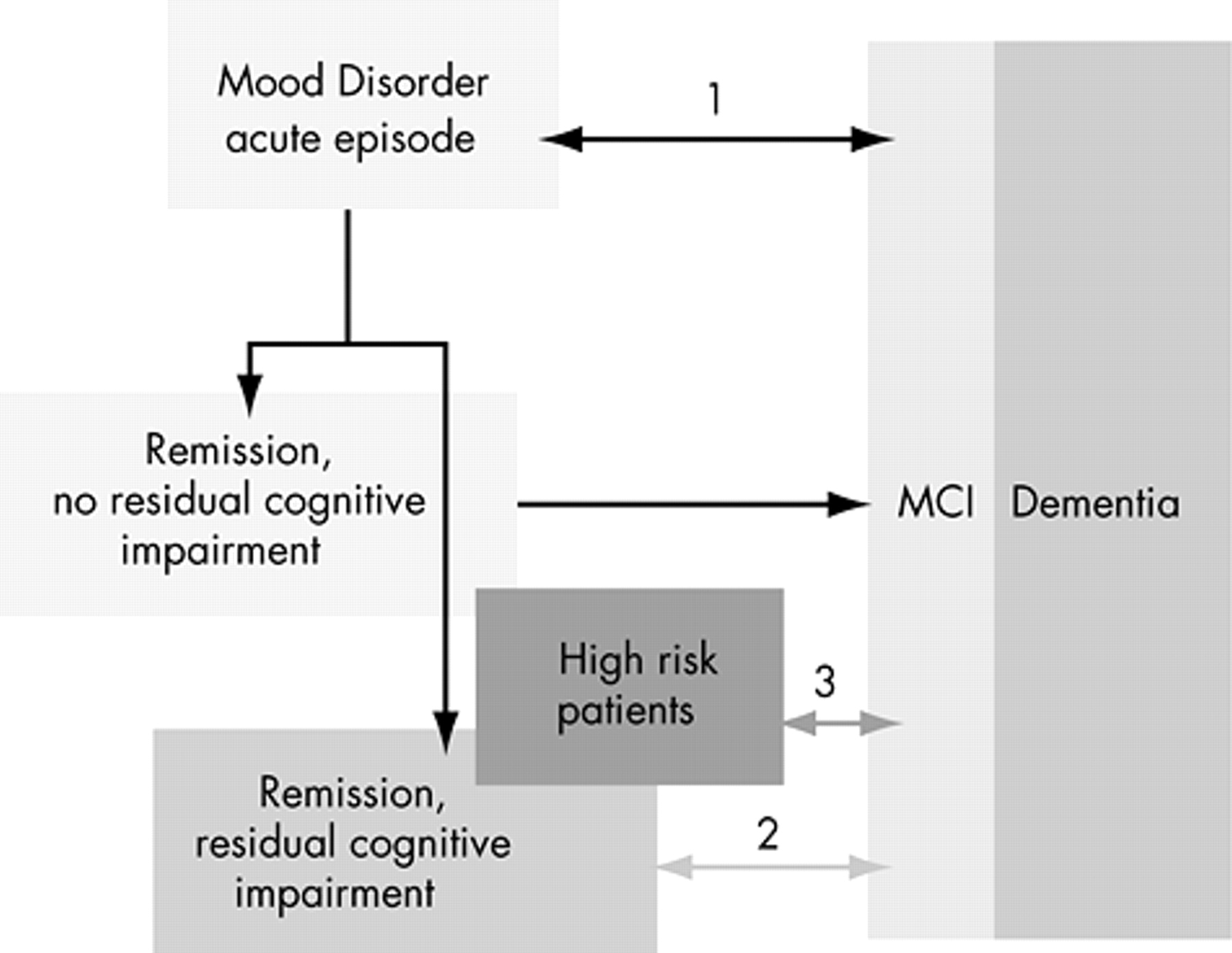
The three major conditions requiring differentiation are depicted in
Figure 1 . The conditions to be differentiated from (early) dementia are mood-associated cognitive impairment in acute episodes,(1) residual cognitive impairment in remitted patients with mood disorders (2) and, if possible, high risk patients with mood disorders who are expected to develop dementia in the future.(3)
In 1979, Wells proposed a widely quoted list of features suggested to differentiate depression with cognitive impairment (formerly termed depressive pseudodementia) from progressive dementia.
52 Some features gained empirical support
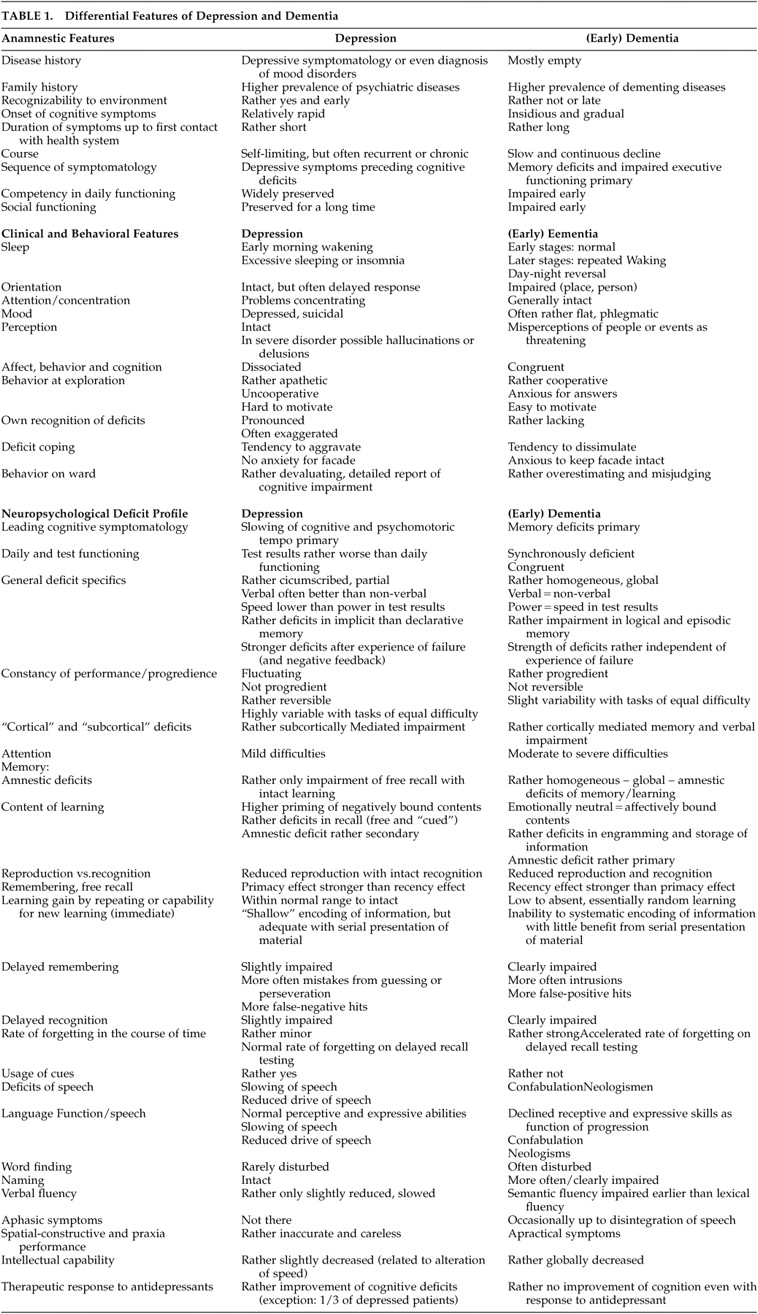
50 and others lack predictive power (e.g., speed of progression). An update of the differential anamnestic, clinical, behavioral, and neuropsychological profiles of patients with present depression and (early) dementia is given in
Table 1 . Behavior at examination, deficit profile, and severity of the deficit add important information for the neuropsychological diagnosis.
The caring specialist’s first diagnostic step for patients presenting with cognitive impairment is to rule out neurocognitive decline due to normal aging. Functions affected by normal aging are mainly slowed recall of new information and problems with nonverbal memory (e.g., misplacing things). Usually, daily functioning is not grossly impaired.
It is essential to exclude the presence of comorbid conditions with secondary neurocognitive impairment by interviewing and physical examination. Additionally, a variety of medications can cause a nonprogressive cognitive impairment which resolves quickly after discontinuation.
Apart from a thorough anamnestic interview (not only with the affected patient but also with a family member or caregiver) and laboratory analyses, including genotyping, appropriate assessment of neurocognitive functioning is warranted. Although neurocognitive testing in affective patients leads to more valid results in stable euthymic states, screening tests for mild cognitive impairment have been developed that prove stable even with comorbid depression.
53Screening tools for mild cognitive impairment and dementia are the commonly used Mini-Mental Status Test (MMST) and the DemTect,
54 the latter being more sensitive to mild cognitive impairment.
55,
56 Additionally, the Clock Drawing Test has been found effective for the detection of very early stages of cognitive impairment.
57 When early dementia is suspected, a neuropsychological evaluation is needed using well-standardized tests of cognition. Here, the Consortium to Establish a Registry for Alzheimer’s Disease (CERAD)
58 test battery or tests from the Nuremberg Gerontopsychological Inventory (NAI)
59 are suggested. The results can help to validate the diagnosis and plan treatment. Neuropsychological testing is considered the most sensitive way to determine the presence, nature and severity of deficits.
50 Recent studies comparing elderly comparison subjects, elderly depressed patients and patients with progressive dementia suggest that the differentiation between the groups is fairly straightforward and facilitated by neuropsychological evaluation.
60Jean et al.
61 used the data of 44 depressed patients on the MMSE and the Dementia Rating Scale (DRS). At follow-up 7.5 years later, subjects who developed dementia had shown greater impairment on tasks measuring attention and memory at baseline than those who did not develop dementia. Future Alzheimer’s disease patients were differentiated on the basis of their difficulties on the MMSE-orientation subtest, whereas the patients with future non-Alzheimer’s dementia initially had more problems with executive functions and visuospatial abilities.
61Of patients with mild cognitive impairment, those that progressed to dementia during prospective follow-up were characterized by a higher severity of impairment on tests of episodic memory at baseline. Additionally, severity of impairment of semantic memory, attentional processing, and speed were predictive markers for progression.
62,
63 Swainson et al.
64 presented data showing that a visuospatial associative learning test (paired-associates learning [PAL] test, part of the Cambridge Neuropsychological Test Automated Battery) accurately distinguished patients with Alzheimer’s disease from depressed and comparison subjects.
Neuroimaging procedures are also being used increasingly for the differential diagnosis of dementing disorders. Techniques, such as magnetic resonance spectroscopy (MRS) and diffusion tensor imaging (DTI), advance the prospects of magnetic resonance imaging (MRI), single photon emission computed tomography (SPECT), and positron emission tomography (PET). CSF analysis assessing the concentration of tau protein (p-Tau
231 ) can be used to differentiate geriatric patients with Alzheimer’s dementia from those with depression.
65