A ssociation Football (soccer) is a massive participatory sport with 265 million players
1 worldwide. An emerging view in the early 2000s was that head trauma sustained playing soccer could cumulate to cause neuropsychological impairment. A distinction was drawn between concussion, usually due to unintentional impacts with other players,
2 and subconcussive head trauma,
3,
4 usually due to “heading”—intentionally playing the ball using the head. However, this view was recently discounted due to methodological problems including inappropriate control groups, questionable representativeness of study samples, overreliance on self-report to quantify soccer heading, failure to separate head injury from heading effects, and multiple statistical testing with inadequate control of type I error inflation.
5 Several recent adult neuropsychological studies
6 –
12 found no decrements related to soccer heading.
Forty-five percent of U.K. males ages 16–19 years old playing soccer monthly
13 shows soccer’s popularity among young people. However, besides our preliminary report,
11 no neuropsychological investigations of head trauma sustained by adolescent soccer players appear to exist. In the present study we compare neuropsychological test scores of school team soccer players, rugby players and noncontact sport players. Concussive head injury data were collected by self-report. Our definition of concussion included head injuries without loss of consciousness.
14 Headers were assumed to be subconcussive head injuries, defined as any blow to the head without overt concussive symptoms. Focusing on cumulative heading effects necessitated controlling for acute and chronic concussive head injury effects. The former was achieved by excluding participants reporting concussion within 3 months of testing.
3,
15 –
17 The latter was achieved through statistical control of concussions sustained.
Three hypotheses were tested: (a) that the number of head injuries would predict poorer neuropsychological performance in all participants; (b) due to the cumulative subconcussive forces arising from regular soccer heading, that soccer players’ neuropsychological performance would be poorer than rugby and noncontact sport players after controlling for head injuries; and (c) that the total amount of soccer heading would predict soccer players’ neuropsychological performance.
METHODS
Participants
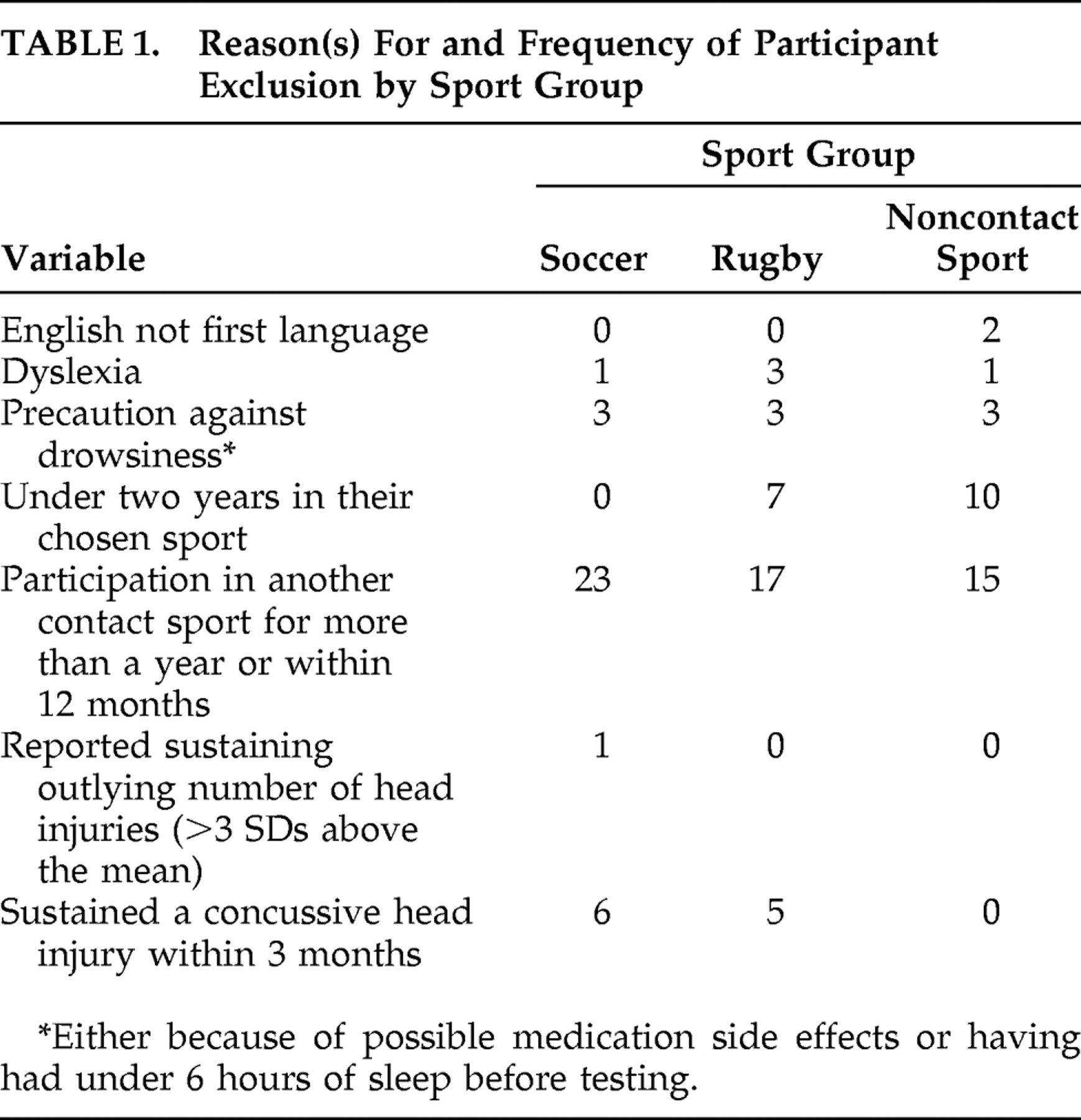
Male state-school pupils ages 13–16 years old participated. Parental consent was obtained for 89 of 142 school team soccer players identified, and 82 attended testing (response rate 63%). After exclusions, 48 soccer players contributed data to the analyses (
Table 1 ). They had played a mean of 3.4 years’ (SD=1.0) competitive soccer since age 11, playing one to two matches and training once per week from September to April. Parental consent was obtained for 58 of 89 school team rugby union players identified, and 56 players attended testing (response rate=65%). Twenty-two rugby players contributed data to the analyses (
Table 1 ). They had played a mean of 3.5 years’ (SD=0.8) competitive rugby since age 11, playing approximately eight matches per season. Parental consent was obtained for 55 of 106 members of school athletics, badminton, basketball, climbing, cricket, squash, swimming, and tennis teams or clubs identified, and 47 members attended testing (response rate 52%). Sixteen noncontact sport players contributed data to the analyses (
Table 1 ). They had played their sport for a mean of 3.4 years (SD=1.0) since age 11. Although not school team or club players, 12 rugby and 11 noncontact sport players occasionally played recreational (“pick-up”) soccer.
Materials
Participants underwent a structured interview assessing demographic, lifestyle and medical factors, head injury history and sports participation history. Also administered were the WISC-R vocabulary subtest,
18 the Childhood Depression Inventory Short Form (CDI-S)
19 and 13 neuropsychological tests: Rey Complex Figure
20 ; WAIS-R Digit Symbol
21 ; WAIS-R Digit Span
21 ; Trail Making test
20 ; Stroop
22 ; WMS-R Logical Memory
23 ; the Alertness, Divided Attention, Covert Attention Shift, Flexibility, and Working Memory subtests from the computerized Test of Attention Performance
24 ; Wisconsin Card Sorting 64-item version
25 ; and Alternate Uses.
26Design
In a quasi-experimental cross-sectional design, three independent groups were compared: school team soccer players, school team rugby players, and school teamor club noncontact sport players. Twenty-five dependent variables were provided by the 13 neuropsychological tests. The WISC-R vocabulary and CDI-S scores, and the responses provided in the structured interview, were employed to check sport group equivalence for depression, premorbid functioning, concussion rates and demographic factors.
Procedure
Teachers at nine local schools identified suitable students. Signed parental consent was a prerequisite for participation. Unreturned consent letters were used to monitor nonresponse. Participants individually attended a free classroom or office for approximately 2 hours to complete the structured interview, questionnaires, and neuropsychological tests. To minimize order effects, the administration order for the questionnaires and neuropsychological tests was varied. Soccer players completed an additional section concerned with heading and soccer participation. A touchline observer recorded heading frequency over one to three matches.
Data Analysis Paradigm
A data analysis paradigm was formulated for the study
27,
28 as part of a strategy to implement control of type I error inflation due to multiple hypothesis testing. This is described in greater detail elsewhere.
10 Briefly, two levels of hypothesis test families were defined. The first level (level A) families were defined by analysis aim: (A1) to determine if the sport groups differ in terms of their biographic characteristics, (A2) to determine whether head injuries predict neuropsychological performance and whether the sport groups differ in terms of their neuropsychological functions, and (A3) to determine if soccer players’ heading frequency is related to their neuropsychological function. A second level (B) of hypotheses test families, described in detail below, were defined within each of the level A analysis aim families as appropriate for the issues addressed. In all analyses a 0.05 significance level was employed and the analysis of variance (ANOVA) convention of treating all tests of hypotheses pertaining to each predictor and each interaction as separate families was retained. Rom’s
29 modification to Hochberg’s
30 multiple tests procedure and, where appropriate, Hochberg and Rom’s
31 extension of Rom’s procedure to situations with logically interrelated hypotheses
32 was applied to the level B families of hypotheses tests in the A1, A2, and A3 families.
For all variables except Test of Attention Performance Alertness, latency, homoscedasticity and normality violations were rectified by data transformation. However, no substantive effects on the general linear model results were observed for those variables for which a rectifying transformation was identified and applied. Therefore, all of the results reported were obtained from analyses carried out on nontransformed data.
RESULTS
A1: Do Sport Groups Differ on Biographic Variables?
B1: Sport Groups That Sustain the Most Head Injuries
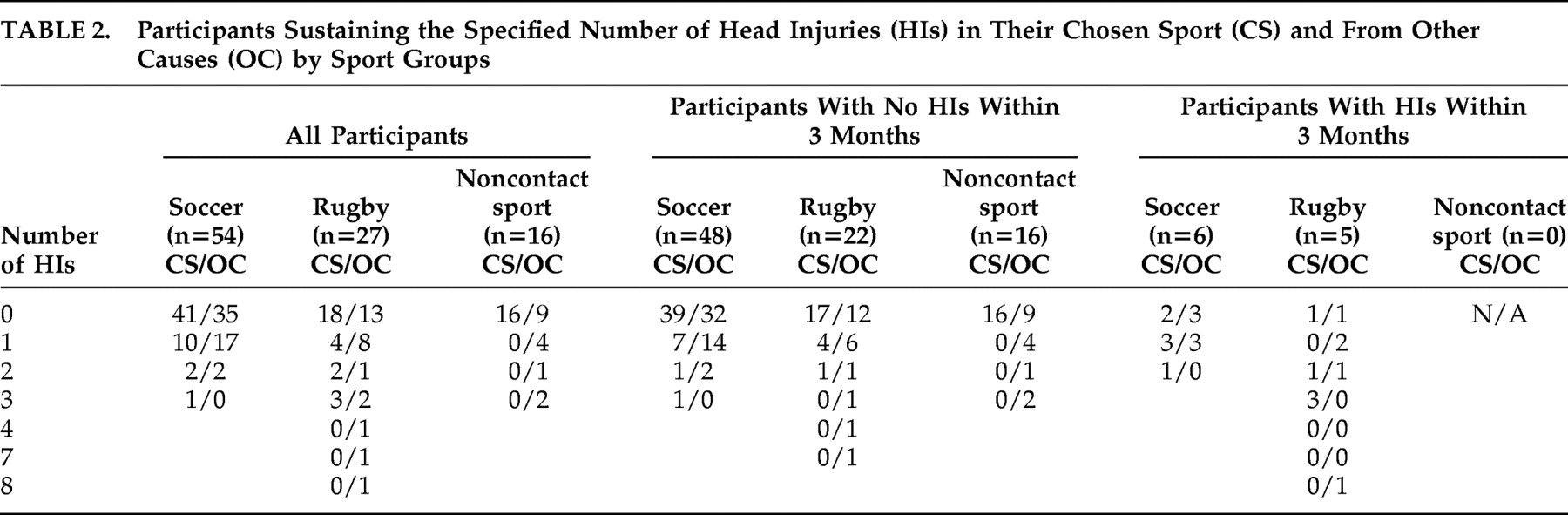
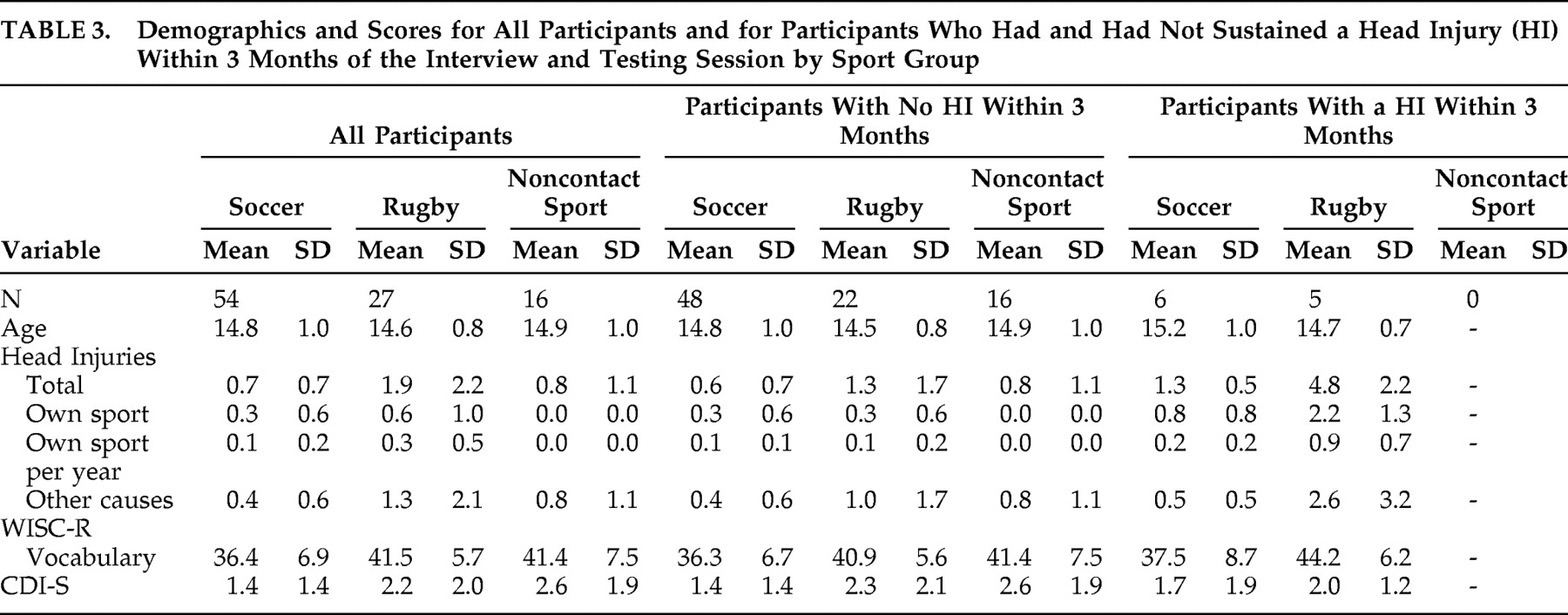
As these analyses do not address neuropsychological function, participants reporting head injury within 3 months of testing were included. Thirty soccer players, 19 rugby players, and seven noncontact sport players reported having sustained one or more head injuries (see
Table 2 and
Table 3 ). The median interval between sustaining a head injury and appearing for testing was 25.0 months (mean=38.0, SD=35.7, range 0–120 months). A Kruskal-Wallis ANOVA was applied to examine the differences between sport groups in terms of the number of head injuries sustained with their own sport (Kruskal-Wallis test statistic =3.983, df=2, nominal p=0.136). As ages are fairly similar across all participants but the number of years playing their chosen sport varies, another Kruskal-Wallis ANOVA was applied to examine the differences between sport groups in terms of the average head injury rate per year sustained within their chosen sport (Kruskal-Wallis test statistic =7.003, df=2, nominal p=0.030). Applying Rom’s procedure, given two Kruskal-Wallis ANOVAs, neither of these differences were genuinely significant.
B2: Age, Vocabulary, and Depression as a Function of Head Injuries and Sport Group
Separate and simultaneous general linear model (GLM) analyses were applied to each of the following dependent variables: age, WISC-R vocabulary score, and CDI-S score in order to understand the relationships between these potentially confounding variables and the main predictor variables used later: head injuries and sport group. The GLMs employed the centered
33 quantitative predictor total number of head injuries; the qualitative predictor sport group; and a predictor representing their interaction. This GLM checked regression homogeneity across sport groups. If the interaction was not significant, a GLM including only head injuries and sport group was applied. GLM analyses employing centered quantitative predictors and categorical predictor(s) are equivalent to traditional analysis of covariance (ANCOVA).
34,
35Neither sport group nor head injuries predicted age. However, sport group was identified as nominally a significant predictor of CDI-S score (F=3.322, df=2, 82, mean squared error [MSe]=2.832, nominal p=0.041) and of WISC-R vocabulary (F=5.863, df=2, 82, MSe=43.838, nominal p=0.004). Rom’s procedure, given three hypothesis tests, identified only the prediction of WISC-R vocabulary score by sport group as genuinely significant. Pairwise comparisons showed that soccer players’ vocabulary scores were lower than those of both rugby players (F=9.632, df=1, 82, p=0.0026, d=0.748) and those of noncontact sport players (F=9.643, df=1, 82, p=0.0026, d=0.718). Rugby and noncontact sport players’ scores did not differ (F=0.011, df=1, 82, p=0.917, d=0.081).
A2: Do Head Injuries of Sport Group Membership Predict Neuropsychological Performance?
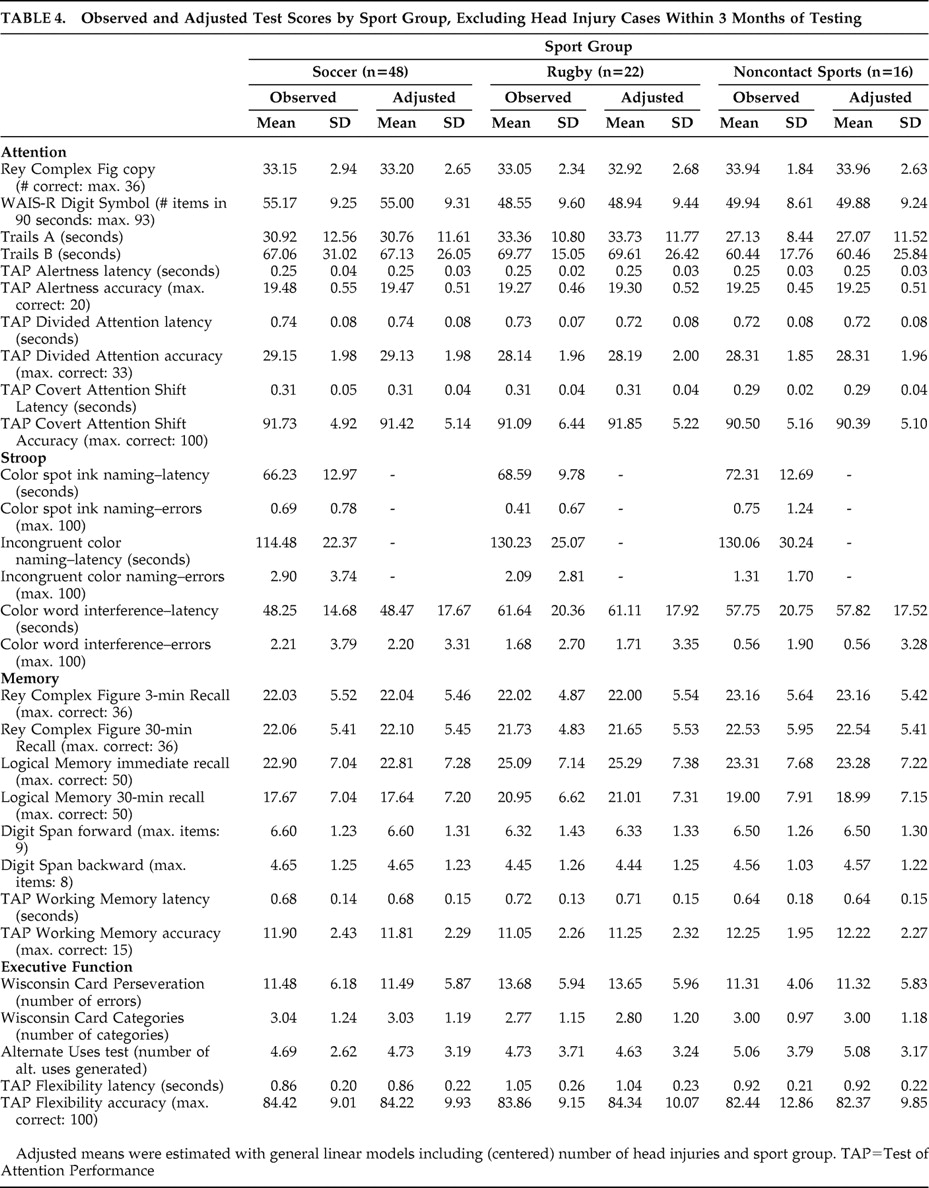
Each of the 25 neuropsychological test scores (12 attention, eight memory and five executive function—see
Table 4 ) was employed as a dependent variable. For each dependent variable, one or two general linear models (GLMs) were applied in a backward stepping approach. The first GLM included the following predictors: centered total number of head injuries, sport group, and the head injuries by sport group interaction. Its purpose was to check regression homogeneity by inspecting the interaction effect. If the interaction was not significant, a second GLM omitting the interaction was employed; where applied, this second GLM is equivalent to a traditional ANCOVA with sport group as the independent variable and total number of head injuries as the covariate.
B1: Attention
Test of Attention Performance Covert Attention Shift Accuracy was nominally predicted by (centered) total number of head injuries (r=−1.644, F=10.454, df=1, 82, MSe=26.016, p=0.002). Sport group nominally predicted Digit Symbol test score (F=3.866, df=2, 82, MSe=85.255, nominal p=0.025) and Stroop interference latency (F=4.335, df=2, 82, MSe=308.852, nominal p=0.016). There were no other nominal effects. Twelve hypotheses were tested with respect to the prediction of attention by head injuries, and by sport group. Upon applying the Rom correction, neither nominal sport group effect was genuinely significant, but the reduction in Test of Attention Performance Covert Attention Shift accuracy with increasing number of head injuries was identified as genuinely significant (effect size omega squared =0.100).
B2: Memory
The only nominally significant effect detected was the prediction of Digit Span backward by the head injuries/sport group interaction (F=3.275, df=2, 80, MSe=1.412, nominal p=0.043). However, applying the Rom correction, based on eight tests of interaction hypotheses with respect to memory, this interaction was not genuinely significant.
B3: Executive Function
The only nominally significant effect detected was the prediction of Test of Attention Performance Flexibility Latency by sport group (F=4.783, df=2, 82, MSe=0.049, p=0.0108). However, applying the Rom correction, based on five sport group hypotheses tests with respect to executive functioning, this effect was not genuinely significant.
A3: Does Heading Frequency Predict Neuropsychological Performance?
Heading observation data were available for 30 soccer players. The median interval between last heading and interview was 3.0 days (range=0–30 days; four soccer players had headed a football on the day of the interview). The mean number of headers observed per match was 4.1 (SD=3.0, range=0–11). The mean estimated number of competitive matches played by the soccer players from the age of 11 was 100.3 (SD=56.5, range=7–194). The product of “observed match headers” and “number of competitive matches played” was used to estimate cumulative heading since age 11 (henceforth just “cumulative heading”). The median of cumulative heading was 247.0 headers (mean=431.9, SD=479.3, range=0–1893). Cumulative heading was significantly correlated with number of head injuries sustained in soccer (r=0.365, p=0.047). As this was the only correlational hypothesis tested, it may be confirmed as being genuinely significant.
A two-step general linear model analysis similar to that described for the A2 family was applied with the following predictors: soccer players’ centered number of concussive head injuries (SHI), soccer players’ centered cumulative headers (SMH), and the SHI × SMH interaction.
B1: Attention
There were no significant effects.
B2: Memory
Only the prediction of Rey Complex Figure 3-minute recall scores by the SHI × SMH interaction was nominally significant (F=10.949, df=1, 26, MSe=27.302, p=0.003). The Rom correction, based on eight interaction hypotheses tests for memory, showed that this effect was genuinely significant (effect size omega squared =0.256). Further analysis of the interaction examined the regression of SMH on Rey Complex Figure 3-minute recall scores at one standard deviation above the mean of SHI, at the mean of SHI and at one standard deviation below the mean of SHI.
33,
36 SMH predicted Rey Complex Figure 3-minute recall at one standard deviation below the mean of SHI (r=0.007, F=4.344, df=1, 26, p=0.047). SMH did not predict Rey Complex Figure 3-minute recall at the mean of SHI (r=0.001, F=0.174, df=1, 26, p=0.680) nor at one standard deviation above the mean of SHI (r=−0.005, F=3.832, df=1, 26, p=0.061).
B3: Executive Function
There were no significant effects.
DISCUSSION
Head Injury
The hypothesis that number of head injuries would predict poorer neuropsychological performance in all participants was supported. After excluding participants reporting recent head injury, Test of Attention Performance Covert Attention Shift accuracy was reduced across all groups by around 1.5% for each head injury incurred. This was a medium to large effect according to Cohen.
37 Nevertheless, sequelae to concussion are not unique to soccer but are present across all activities sharing elevated risk of concussion.
38 The number of head injuries sustained did not differ across the sport groups in the present study.
Sport Group
The hypothesis that soccer players’ neuropsychological performance would be poorer than that of rugby and noncontact sport players, due to the cumulative subconcussive forces arising from regular soccer heading, was not supported. No genuinely significant sport group effects were detected.
Cumulative Heading
The hypothesis that cumulative heading would predict soccer players’ neuropsychological performance was not supported. Underlying the cumulative heading/head injuries interaction observed on the Rey Complex Figure 3-minute recall test was a tendency for better recall, with an increasing number of headers but only in soccer players sustaining fewer head injuries. The interpretation of this finding is unclear; improved performance with increasing head trauma estimates was not predicted. To our knowledge this study records the first estimates of heading frequency in adolescent soccer. The average of 4.1 headers observed per match is considerably lower than the 6–16 headers per match observed in professional male players.
39 –
42Evaluation
This section evaluates how successfully we addressed the common methodological problems described in previous soccer heading studies.
37Control Groups
Employing intact groups raises the problem of how to ensure the groups’ equivalence on background characteristics that are likely to affect neuropsychological test performance. The sport groups were demonstrably homogenous with respect to sex, age, and absence of depression. The soccer players’ poorer premorbid functioning most likely reflects the relative characteristics of people who play soccer seriously rather than reflecting some change brought about by soccer participation. In Britain, most young males play soccer to some degree, and this is illustrated in the several control group members reporting playing low-level recreational soccer. However, since the frequencies of head injury and heading are positively correlated with level of soccer play,
37 including these cases is not likely to have confounded the results significantly.
Representativeness
The high response rates indicate that participants were reasonably typical of their respective populations. However, the considerable overlap in the sports history of members of different study (sport) groups necessitated developing exclusion criteria based on participatory experience. A tension arose between limiting exclusion to maximize statistical power and limiting inclusion to reduce “data noise” from shared sport history. One consequence of the criteria adopted is that despite collecting data from more participants, the rugby and noncontact sport group samples actually diminished between our preliminary paper (discussed later) and this report. Nevertheless, the study was powered sufficiently to detect several nominal sport group effects, although none indicated reduced performance in the soccer players.
Overreliance on Self-Report to Quantify Soccer Heading
Employing observed match heading as one component of our cumulative heading estimate is an improvement on many prior studies.
Separating Concussive and Subconcussive Effects
We avoided confounding acute and chronic head injury effects by excluding participants reporting concussion within 3 months. Furthermore, by statistically controlling concussion, any sport group or cumulative heading effects in our statistical models may be assumed to be attributable to causes other than concussion. However, head injury history was collected by self-report and so, inevitably, will incorporate a degree of error. Recent soccer heading raises the possibility of data contamination by acute heading effects. However, prior research indicates an absence of cognitive
43 or neurochemical
44 effects immediately following heading training sessions.
Type I Error Inflation
The data analysis paradigm employed
10 ensures that the study complies with the requirements for confirmatory rather than exploratory research.
45 It is notable that although confirmatory research sets more stringent statistical criteria, implementing type I error control did not eliminate any nominally significant prohypothesis effects. We believe the criteria set here achieve a reasonable balance between controlling type I error and maintaining analysis power.
Preliminary Data
In a preliminary paper, increased cumulative heading marginally predicted decreased Test of Attention Performance Divided Attention accuracy.
11 However, we specifically noted that this finding was subject to ratification by confirmatory analyses employing appropriate type I error control. The absence of an equivalent effect in these final confirmatory analyses suggests that the preliminary finding was a statistical artifact and affirms our cautious interpretation.
CONCLUSION
There was no evidence of neuropsychological decrement in adolescent soccer players or rugby players compared with noncontact sport players. Neither was there any relationship between cumulative heading and neuropsychological decrement. However, consistent with previous reports, there was evidence of poorer attention performance with increasing concussive head injury across all participants. Therefore, while no specific attribute of soccer was linked with neuropsychological deficit, concussion arising from general sports (including soccer) and other sources may be linked to decrements in attention, although the literature indicates that such effects are likely to be transitory.
38Acknowledgments
Funded by the Wellcome Trust, grant reference 054248. This research was approved by the Keele University Department of Psychology Research Ethics Committee.