Surveys after the World Trade Center attacks on September 11, 2001, reported substantial traumatic stress among 61 percent of 560 randomly sampled adults who lived within 100 miles of Ground Zero (
1 ). Additionally, among 3,512 randomly selected respondents within the New York City metropolitan area, 38 percent reported heightened worry, 14 percent reported sleep difficulties, and 8 percent reported hopelessness (
2 ). Furthermore, of 1,008 adults living south of 110th Street in Manhattan, 7.5 percent reported symptoms consistent with probable posttraumatic stress disorder (PTSD) and 9.7 percent reported symptoms consistent with depression (
3 ).
In response to the attacks, the New York State Office of Mental Health used funding from the Federal Emergency and Management Agency (FEMA) to develop a large-scale public health intervention, Project Liberty. Within four to six weeks after the attacks, thousands of mental health professionals and paraprofessionals were trained in the basics of community outreach and disaster counseling (
4 ). Project Liberty offered short-term outreach, crisis counseling, and public education services through community outreach in settings such as homes, schools, community agencies, and businesses. Project Liberty provided services at no cost to recipients.
Analysis of logs of service encounters from the first five months of Project Liberty indicated that 9 percent of 36,672 service recipients who received individual counseling were referred for more intensive mental health services (
4 ). Such referrals were based on counselors' perceptions that clients' clinical needs were beyond the scope of brief treatment. Over the next two years, counselors continued providing such triage referrals for more intensive non-Project Liberty mental health services, including evaluations to determine whether prescription of psychotropic drugs was appropriate (medication evaluations). This report describes demographic characteristics and risk factors that predicted whether recipients of brief counseling received referrals for more intensive and specialized mental health services.
Methods
FEMA funding rules required that all Project Liberty services be anonymous. A total of 177 service providers completed 753,015 service logs indicating date and location of service (for example, school or place of employment), borough or county where service was received, and risk category (for example, family of missing or deceased; injured in the attack; or fire, police, or rescue personnel). For individual counseling sessions, service logs further indicated whether counseling contacts were for a first or follow-up visit and listed demographic information for individuals (for example, gender, preferred language, and race or ethnicity, as observed by service providers). Counselors also noted whether the individual exhibited any of 31 event reactions related to the attacks (coded as present or absent) at the time of the visit. These event reactions, which mapped onto DSM-IV symptom clusters for PTSD and depression and captured functional impairment, were organized into various domains: behavioral (for example, extreme change in activity level or excessive use of substances), emotional (for example, sadness or tearfulness, or irritability or anger), physical (for example, headaches or difficulty eating), and cognitive (for example, distressing dreams or difficulty concentrating). The Mount Sinai School of Medicine Institutional Review Board found this secondary analysis of anonymous data to be exempt.
Descriptive statistics examined patterns of referrals through time. To capture how broad an impact the event had on an individual's functioning, we created a variable indicating how many of the four categories (behavioral, emotional, physical, or cognitive) an individual's event reactions fell into (range of zero to four categories, mean±SD of 2.9±1.3 categories per client). To examine influences of time on referral process, we created hierarchical mixed regression models for nominal longitudinal data (
5 ). The first model examined the influence of demographic characteristics—gender, language preference (English versus other language), age (adult versus youth), and race or ethnicity (Caucasian, Hispanic, African American, or other)—service location (New York City versus surrounding county), risk category, and number of different event reaction categories reported. The second model included all terms in the first model plus months since September 11, 2001 (September 2001, month 0), months squared since September 11, 2001, and the interaction of each of these time terms with a variable distinguishing first versus follow-up visits.
Results
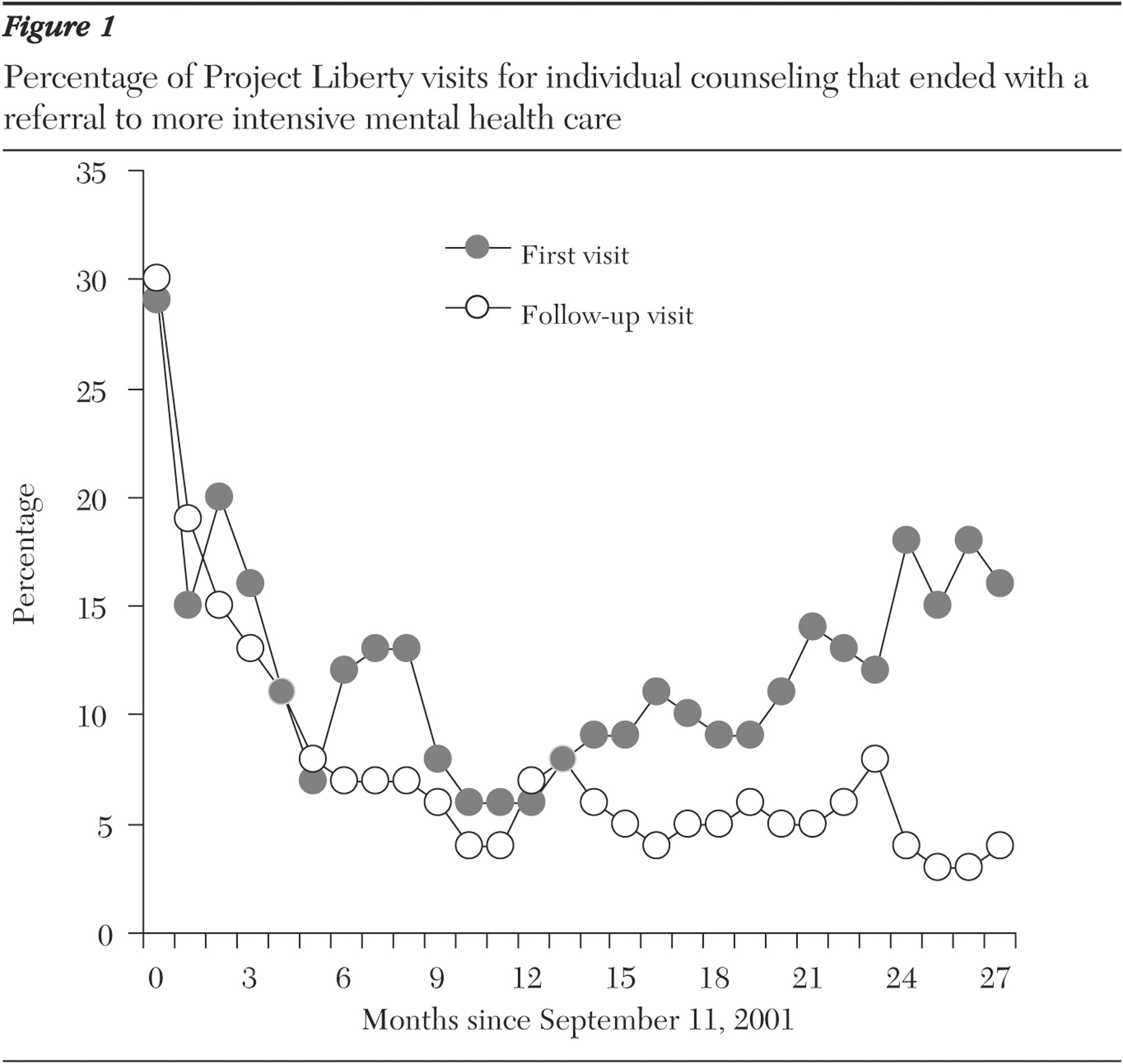
In the first year after the World Trade Center attacks, the proportion of individual counseling visits ending in referral to mental health treatment services decreased through time from about 30 to 6 percent of first visits and from 30 to 4 percent of follow-up visits (
Figure 1 ). Between one and two years after the attacks, the proportion of visits ending in a referral slowly increased to about 18 percent for first visits, while the proportion for follow-up visits remained generally steady (about 4 to 6 percent) (
Figure 1 ). Overall, 59,526 of 684,500 (9 percent) visits for individual counseling for which visit information was available (10 percent of first visits and 6 percent of follow-up visits) ended with a referral to professional mental health services.
Results of hierarchical MIXNO models indicated that the strongest predictor of receiving a referral to professional mental health services was the number of event reaction categories scored as present (z=197.2, p<.001). Referrals were received by 386 of 43,898 individuals (1 percent) with no categories, 2,977 of 77,392 (4 percent) with one category, 6,736 of 107,306 (6 percent) with two categories, 11,579 of 144,295 (8 percent) with three categories, and 37,848 of 311,609 (12 percent) with four categories. The second-strongest predictor was risk category (z=-85.2, p<.001), with the following groups accounting for more referrals: individuals who were directly affected by the attacks (persons who were injured, World Trade Center or school evacuees, World Trade Center employees absent on the day of the attack, or persons who experienced significant damage to their home) (6,447 of 49,213 persons, or 13 percent); those who were rescue or recovery workers (1,729 of 13,584, or 13 percent); those who had a physical disability or preexisting trauma, mental health, or substance abuse problem (11,843 of 94,914 persons, or 12 percent); those who experienced loss of family (4,184 of 33,830, or 12 percent); those who experienced job loss (7,985 of 69,056, or 12 percent); and uniformed personnel (8,791 of 88,566, or 10 percent). Categories of risk were hierarchic; for example, an individual who experienced both job loss and loss of family was considered to be in the latter category.
Compared with persons in the other risk categories, children categorized as belonging to the risk group of schoolchildren and members of the general population had fewer referrals (3,328 of 86,343 schoolchildren, or 4 percent, and 15,219 of 248,994 members of the general population, or 6 percent). Age was also related to referral to professional mental health services (z=66.1, p<.001), with adults being more likely than children to receive a referral (54,969 of 576,074 adults, or 10 percent, compared with 4,260 of 105,244 children, or 4 percent).
The model including time variables was significant above and beyond the model that did not include terms representing months since the World Trade Center attacks ( χ 2 =6,501.2, df=4, p<.001), indicating that time and type of visit (first or follow-up) through time exerted an independent effect above and beyond the other variables in the model (z=2.0, p<.05 for month 2, z=-40.2, p<.001 for visit type by month, and z=8.6, p<.001 for visit type by month 2 ; findings were not significant for month alone).
Discussion
These outcomes indicate that the same factors reported by Felton (
4 )—that is, more traumatic symptoms and greater exposure to the attacks—remained significant predictors of referral for more intensive treatment for up to two years after the World Trade Center attacks. Referrals after first visits followed a curvilinear pattern, with decreases across the first year and increases across the second year. This pattern is consistent with cognitive-behavioral theories that suggest that dissociation and avoidance often initially blunt deleterious consequences of PTSD (
6,
7 ). Such blunting is likely to be particularly powerful for adults in isolated life circumstances (
8 ) and for rescue responders, who function in cultures that often prohibit emotional expression (
9 ). The continued decline of referrals for follow-up visits suggests that providers quickly identified individuals who would not benefit from the brief treatment model and that they became more adept at this identification through time. The finding that children were less likely to receive referrals for professional mental health services (including medication evaluations) may indicate that children had other supports available (for example, schools and families) that increased the likelihood that they would respond to the brief treatment model. The anonymity of respondents made it impossible to link first and subsequent counseling visits, which represents a limitation of this investigation.
The widespread prevalence of PTSD after the terrorist attacks (
3 ) dictated that easily accessible brief counseling and triage services should be offered to victims immediately after a disaster. The outcomes reported here suggest three additional strategies for allocating such valuable counseling resources in future large-scale emergencies. First, given prolonged delays in the emergence of psychiatric impairment and because individuals continued to steadily exhibit symptoms consistent with depression and PTSD for two years after this event (
10 ), brief counseling and triage services should be continued for several years after a disaster. Second, both initial and continued supportive services could most profitably be targeted toward those exhibiting high current levels of impairment. Third, such services should be targeted toward police, fire, and rescue personnel, as these individuals are at heightened risk for acute stress disorder and subsequent PTSD (
9 ).
Conclusions
Individuals needing intensive mental health treatment continued to seek Project Liberty services for up to 27 months after the World Trade Center attacks. More pervasive behavioral, emotional, physical, and cognitive distress and greater attack-related exposure were temporally stable indicators of such referrals. Crisis counseling and triage services should not be limited to the period immediately after a disaster at the expense of maintaining their long-term availability.
Acknowledgments
This evaluation was funded by grant FEMA-1391-DR-NY (titled "Project Liberty: Crisis Counseling Assistance and Training Program") to New York State from the Federal Emergency Management Agency. The Center for Mental Health Services of the Substance Abuse and Mental Health Services Administration administered the grant. The authors express their appreciation to Katherine M. Shear, M.D.