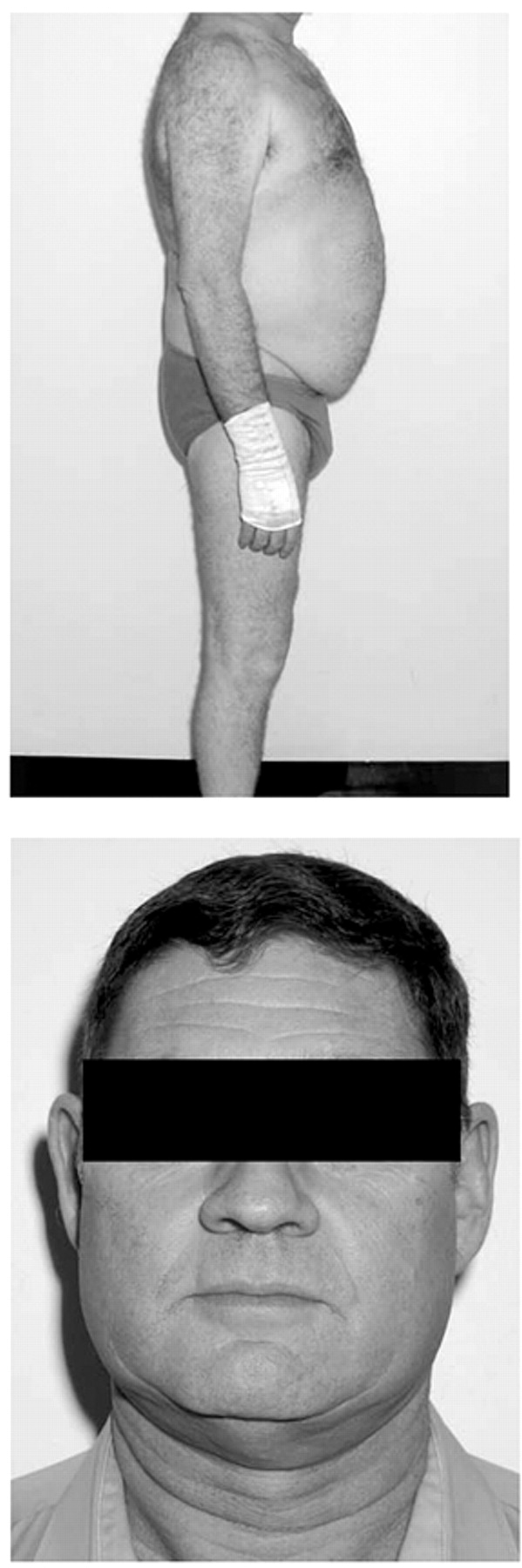
To the Editor: An anxious 53-year-old male presented with hypertension (220/110 mmHg) and hypokalemia (2.6 mmol/liter). Central adiposity and facial plethora were noted (
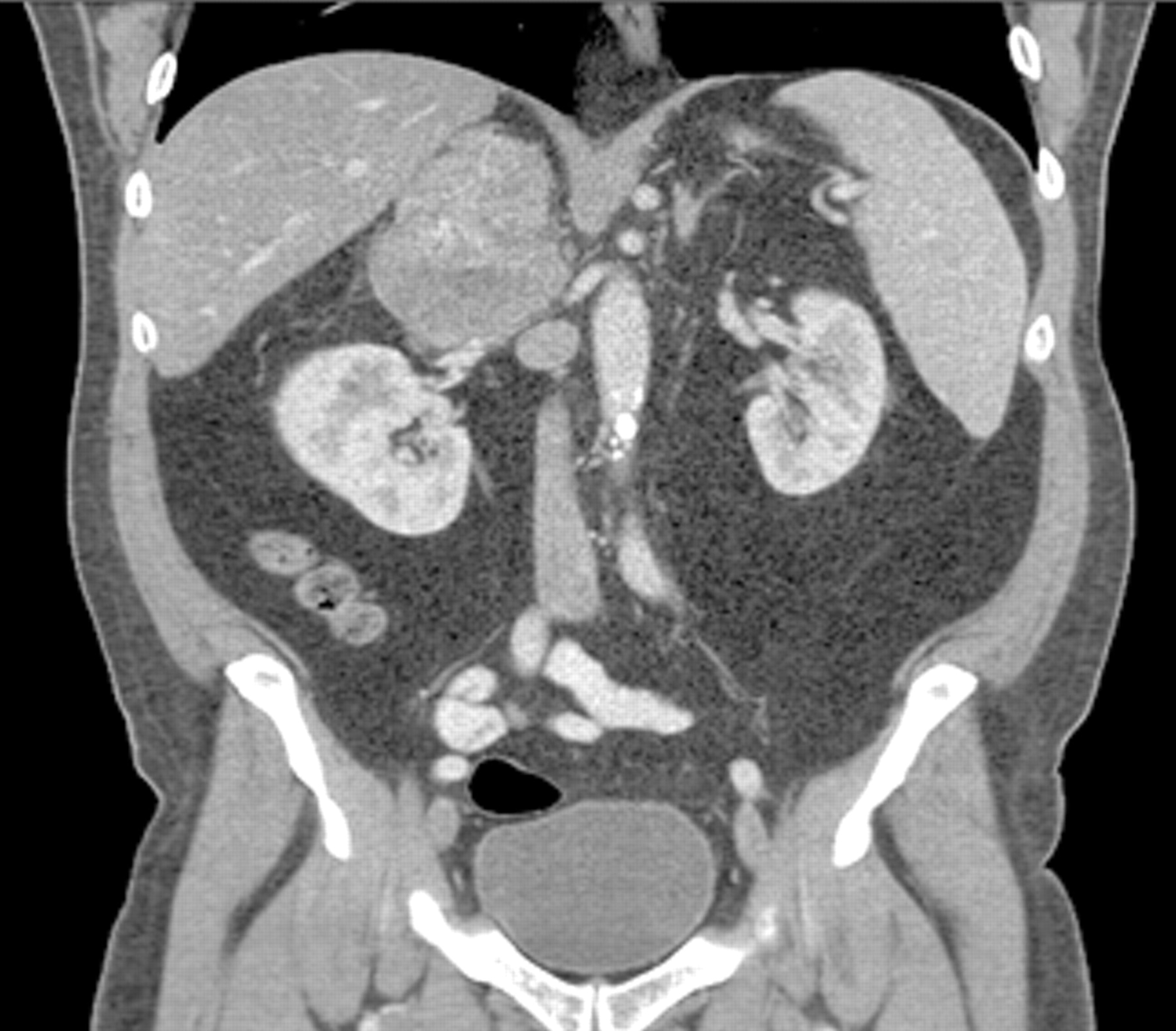
Figure 1 ). Twenty-four hour urinary-free cortisol was >11000 nmol/day (reference range<330) and plasma ACTH 1.6 pmol/liter (2.0–10). Catecholamine, rennin, and aldosterone studies were normal. Abdominal CT scan revealed a 10.7 cm right adrenal mass (
Figure 2 ). Further imaging revealed metastatic lesions in the liver, lungs, left fourth rib and L2 vertebrae, but no intracranial metastases. A diagnosis of cortisol secreting metastatic adrenal carcinoma was made.
Antihypertensive therapy, together with amiloride and potassium supplements, was commenced. Following admission, increasing anxiety became apparent. On mental state examination he was orientated to time, place, and person but complained of difficulties thinking clearly and was easily distracted. He had indifferent affect, tangential thinking, and was easily irritated, being unable to maintain a logical flow of conversation. The following day he became increasingly agitated and irritable and reported racing thoughts. Initial treatment was with lorazepam (1 mg/bd), but olanzapine (5 mg/day) had to be added after the onset of grandiose delusions (e.g., that his mind had the ability to control his heart rate and respiratory functions). The following day he became fully hypomanic with irritability, hyperactivity, distractibility, decreased need of sleep, flight of ideas, and grandiose and paranoid delusions. Insight and judgment deteriorated, agitation increased, he threatened to stop all treatment, and he also threatened medical personnel. Olanzapine was increased to 20 mg/day, and risperidone (2 mg/day) added. Nevertheless, agitation increased, and he was transferred to a psychiatric unit on day 10 of admission exhibiting disinhibition, overfamiliarity, easy agitation, restlessness, euphoria, and grandiose delusions.
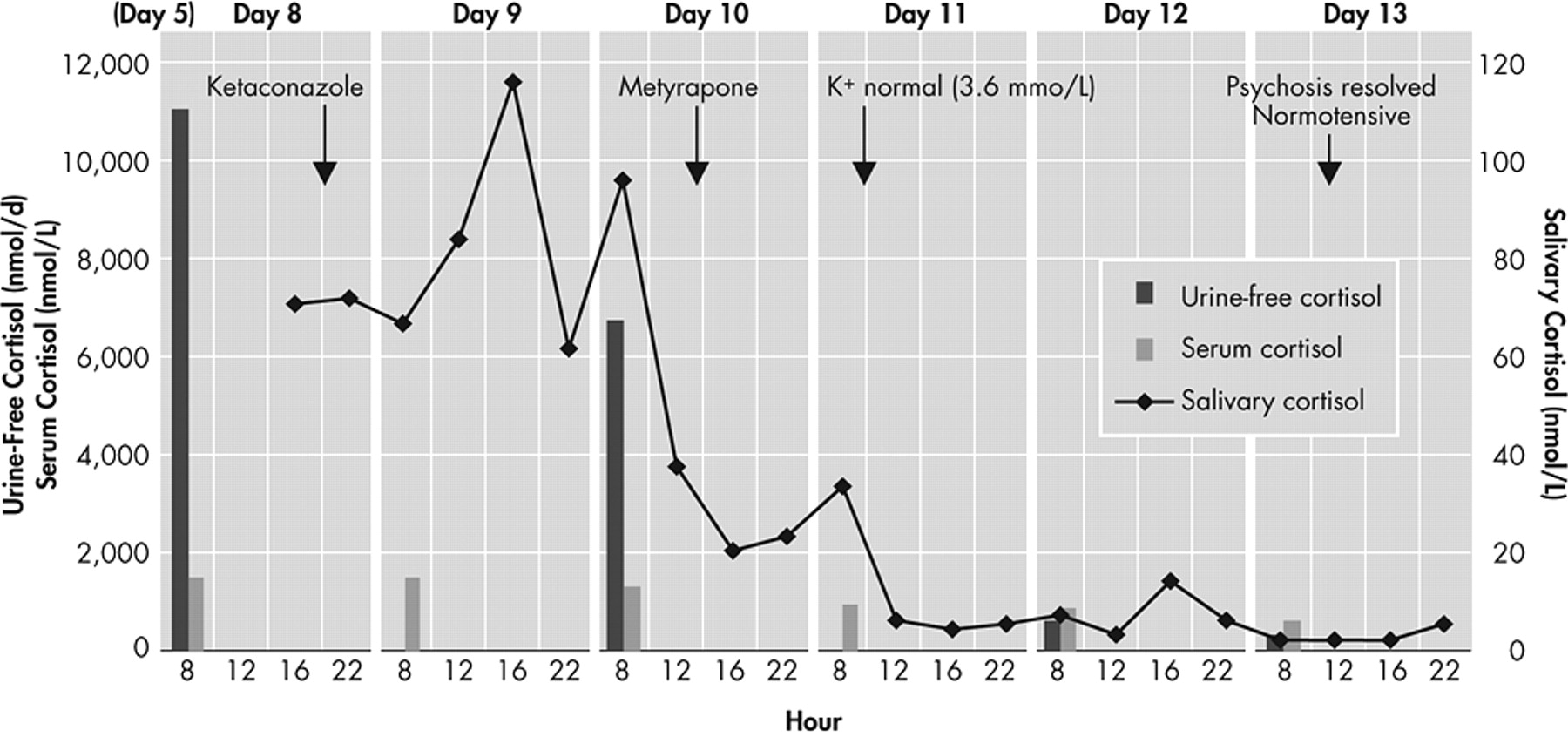
Therapy to inhibit cortisol biosynthesis was initiated with ketaconazole titrated to 1.2g/d. Metyrapone was added the day prior to transfer to the psychiatric unit and rapidly titrated to 1.5g/d. There was substantial reduction in salivary and urinary free cortisol in response to ketoconazole, with additional reduction on introduction of metyrapone (
Figure 3 ). Following normalization of salivary cortisol, his behavior started to improve and blood pressure and serum potassium concentration normalized, allowing cessation of potassium supplements and amiloride. Five days after starting hormonal treatment, his mood, affect, and behavior were normal and he was discharged to the medical ward on olanzapine 10 mg/day.
This report demonstrates that salivary cortisol assays are a convenient means not only of diagnosing but also of monitoring treatment response to medical therapy for Cushing’s syndrome.
1 Prompt resolution of hypertension, hypokalemia and also psychosis occurred with normalization of salivary cortisol levels. While hypertension and hypokalemia are recognized features of severe cortisol excess, Cushing’s syndrome is more commonly associated with anxiety and depression rather than overt mania.
2,
3 Although olanzapine can exert antipsychotic effects within a week of commencing therapy, full resolution of mania would be unusual.
4,
5 Thus the improvement in mental state likely reflected amelioration of cortisol excess. Further investigation of salivary cortisol measurements to monitor response to therapy in Cushing’s syndrome are needed to determine whether resolution of psychosis can be consistently predicted, to allow timely planning and provision of informed consent for definitive therapy.