Although anxiety symptoms are one of the most common psychological expressions among older adults (
1 ), there have been remarkably few epidemiological studies of anxiety disorders for this age group (
2 ). Moreover,
DSM-IV criteria have made interpretation of the extent of anxiety disorders in later life difficult because anxiety is often accompanied by medical illness, depression, or cognitive difficulties (
3,
4 ). Thus, according to diagnostic algorithms, comorbid conditions may take precedence with respect to diagnosis. This is unfortunate because anxiety symptoms may have independent effects on mortality, adaptive functioning, and life satisfaction. Anxiety symptoms also may affect the course of depressive, cognitive, and medical disorders (
4,
5,
6 ). To rectify this problem, several writers (
4,
7 ) have suggested using a dimensional model in which anxiety could be conceptualized into a separate dimension that might accompany other dimensions, such as depression or cognitive impairment.
Another important limitation of prior studies was the lack of a theoretical model to assess anxiety. Use of a theoretical model would allow for the inclusion of an array of independent variables and provide a basis for generalization across studies. In this study we used an adaptation of George's social antecedent model of psychopathology (
12 ). This model consists of six stages of risk factors—demographic factors, early events and achievements, later events and achievements, social integration, vulnerability factors, and provoking agents—with later stages hypothesized to be increasingly proximate precursors of mental disorders.
Finally, the few extant epidemiological studies of anxiety in later life have not included large numbers of people from minority groups. The Epidemiologic Catchment Area study included older members of minority groups, but the numbers were limited to three sites (
13 ). The recent National Comorbity Survey Replication (
14 ) survey of anxiety disorders in the United States included slightly over 100 non-Hispanic older black respondents. Neither of these studies fully took into account the increased diversity of the black population resulting from the influx of approximately two million African-Caribbean immigrants into the United States (
15 ) and the fact that a proportionately greater number of older black persons are found in Northern metropolitan areas (
16 ).
Using the theoretical model described above with a large multiracial population of persons aged 55 and older who were residing in Brooklyn, New York, we addressed three questions with this study: What are the prevalences of subsyndromal and syndromal anxiety? What are the factors associated with each level of anxiety? Are there clinical and social factors that justify the use of subsyndromal anxiety as a distinct category of anxiety among older adults?
Results
Overall, 15.6 percent of respondents met our criteria for clinical anxiety, with 2.3 percent meeting criteria for syndromal anxiety and 13.3 percent meeting criteria for subsyndromal anxiety. We also examined whether there were intragroup differences in the prevalence of anxiety disorders in the black population. Rates of subsyndromal anxiety were 10 percent for U.S.-born black persons, 10 percent for English Caribbeans, and 8 percent for French Caribbeans. These intragroup differences were not significant. Rates for syndromal anxiety were 2 percent for the U.S.-born black persons, 5 percent for English Caribbeans, and 4 percent for French Caribbeans. These intragroup differences also were not significant.
In bivariate analyses (
Table 1 ), persons in the subsyndromally anxious group differed from those in the nonanxious group on six of 17 variables. Persons in the subsyndromally anxious group were more likely to report greater lifetime trauma, more physical illnesses, greater depressive symptoms, more phobic symptoms, and more acute stressors and to deal with conflicts by keeping things inside. Persons in the syndromally anxious group differed from nonanxious individuals on eight variables. Persons in the syndromally anxious group were more likely to be women, to consider a greater proportion of their network contacts to be intimates, to deal with conflicts by keeping things inside, to have lower income, and to report more physical illness, depressive symptoms, phobic symptoms, and acute stressors. The syndromally anxious group differed from the subsyndromally anxious on five variables. The latter were significantly more likely than the syndromally anxious group to be male and to have fewer physical illnesses, more phobic symptoms, higher income, and a lower proportion of intimate contacts.
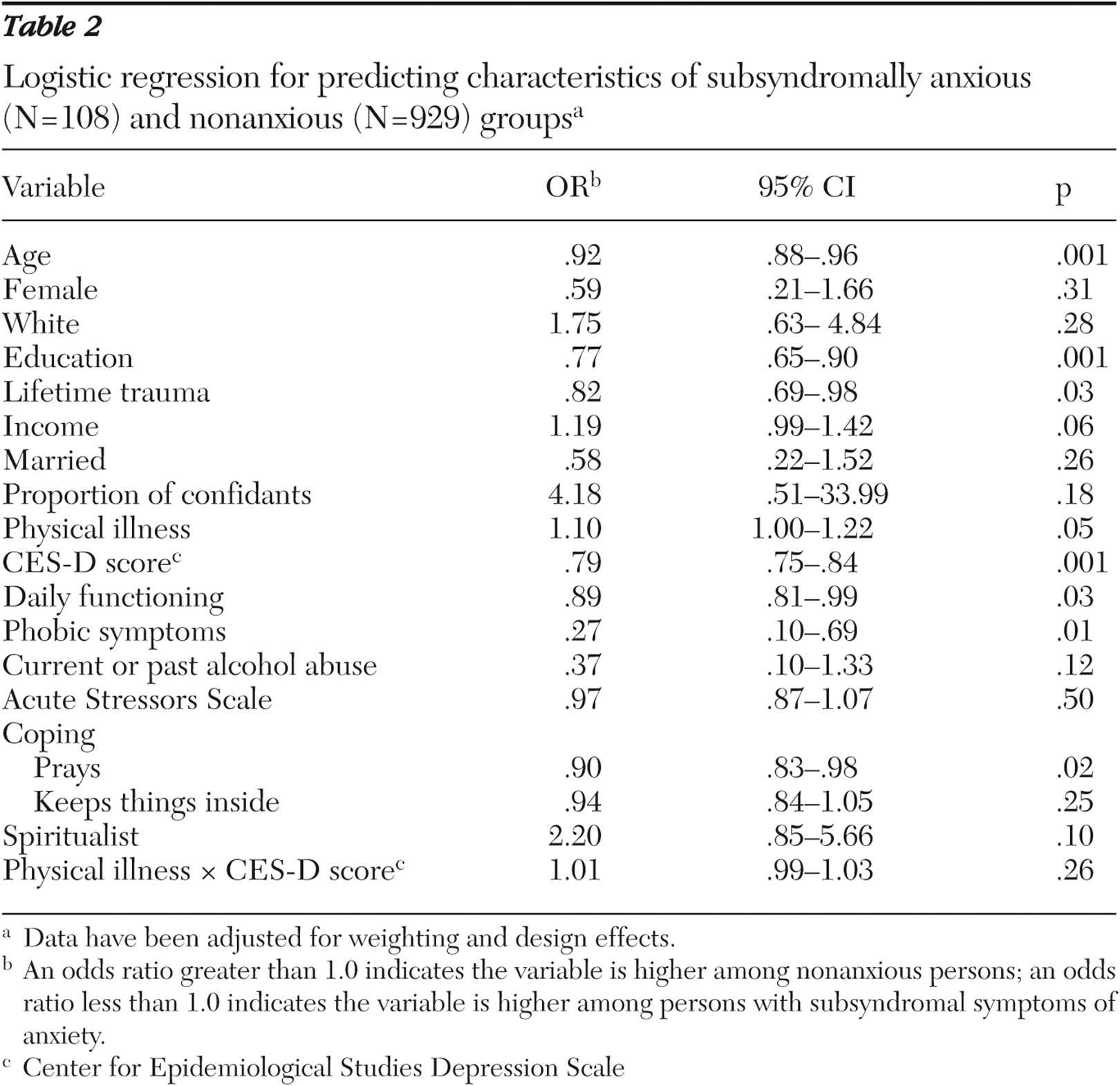
In logistic regression analyses, the subsyndromally anxious group differed significantly from the nonanxious group on seven of 18 variables (
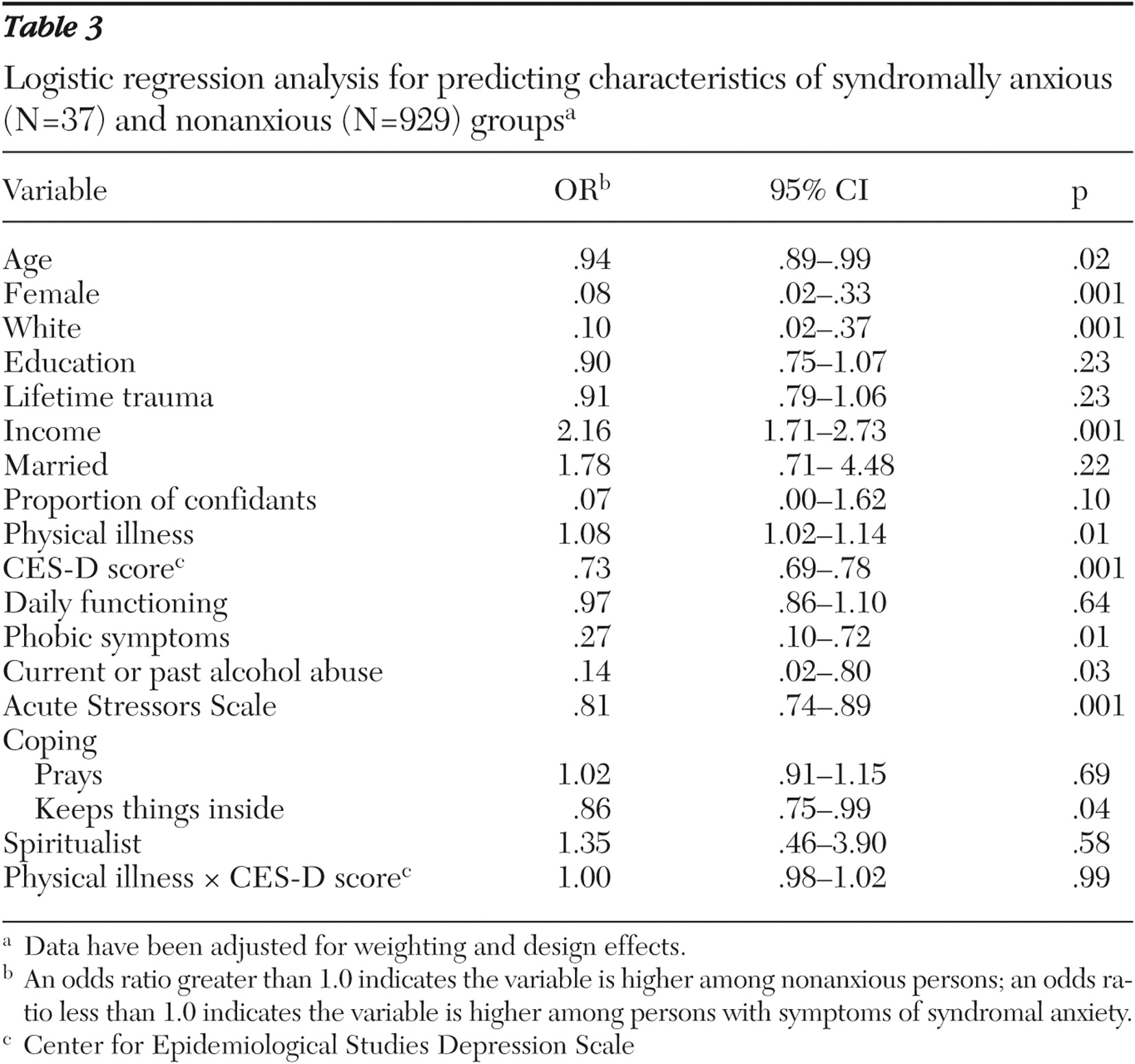
Table 2 ). The former was significantly older, had more education, more lifetime trauma, dealt with conflicts with prayer, had better daily functioning, and reported more physical illnesses and depressive symptoms. Persons in the syndromal anxiety group differed significantly from the nonanxious group on ten variables (
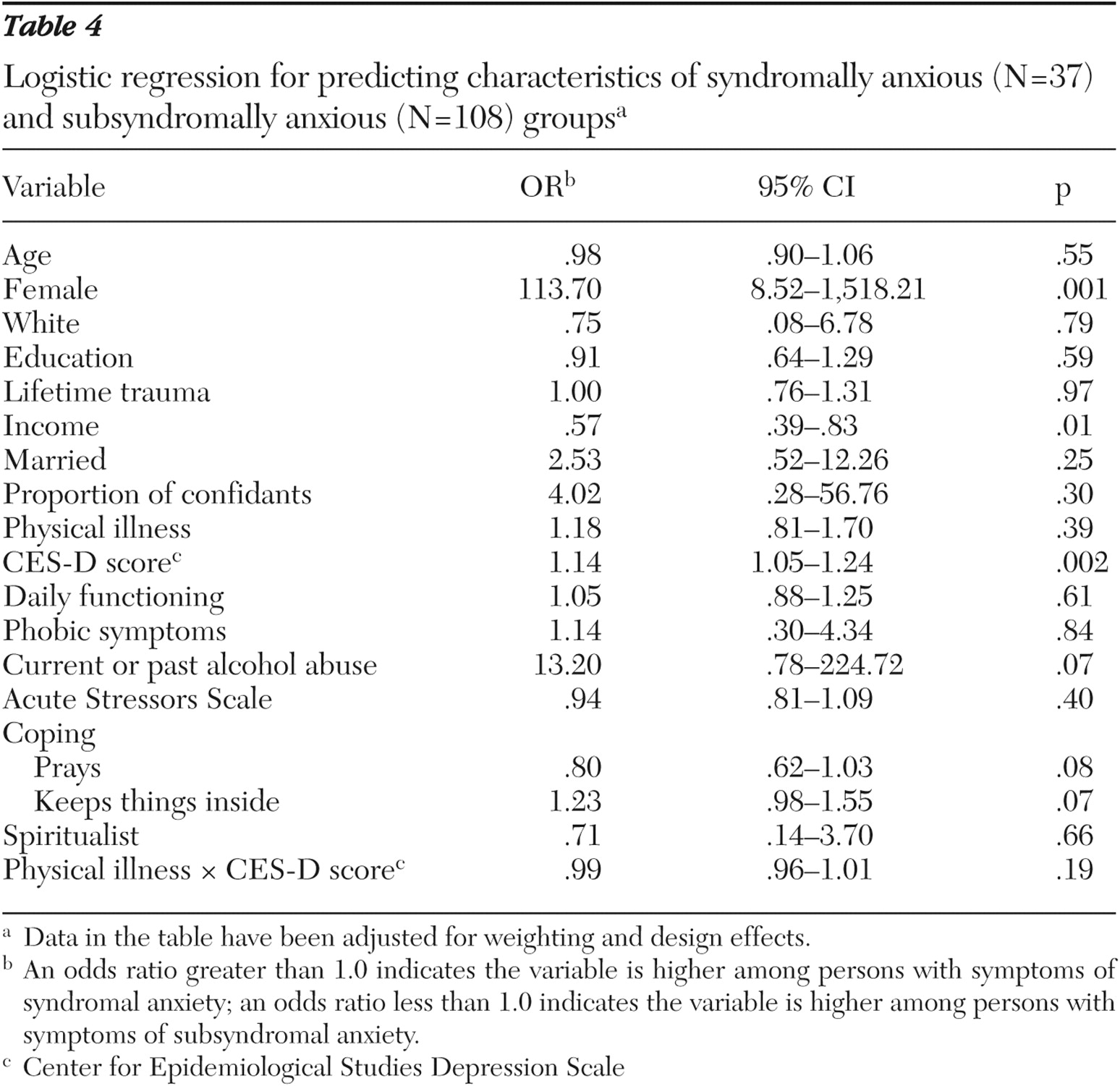
Table 3 ). They were more likely to be female, older, and white; to have current or past alcohol abuse, more acute stressors, and lower income; to deal with conflicts by keeping things inside; and to report more phobic symptoms, more physical illnesses, and more depressive symptoms. Persons in the syndromally anxious group differed significantly from those in the subsyndromal group on three variables (
Table 4 ). Persons in the latter group were more likely to be male, to report fewer depressive symptoms, and to have a higher income.
With respect to mental health treatment, 23 percent in the syndromal anxiety group, 12 percent in the subsyndromal anxiety group, and 3 percent in the nonanxious group reported talking to any type of doctor for mental health reasons in the past year. Although there was a greater likelihood for persons in the anxiety groups to have spoken to a physician, none of these differences attained significance. Finally, anxious individuals were more apt to have seen a physician three or more times in the past year, with 93 percent in the syndromal anxiety group, 76 percent in the subsyndromal anxiety group, and 68 percent in the nonanxious group reporting this frequency level (syndromal anxiety compared with nonanxious, χ 2 =6.49, df=1, p=.01; subsyndromal anxiety compared with nonanxious, not significant; all anxiety disorders compared with nonanxious, χ 2 =3.89, df=1, p=.05).
Discussion
The prevalence rate for syndromal anxiety of 2.3 percent was consistent, albeit on the lower end, with prevalence rates for general anxiety disorder of 1.9 percent to 7.3 percent reported in other older populations (
4,
8,
10,
41 ). Few studies have examined subsyndromal anxiety among older adults. However, our data resembled those in a study of Kentucky elders in which 20 percent had levels of anxiety that warranted clinical interventions (
22 ). Our combined total for syndromal and subsyndromal anxiety was 15.6 percent.
By using a multicategorical model and including a broader representation of individuals with anxiety symptoms in our study, we were able to clarify previously reported differences between anxious and nonanxious older adults in the general community. We found differences at five of the six levels in our model. Specifically, in the logistic regression analyses we found that persons with syndromal anxiety differed significantly from nonanxious individuals on ten of 18 model variables and that persons with subsyndromal anxiety differed significantly from nonanxious persons on seven variables. However, the two anxiety groups differed significantly on only three of the 18 variables. Thus the latter two groups differed on substantially fewer variables than they did with the nonanxious group.
An important issue is whether the differences between the nonanxious and subsyndromal groups were of sufficient merit to warrant a distinction. The fact that the latter exhibited significantly more depression and physical illness than the nonanxious group suggests that there is a conjunction of depression, physical illness, and subsyndromal anxiety that parallels findings with syndromal anxiety, both in our study and in earlier reports (
27 ). Because we used cross-sectional data, causal directions could be determined; however, it is likely that these relationships were mutually reinforcing. As Lindesay (
42 ) observed, "There is a complex interaction between anxiety, depression, and physical ill-health," and he suggested that anxiety disorders may aggravate and complicate more clinically conspicuous physical and psychiatric disorders. However, our regression analyses did not detect any interactive effects of depressive symptoms and physical illness on anxiety, so the relationship among these variables may be additive rather than interactive.
With respect to the other variables, all the demographic variables were significant in one or both anxiety groups. Our finding that older age was associated with both anxiety groups is consistent with some studies that found that anxiety increases with age, especially among subsyndromal cases (
8 ). However, most studies, using more traditional diagnostic categories, have found similar or lower rates among older persons (
3,
13,
14,
26 ). Also, consistent with studies of older populations (
13,
20,
36 ), we found that women were more likely to have syndromal anxiety, although this result was not significant for subsyndromal anxiety. Our results differed from several European studies that found gender differences in subsyndromal cases (
8,
10 ).
Our finding that white persons had higher levels of syndromal anxiety than black persons differed from the Epidemiologic Catchment Area sites that found no racial differences among older adults or that syndromal anxiety had a slightly greater prevalence among older black persons (
13,
43 ). It is not clear whether our findings reflect differences in geography, historical changes in symptom patterns among races, or methodological differences in studies. Our large sample also allowed for within-group comparisons for the black sample, and we found no ethnic differences in rates of syndromal or subsyndromal anxiety.
With respect to the life events and achievement variables, consistent with other reports (
13,
10,
44 ), we found lower income to be associated with anxiety, although this association was more pronounced among the syndromally anxious group. Contrary to most earlier reports (
13,
10 ), we found higher education to be associated with higher anxiety levels, although this association attained significance only among subsyndromally anxious persons. During the last third of the 20th century there was an out-migration of the middle class from many of the census tracts in our study. For persons with more education, remaining in these neighborhoods may reflect personal circumstances that could contribute to anxiety or depression, or conversely, remaining in more troubled neighborhoods may have more profound emotional effects on those with more education (
45 ).
Consistent with our model, more accumulated lifetime traumatic events were associated with subsyndromal anxiety. Marital status, which had been reported as a differentiating variable by other investigators (
13,
44 ), did not attain significance in bivariate or regression analyses. The social network variable (proportion of intimates) likewise failed to attain significance in regression analyses.
In addition to physical illness and depressive symptoms, two other vulnerability variables—past or current alcohol abuse and acute stress—attained significance for the syndromally anxious group. As Liptzin (
46 ) observed, alcohol can cause anxiety for some and relieve anxiety for others. Similarly, although acute stressors were significant for both anxiety groups in bivariate analysis, they retained significance among only the syndromally anxious group. This finding is consistent with other studies that postulate that acute stressors may be precipitants of anxiety (
5,
24 ). Finally, our findings supported our inclusion of coping variables. Coping by prayer was greater among those with subsyndromal anxiety, whereas syndromally anxious persons coped by keeping things inside. Why different coping styles predominated at the two levels of anxiety will need further study.
Although persons in the syndromally anxious group were also more likely than persons in either the subsyndromal or nonanxious groups to consult any type of doctor for mental health reasons, fewer than one-quarter did so. Because 79 percent of persons with any anxiety disorder saw a physician three or more times in the past year, these encounters offer potential opportunities for assistance. As has been done for depression, the feasibility of enlisting primary care physicians to identify and treat anxiety disorders should be explored (
47 ). On the other hand, despite the higher number of depressive symptoms that accompanied the anxiety disorders, both anxiety groups maintained levels of daily functioning and emotional closeness that were comparable with the nonanxious group. Thus, given a reasonable level of instrumental and social functioning, most persons in the anxiety groups apparently felt little need to seek assistance. Indeed, Kessler and associates (
48 ) observed that anxiety disorders per se do not trigger help seeking and that treatment typically occurs when anxiety accompanies other disorders.
Finally, although this study offers new insights about older adults with anxiety in one urban setting in the Northeast, it has several limitations that reflect the exploratory nature of this work. It is cross-sectional so that causal relationships cannot be determined, and the method of determining syndromal and subsyndromal anxiety is not based on formal clinical diagnostic categories.
Conclusions
In addressing the three questions posed in the introduction, we found that about one in seven older adults has appreciable anxiety, there are substantial differences in psychosocial and health-related factors associated with anxiety and nonanxiety, and there is provisional support for viewing older adults with subsyndromal anxiety as distinct from nonanxious older individuals. Future studies will need to identify clinically meaningful points of demarcation between subsyndromal anxiety, syndromal anxiety, and nonanxiety for older individuals.
Community psychiatrists must recognize that there are many untreated older persons with anxiety in the general community. Notably, persons with subsyndromal anxiety, who represent slightly more than one-sixth of older adults, are likely to be overlooked because they do not attain the diagnostic threshold for anxiety disorder. However, the prevalence of subsyndromal anxiety may increase with age, and it is independently associated with more depressive symptoms and more physical disorders. Recognizing and treating anxiety with a combination of medical and psychosocial interventions may have a substantial impact on the well-being of elders in the community.