Design
Details of the randomized controlled trial have been published elsewhere (
1,
2,
26,
29,
31,
32 ). The study was approved by institutional review boards at Michigan State University and the HMO. Members of the staff-model HMO were recruited during May 2000 through January 2002 and gave informed consent. Criteria included membership in the HMO for the previous two years, age between 18 and 65 years, no more than one visit per month to a mental health professional in the year before study entry, and eight or more physician office visits per year for the past two years. Using explicit guidelines (
1 ), chart raters who were clinicians identified patients with medically unexplained symptoms, which was defined as having no documented organic disease to explain symptoms of at least six months' duration. Only patients with the most severe comorbid organic diseases were excluded, which left 206 patients with medically unexplained symptoms as documented in their medical charts.
These patients were randomly assigned to treatment or usual care in the HMO. The treatment protocol was deployed by four nurse practitioners, who received 84 hours of training. The protocol emphasized the provider-patient relationship and included cognitive-behavioral therapy and pharmacological management.
Cognitive-behavioral treatment involved cognitive restructuring (including symptom diaries when indicated) and operant mechanisms tailored for busy primary care providers (for example, regularly scheduled visits and medications). To maximize other aspects of treatment (
2 ), nurse practitioners used a behaviorally defined, five-step patient-centered method to establish a positive physician-patient relationship and a three-step patient-centered method to inform and motivate patients specifically about treatment (
33,
34 ). Although they did not use a training manual, nurse practitioners carefully followed the training they received. This was ensured by periodic taped reviews of their interactions as well as individual supervision and group meetings every one to three weeks. In the analysis that corrected for baseline severity of mental dysfunction, no difference in outcomes by individual nurse practitioner was found.
The nurse practitioners also followed a collaborative stepped-care approach that has been useful in treating depression in primary care (
35 ). They took full care of the patient, including management of frequent comorbid medical conditions. Rarely, for severe problems or hospital admissions, they consulted the patient's physician. Treatment focused on both mental and physical functioning and symptoms, but the primary endpoint was improved mental health functioning. Treatment included antidepressants, reduction or elimination of controlled-substance medications that were ineffective, exercise, relaxation training, physical therapy, and management of comorbid organic diseases. Most referrals were to mental health professionals, usually for improved patients who would benefit from counseling. Treatment entailed 12 scheduled patient visits with the nurse practitioner (20 minutes each) in weeks 1, 2, 3, 5, 8, 12, 16, 22, 28, 36, 44, and 52, but additional visits could occur. Telephone contact (from five to ten minutes) was scheduled between visits.
Patients in the control group received usual care from 21 HMO physicians and had their usual access to mental health professionals.
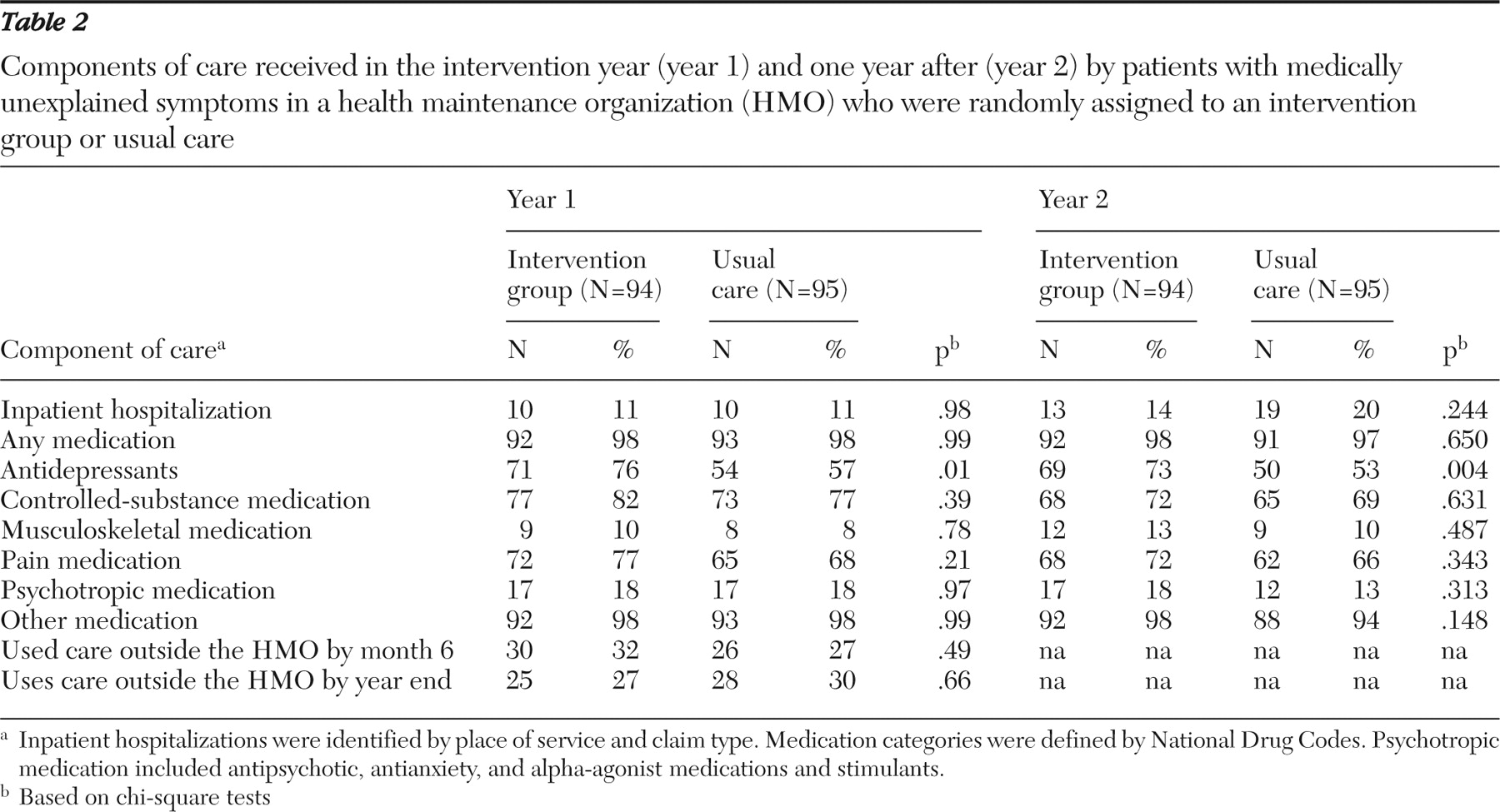
Outcomes were assessed by independent evaluators. For these patients, clinically significant improvement in the Mental Component Summary of the 36-item Short Form from the Medical Outcomes Study (SF-36) was found and reported elsewhere; in addition, depression, physical disability, and satisfaction with providers all improved, and there was an increase in use of antidepressants and a decrease in the use of addicting agents (narcotics, tranquilizers, and sleeping pills) (
29 ).
Measurements of costs
Much of the primary care for the study participants was provided by HMO staff at the HMO facilities. However, many services were also purchased by the HMO from outside providers—including, for example, all inpatient hospital care. We used data on costs from the HMO's electronic management information system. For each participant, we used information on services delivered during the year that the individual was enrolled in the study. Costs are reported in current dollars from the time of the study.
In analyzing costs our intent was to measure the value of the resources used to deliver medical care to study participants. For services purchased by the HMO, such as outside referrals (which may have included psychiatric care), we documented the amount that the provider was paid, inclusive of patient copayments. We took this amount as our approximation of the resource costs of services. For services provided within the HMO, the management information system indicated the amount that an outside provider would have been paid for the same service. We used this information to approximate the costs of such in-house services. Because of a lack of data, we did not attempt to measure the costs of participants' time associated with receipt of services.
The intervention used nurse practitioners as primary care providers, but we calculated costs as though services were delivered by physicians. That is, the cost allocated to a particular type of visit at the HMO was treated as the same regardless of the provider type. Because nurse practitioner time has a lower cost than physician time, this approach may bias the comparison against the intervention. However, the intervention protocol requires regular meetings between nurse practitioners and physician supervisors (
7 ) that were not separately accounted for in the cost analysis, and nurse practitioners' time spent on phone contacts with participants was also not included, because phone calls to patients were not recorded in the management information system. We believe the omission of meeting time and phone contact roughly offsets the failure to account for the lower cost of nurse practitioner time.
Although one of the criteria for inclusion in the study was that a participant expected to be a member of the HMO for at least one year after entering the study, participants who were not covered by the HMO during part of the 12-month period were included in the randomized controlled trial. However, because information on their use of services was incomplete or absent from the management information system, we excluded them (four in the treatment group and seven in usual care) from the cost analysis.
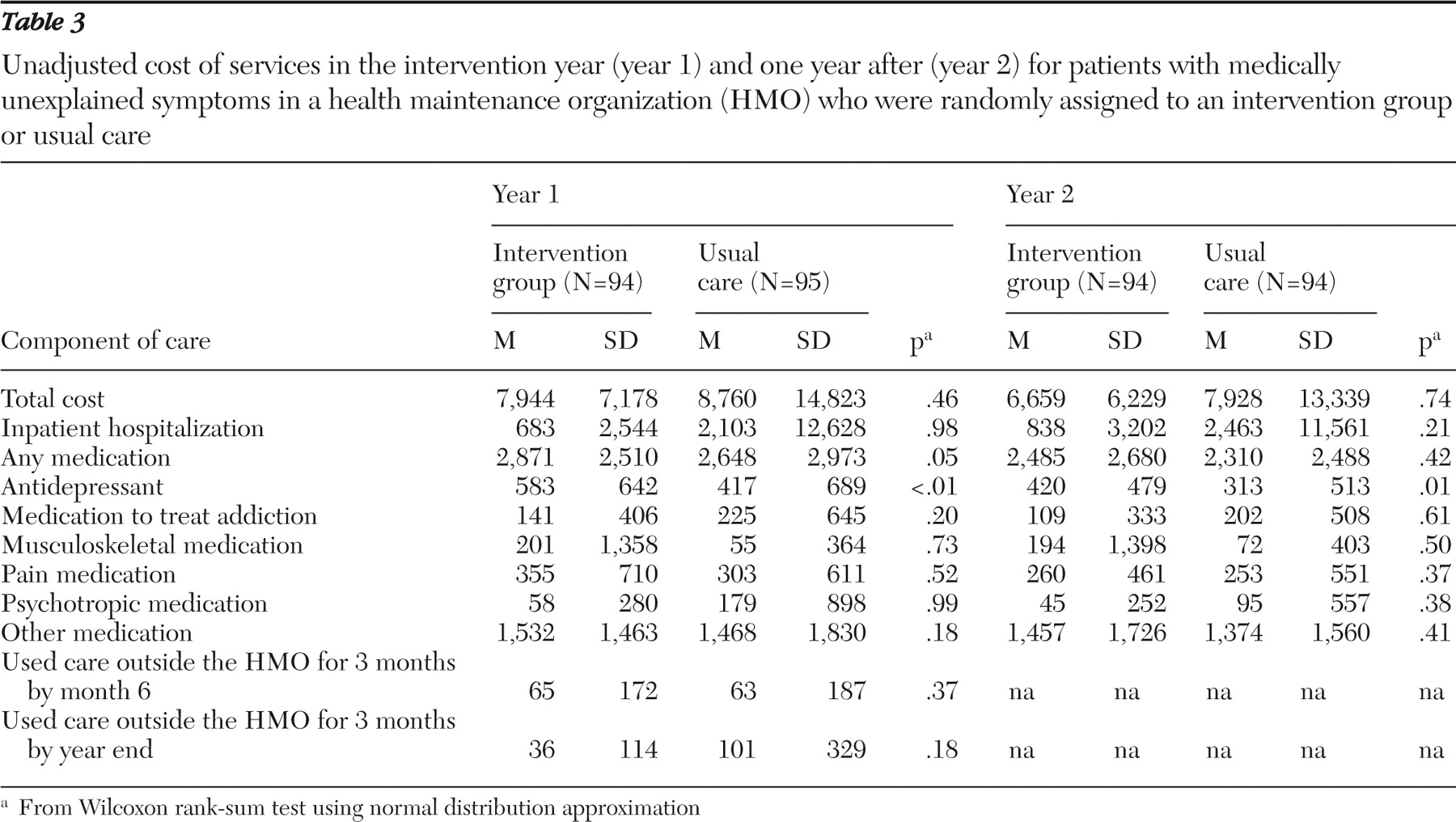
In addition to examining total costs of services, we looked at several components: costs associated with inpatient hospitalizations, all other costs (that is, other than for hospitalization), and costs for medications. We categorized medications by the National Drug Code into six groups: antidepressants, controlled-substance medications, musculoskeletal medications, pain medications, psychotropic medications (including antipsychotic, antianxiety, and alpha-agonist medications and stimulants), and others.
To capture health care utilization outside the HMO, at six- and 12-month follow-ups we asked the participants whether in the past three months they had any visits to other physicians for medical consultations, second opinions, or ongoing medical treatment; counseling of any type; visits to a chiropractor; visits to an urgent care facility; visits to an emergency room; diagnostic tests (such as blood tests and x-rays); acupuncture treatments; pain treatments; hypnosis; biofeedback sessions; or outpatient surgery or treatment that were not covered or authorized by the network. We then aggregated the corresponding out-of-pocket cost for these visits.
Statistical analysis
In addition to the 11 patients excluded for lack of cost data, six participants (three in each group) did not complete the study and were excluded from the analysis, leaving a total sample of 189 patients. Baseline characteristics of patients were compared by using the t test for continuous variables and the chi square test for categorical variables. For costs we used the Wilcoxon rank-sum test.
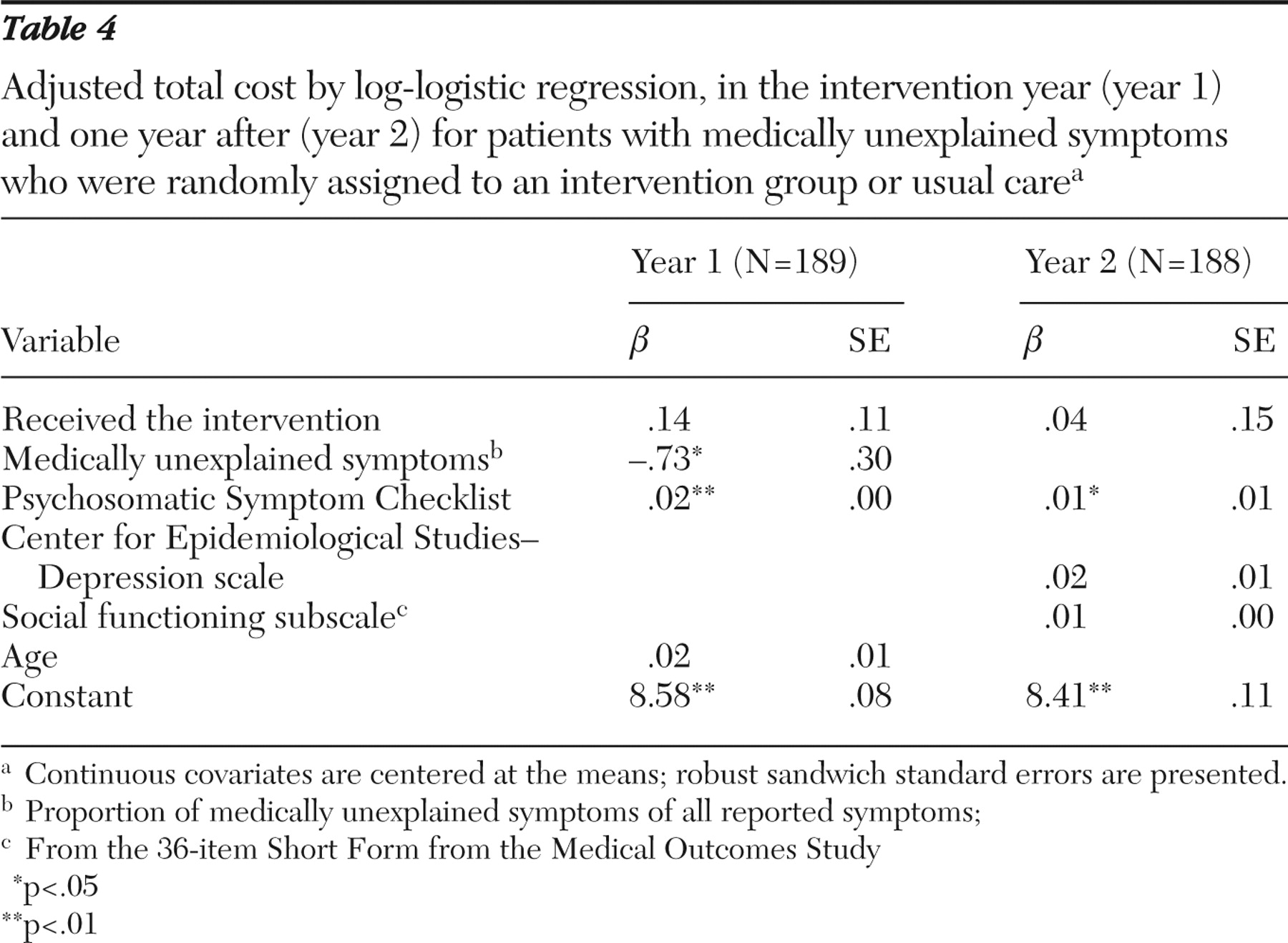
As is very common with health care data, our cost distributions were skewed to the right. To mitigate the influence of skewness and outlying observations, we assumed a log-normal or log-logistic distribution to model total cost. In our sample, total cost was positive for all patients. There was one extreme outlier in the control group in the distribution of total costs (primarily attributable to hospital costs of $119,202). Covariates considered for inclusion in the model of costs were age at study entry, sex, marital status, education level (16 or more years of formal schooling compared with less than 16 years), eight subscales from the SF-36 (mental health, emotional role, social functioning, vitality, general health, bodily pain, physical role, and physical functioning), score on the Center for Epidemiological Studies-Depression scale (CES-D), the state anxiety scale of the Spielberger State Anxiety Inventory (STAI), the proportion of reported medically unexplained symptoms among all symptoms, and the score on the Psychosomatic Symptom Checklist. The mental component summary and physical component summary of the SF-36 were highly correlated with the eight SF-36 subscales and were not used in variable selections. Maximum likelihood estimation methods were used, and the choice of models was based on the Akaike information criterion.
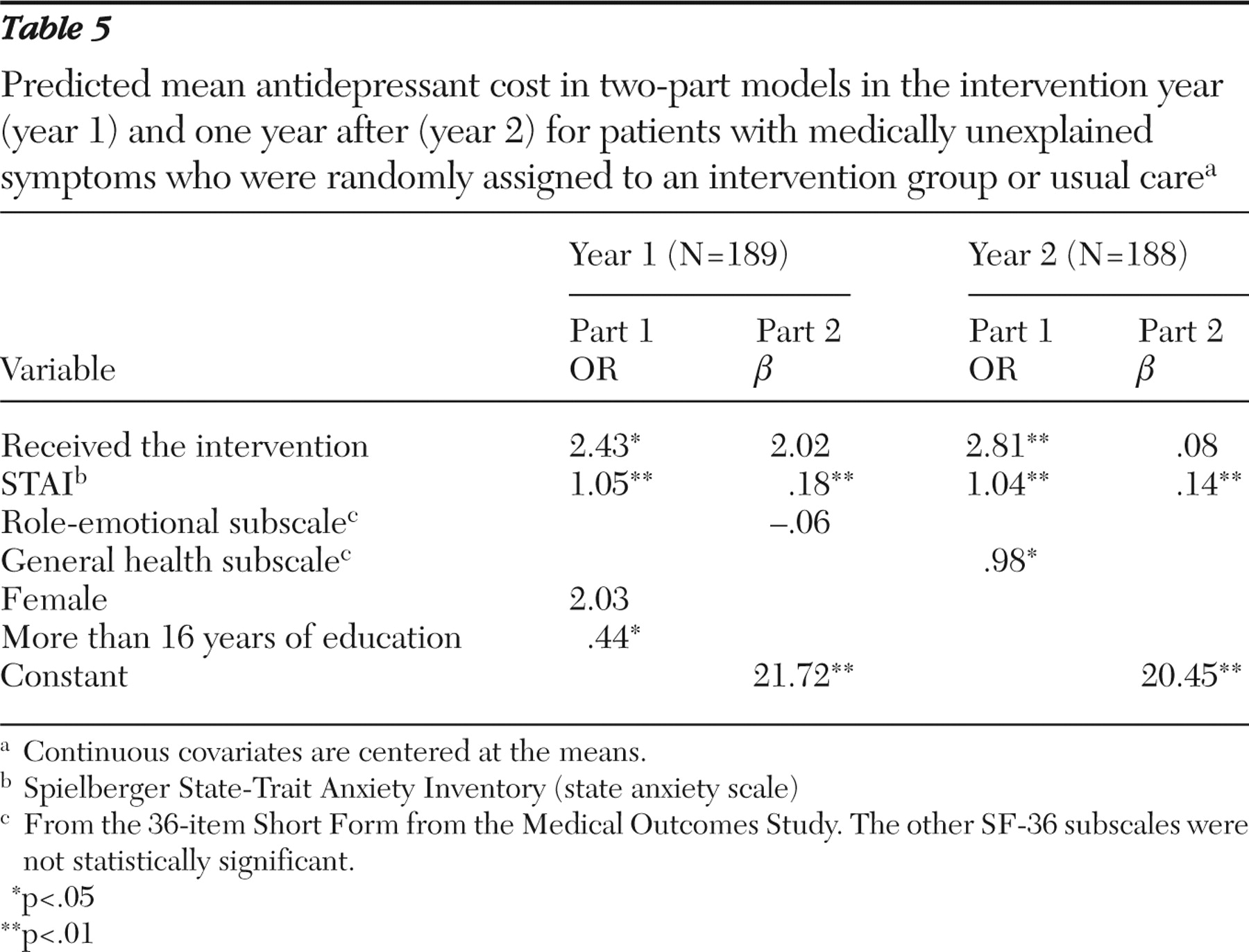
Because promoting appropriate use of antidepressants was a key aim of the multifaceted intervention and there was no difference in use of other categories of medication (such as controlled substances or musculoskeletal or pain medication), we focused on the cost of antidepressant use in the study. A substantial proportion of patients were not prescribed antidepressants and incurred no cost for antidepressants. Application of the usual statistical regression methods, such as ordinary least squares, to the whole sample or log-normal models to nonzero part of the sample raises the possibility of bias.
Because our aim was to understand the actual expenditure from a budgetary standpoint, we used a two-part model to handle the clustering of zeros (
36 ). In the first part of the two-part model we used logistic regression to estimate the probability of positive antidepressant cost. For the second part of the two-part model, we used linear, square-root or logarithm transformations for positive costs. The square-root transformation outperformed the other specifications. In this case, the estimated mean of antidepressant costs Y combined the two parts of the model; that is, a logit model for part 1: P(Y<0|x
1 )={1+exp (-x
1 ′
β 1 )}
-1 and a linear predication for the transformed costs for part 2: E(Y|Y< 0,x
2 )=(x
2 ′
β 2 )
2 +
σ 2, where
σ 2 is the conditional variance of √Y. We get E(Y|x)={(x
2 ′
β 2 )
2 +
σ 2 }{1+exp(-x
1 ′
β 1 )}
-1 . For each part of the two-part model we used stepwise selection methods to choose potential covariates from the list of covariates above. Only statistically significant covariates and the intervention dummy are reported in the final model.