In addition to its primary function of stabilizing the condition of critically ill and injured patients, the medical emergency department often serves as the sole provider of primary care services for the uninsured and underinsured in the United States (
1 ). Several reports indicate that hospital emergency departments in the United States and other countries are also having to contend with a substantial and disproportionate increase in the number of patients seeking treatment for psychiatric disorders (
2,
3,
4,
5 ). Using data from the National Hospital Ambulatory Medical Care Survey (NHAMCS), Larkin and colleagues (
4 ) estimated that the number of emergency department visits for mental health problems increased by nearly 40% between 1992 and 2000, compared with an increase in overall emergency department visits of only 20%. This increase in psychiatry-related emergency visits may be a result of multiple factors, ranging from the effects of deinstitutionalization to inadequate funding for community-based mental health and substance abuse services (
3,
4,
5 ).
One of the challenges confronting medical emergency departments is how to accurately identify and appropriately manage patients with mental health problems who are frequent users of their services. Several studies have found that persons with psychiatric disorders account for a large proportion of the population who make multiple return visits to the hospital emergency department (
6,
7,
8 ). Uninsured patients with mental health problems may represent a high-risk group for heavy use of the medical emergency department because they face substantial barriers in accessing conventional psychiatric services (
3,
9 ). Hence, identifying the clinical and demographic correlates of emergency department usage by uninsured patients with mental disorders may be of value in developing more effective strategies to meet the health care needs of this growing segment of the U.S. population. We conducted a retrospective study to determine the prevalence of psychiatric disorders in a large cohort of uninsured patients treated in the medical emergency department of an academic medical center in Texas, the state with the highest percentage of uninsured persons in the United States (
10 ). We also examined whether a diagnosis of a mental disorder was associated with an increased risk of making multiple visits to the emergency department or being admitted to the hospital from the emergency department.
Methods
The primary source of data for the study was an administrative database maintained by the University of Texas Medical Branch (UTMB) Department of Finance. Permission to use these data for analysis and publication was granted by the UTMB Institutional Review Board. The study population consisted of all uninsured patients (N=15,672) who made at least one visit to the UTMB emergency room and trauma center in Galveston between September 1, 2005, and August 31, 2006. Patients insured by public programs (Medicaid or Medicare) were not included in the study.
The UTMB emergency department serves as a regional level 1 trauma center for a nine-county area in southeast Texas and provides emergency care for most indigent patients in Galveston County. Although a designated psychiatric holding area was not available in the emergency department during the entire span of the study period, a psychiatrist and psychiatric nurse practitioner were always available to provide psychiatric consultations. All diagnoses of a psychiatric disorder established during an emergency department visit were made by a board-certified psychiatrist. Both pediatric and adult patients who required inpatient treatment for a psychiatric disorder at the time of their emergency department visit were typically admitted to the university's psychiatric hospital.
Diagnoses of all medical and psychiatric conditions, established at the time of the emergency visit, were classified according to the International Classification of Diseases ( ICD-9 ) coding system. For this study, patients were classified as having a psychiatric disorder if either a primary or secondary diagnosis of a mental disorder was recorded during at least one emergency department visit. A psychiatric visit was considered to have occurred if a diagnosis of mental illness was made during the visit.
The following ICD-9 categories of psychiatric disorders were used in this investigation. Anxiety disorders included diagnoses of all anxiety disorders, including dissociative, somatoform, and phobic disorders ( ICD-9 9 codes beginning with 300). Bipolar disorder included diagnoses of mania or bipolar disorders of any type ( ICD-9 codes 296.0, 296.1, and 296.4– 296.8). Depressive disorders included diagnoses of depressive disorders ranging from dysthymia to major depression ( ICD-9 codes 296.2, 296.3, 300.4, and 311). Psychotic disorders included diagnoses of schizophrenia, schizoaffective disorder, and psychosis not otherwise specified ( ICD-9 codes 295, 297, and 298). Substance use disorders included diagnoses of substance-induced psychotic disorders, substance dependence, and substance abuse ( ICD-9 codes 291, 292, and 303–305).
Prevalence odds ratios (ORs) and associated 95% confidence intervals (CIs), which were calculated with bivariate logistic regression models, were used to assess the association of demographic factors (age, race, and gender) with the prevalence of all psychiatric disorders as well as each of the five master categories of disorders. In addition, multivariate logistic regression models were used to examine the association of each psychiatric disorder—adjusted for age, race, and gender—with the following dichotomous response variables during the 12-month study period: two or more emergency department visits, three or more emergency department visits, four or more emergency department visits, and hospitalization for any medical or psychiatric condition immediately after the emergency department visit. Nonoverlapping CIs were considered statistically significant. Statistical analyses were conducted with SAS software, version 8.2.
Results
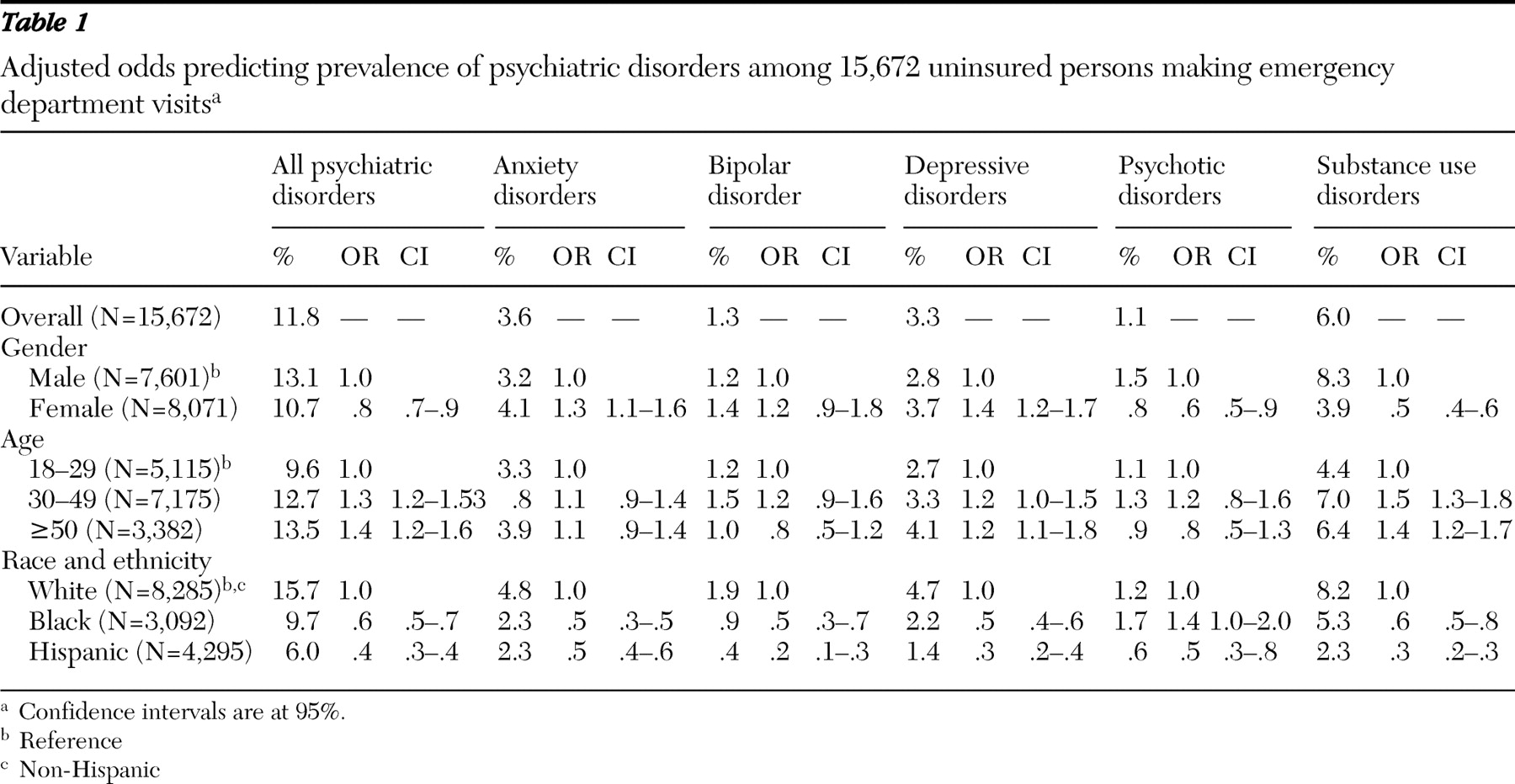
The prevalence ORs and adjusted prevalence ORs for diagnosis of a psychiatric disorder during an emergency department visit are presented in
Table 1 according to demographic characteristics. Overall 11.8% (1,849 admissions) of the study population was diagnosed as having at least one psychiatric disorder during an emergency department visit. The likelihood of presenting to the emergency department with a psychiatric disorder was lower among women and persons who were black or Hispanic and increased linearly with age. The prevalence of several categories of psychiatric disorders also varied according to demographic characteristics (
Table 1 ).
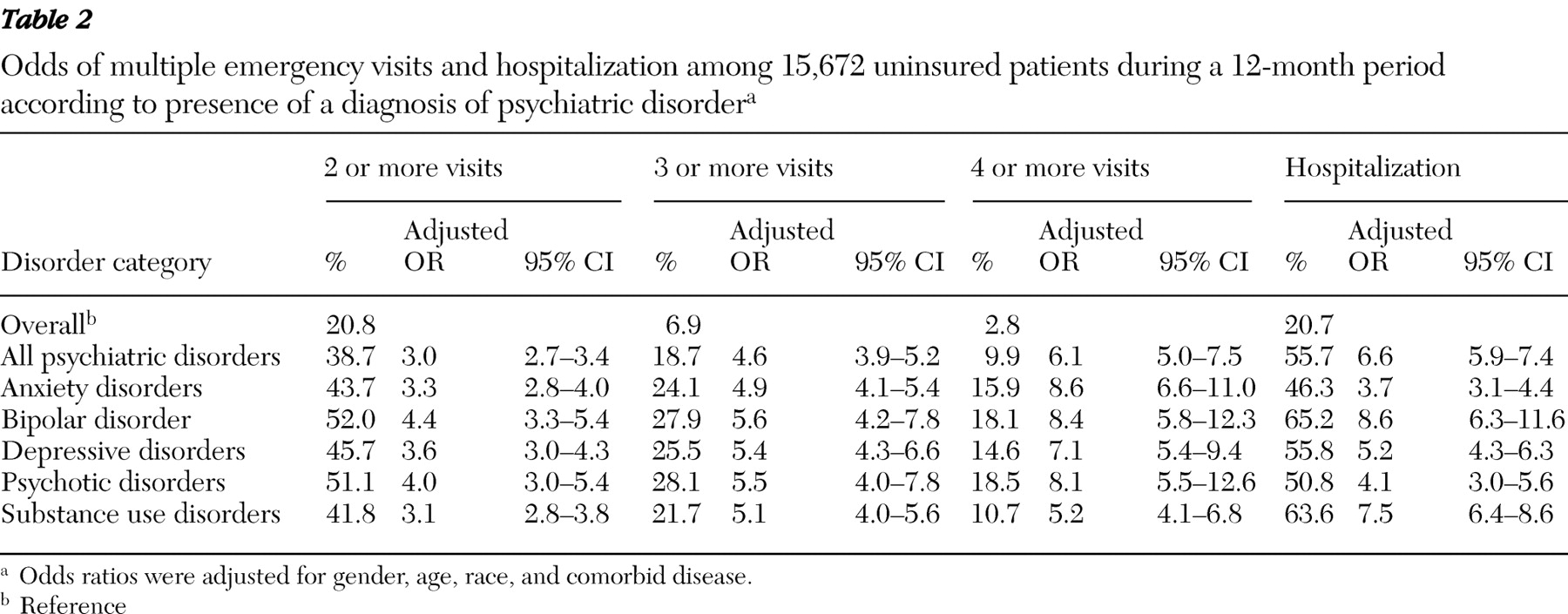
A total of 3,257 patients (21%) made multiple emergency department visits during the 12-month study period. Among the subgroup of 1,856 patients with at least one psychiatric disorder, 719 patients (39%) made multiple emergency department visits. The likelihood of uninsured patients having multiple emergency department visits is presented in
Table 2 according to the six categories of mental disorder. Compared with the total study population, patients with a diagnosis of any psychiatric disorder had a substantially increased risk of having multiple emergency department visits. This association persisted across all three of the dependent variables, which assessed different thresholds in the total number of emergency department visits: two or more, three or more, and four or more visits. Using each of the three outcomes, we found the risk of multiple emergency department visits was particularly elevated for patients with bipolar disorder and psychotic disorders.
Table 2 also shows the likelihood of being hospitalized for either medical or psychiatric problems after an emergency department visit. Patients with any psychiatric disorder had a substantially increased risk of being hospitalized. This risk was especially high for patients with bipolar disorder or substance use disorders.
We also examined the percentage of return emergency department visits that were not related to psychiatric disorders. For 3,257 patients with two or more emergency department visits during the study period, 85.9% of the return visits were unrelated to psychiatric disorders. For the 719 patients in this subgroup with a diagnosis of at least one psychiatric disorder, 48.3% of return emergency visits were unrelated to mental health problems. Only a few diagnostic categories indicated substantial variation from this percentage. Patients with a diagnosis of either bipolar disorder (N=106) or a psychotic disorder (N=178) had a lower proportion of return visits unrelated to mental illness (38.4% and 31.2% of return emergency visits, respectively), whereas patients with anxiety disorders (N=568) had the highest (45.3%).
Discussion
In our study, a substantial proportion of uninsured adults who visited the medical emergency department were treated for a psychiatric disorder during their visit. In addition, a significant number of these patients made multiple visits to the emergency department within a 12-month period or were hospitalized after a visit. Our finding that 11.8% of our uninsured patients received a diagnosis of at least one psychiatric disorder during an emergency department visit is substantially higher than the rate of 3.3% estimated by Hazlett and colleagues (
3 ), who used data that were from the NHAMCS emergency department survey conducted in 2000. This disparity may be attributable to several factors. First, the NHAMCS data were limited to no more than three
ICD-9 codes per patient, whereas our study relied on up to 15 codes. Also, time-related trends in the financing and delivery of health care in the United States may have contributed to the higher rates of psychiatric disorders in our study; the NHAMCS data were collected between 1992 and 2000, whereas our data were collected between 2005 and 2006. Finally, differences in race and ethnicity as well as regional disparities in access to mental health resources across the two studies may have contributed to differential patterns of care-seeking behavior.
Our study also differed from that of Hazlett and colleagues (
3 ) in terms of the demographic distribution of psychiatric disorders. Whereas our study showed lower rates of psychiatric disorders among women and persons who were black or Hispanic and showed a linear increase according to age, the prior study found no difference according to gender, elevated rates among the black population, and no linear increase according to age. It is important to point out, however, that the inclusion of all insurance groups (including private insurance, Medicaid, and Medicare) in the study by Hazlett and colleagues significantly limits comparability with our study. Also, because Texas has the highest rate (24%) of uninsured persons in the United States (
10 ), our study population may not be representative of the overall national population of uninsured emergency department patients.
Our study showed that patients with psychiatric disorders had consistently elevated rates of multiple emergency department visits. This finding persisted across all psychiatric disorders but was particularly elevated for patients with bipolar disorder and psychotic disorders. Other investigators have reported that patients with psychotic disorders, particularly schizophrenia, are at high risk for multiple visits to psychiatric emergency departments (
6,
7 ). A number of behavioral, social, and biological mechanisms may underlie this association. In view of this, future investigators will need to carefully and prospectively examine the specific pathways that lead to increased emergency department use among patients with psychotic disorders.
Although several studies have examined the demographic and clinical profiles of persons who make multiple visits to psychiatric emergency departments (
11,
12,
13,
14 ), little information is available on the proportion of medical emergency department return visits that were unrelated to mental health conditions of patients with preexisting psychiatric disorders. We believe it is noteworthy that 48.3% of the return emergency department visits among our patients with psychiatric disorders were unrelated to mental health conditions. As expected, patients with psychotic disorders and bipolar disorder had the lowest proportion of return visits that were not related to psychiatric disorders, whereas patients with anxiety disorders and substance use disorders had the highest. In view of this, it may be beneficial to focus on patients with psychiatric disorders, particularly those with anxiety and substance use disorders, for screening and subsequent case management or chronic care programs.
The results of this study should be interpreted in the context of several limitations. First, the ability to draw general inferences or conclusions from our findings is limited by our reliance on data from a single financial class of patients (the uninsured) drawn from a relatively small geographic location. In addition, it is difficult to determine the extent to which the unique distribution of mental health care services available to uninsured patients in this particular region has altered the profile of our emergency department study population. Although low external validity is a threat to any regionally limited sample, our ability to access linked patient records over time may provide information about patterns of return emergency department visits that are not discernible with use of NHAMCS data or other national data sets that mask patients' identity. Second, as with any study using a large administrative database, we were unable to examine some of the important behavioral and social characteristics that may have accounted for the observed racial and age disparities in disease profiles, repeat emergency department visits, and hospitalizations. It will be important for future prospective studies to directly assess these factors. Another limitation is that we were unable to identify the subgroup of our cohort who were homeless. It is possible that the high rates of psychiatric disorders in our study were concentrated among homeless patients. Understanding the disease profile in this subgroup of uninsured emergency department patients merits further investigation.
Previous investigations have shown that persons with psychiatric disorders account for a significant proportion of the patient population who are heavy users of the medical emergency department. This brief report adds to this research by examining the patterns of emergency department use among a specific subgroup of patients with mental illness—those without health insurance. Continued research in this area has the potential to increase our understanding of the complex factors associated with repeat emergency department visits among patients with mental illness.
Acknowledgments and disclosures
Leonard Pechacek assisted in writing and editing this article.
The authors report no competing interests.