Persons with schizophrenia have higher rates of medical illness, greater severity of their medical conditions, more untreated disorders, and higher mortality rates than their age peers without schizophrenia (
1,
2 ). Although increasing age is associated with worsening health status, there have been few studies devoted to examining the health care of older patients with schizophrenia. Four-fifths of older persons with schizophrenia rank improving their physical health as a high priority (
3 ). Nevertheless, there is evidence that this group may be at risk of undetected or inadequately treated medical conditions (
4,
5 ).
Among older persons, there is a complex interplay between co-occurring medical illness and schizophrenia. Because mortality rates are higher among younger persons with schizophrenia than their age peers without the disorder, older adults with schizophrenia may be hardy survivors, although they still have somewhat higher mortality and morbidity from medical illness than the general population (
5,
6 ). Notably, older patients with schizophrenia compared with age peers without the disorder tend to experience greater severity of their medical disorders rather than a greater number of illnesses (
4 ). It is unclear to what extent this difference in illness severity represents the effect of proportionately more unhealthy behaviors among persons with schizophrenia (
7 ), the consequence of the cognitive and behavioral features of the disorder (
8 ), greater problems with medication compliance (
8 ), poor communication or interactions with health providers (
8 ), lack of an adequate social support system (
9 ), or the lack of tangible aid necessary to secure appropriate health care.
In this study, using an adaptation of Krause's model of illness behavior in later life (
10 ), we examined some of the elements that may account for inadequate medical treatment among older adults with schizophrenia. Earlier studies have not used a theoretical model to examine the behavior of individuals in this population in relation to their having a physical illness. A theoretical model has the advantage of allowing for the inclusion of predictor variables, the concurrent examination of multiple variables, and generalization across samples. Krause observed that the most popular models of illness behavior (that is, how persons perceive, evaluate, and act on health symptoms)—the health beliefs model (
11 ) and the health behavioral model (
12 )—share a nucleus of common constructs, including the importance of perceived illness symptoms, demographic and economic factors, social support, and the perceived efficacy of medical care. Using findings from the gerontology literature, Krause has proposed a preliminary model for older adults in which these constructs are bound together by the integration of the role of life stress. The latter is thought to affect physical illness as well as elicit responses from the individual's social network with respect to emotional, informational, and tangible support. Although the endpoint in Krause's model is formal medical care, the use of informal care and self-care is also considered.
Finally, much of the literature examining the relationship between aging, schizophrenia, and medical illness has been limited by the use of specialized centers such as Veterans Affairs medical centers, nursing homes, or residential treatment facilities, and many of the studies have been conducted in one geographical area (San Diego County) (
4,
5,
6 ). Moreover, these studies have not included a culturally and economically diverse sample, and there is a lack of comparative data between community-dwelling older persons with and without mental illness.
Thus in this study we addressed some of the limitations in the literature by using a theoretical model of health behavior among older persons and a large multiethnic urban population in the northeastern United States to examine the care of four medical illnesses among older persons with schizophrenia, specifically, heart disease, gastrointestinal ulcers, diabetes mellitus, and hypertension. In so doing we aimed to answer two questions. First, are there differences in the adequacy of medication treatment of these four conditions between older patients with schizophrenia and a community comparison group? Second, among patients with schizophrenia, what factors are associated with higher adequacy of medication treatment rates for these conditions?
Methods
This study was part of a larger study that has examined various measures of clinical and social well-being and service utilization among older adults with schizophrenia that was conducted from 2002 to 2004. Participants were age 55 and over and developed schizophrenia before the age of 45 and lived in the community. We used stratified convenience sampling in which we attempted to recruit approximately half the participants from outpatient clinics and day treatment programs and the other half from supported community residences. The latter sample included sites with varying degrees of on-site supervision. Inclusion was based on having an existing
DSM-IV diagnosis of schizophrenia or schizoaffective disorder that was determined by agency clinical staff and by a lifetime illness review adapted from Jeste and associates (
13 ). Persons with cognitive impairment too severe to complete the questionnaire were excluded from the study, and the threshold for this was defined as scores of 5 or less on the Mental Status Questionnaire (
14 ).
A community comparison group was recruited with the use of Wessex Census Summary Tape File 3 of Kings County (Brooklyn, New York). Records of persons 55 years of age and over were extracted. A computer program was written to randomly select without-replacement block groups as the primary sampling unit. Without-replacement sampling was used to avoid unnecessary duplication of effort and waste of resources. An effort was made to interview all persons in a selected block group by knocking on doors. In order to enhance response rates, participants from the selected block group were also recruited at senior centers, churches, and through personal references. Persons were excluded if they reported a history of outpatient treatment or hospitalization for schizophrenia or schizoaffective disorder.
Participants were offered $75 for completing the 2.5-hour interview. The rejection rate was 7% in the schizophrenia group and 48% of those contacted in the community group. The schizophrenia sample consisted of 198 persons. Among the latter, 39% were living independently in the community and 61% in supported community residences. From the original community sample of 206 residents, we selected 113 persons who more closely matched the schizophrenia sample for age, gender, and race. Because the initial community comparison group had disproportionately more African Americans and women, matching was done manually in the following order: race, gender, and age. Forty-nine percent of both the schizophrenia and the community comparison groups were women, and 35% of the schizophrenia group was African American versus 36% of the community group. These differences between groups for gender and race were not statistically significant. The mean±SD ages of the schizophrenia and community comparison groups were 61.5±5.6 and 63.0±5.4 years, respectively (t=2.37, df=306, p=.02). Thus this small absolute difference in age between the two groups still attained statistical significance. Median income for both groups fell within the same category ($7,000–$12,999).
After providing a description of the study to the participants, we obtained written informed consent. The institutional review boards of Long Island University and the State University of New York Downstate Medical Center approved this study.
Instruments
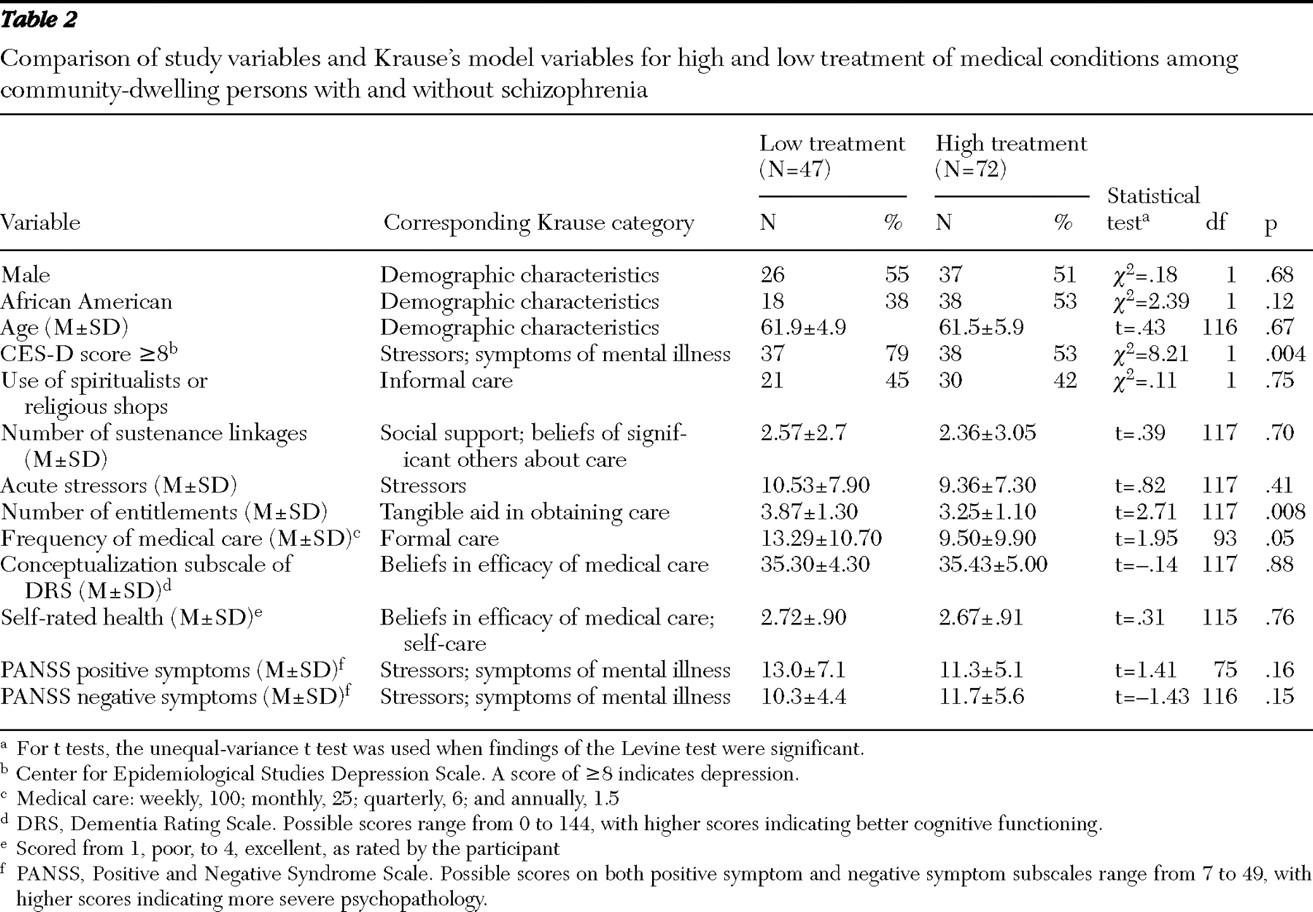
We adapted Krause's model, which includes ten categories that are postulated to influence illness behavior of older adults: demographic characteristics, acute stressors, social support, symptoms of illness, beliefs about illness by significant others, personal beliefs about medical care, aid in obtaining medical care, self-care, informal care, and formal care. We operationalized the model into one dependent variable and 13 independent variables that reflected the ten categories proposed by this model (see Table 2, discussed below, for variables and categories). These independent variables were selected on the basis of their theoretical importance in the model as well as their having been identified in the literature as affecting the use of formal health services. The sample size also posed limitations on the number of independent variables. Stress was assessed with the Acute Stressors Scale (
15 ), which consisted of 11 possible events experienced within the "last month or so" and the degree of stress that was experienced, rated from 0, none, to 3, very much. Because we were focusing on a population with schizophrenia, we included measures of psychopathology. We considered these variables to be part of the stress-related category of the model, although they also might be viewed as a separate category.
We assessed depression with the Center for Epidemiological Studies Depression Scale (CES-D) (
16 ), which was dichotomized into depressed (syndromal or subsyndromal levels) and not depressed on the basis of a score of ≥8, which indicates depression (
17 ). We assessed positive and negative symptoms of schizophrenia using the Positive and Negative Syndrome Scale (PANSS) (
18 ), which contains items for seven positive symptoms and seven negative symptoms. We selected self-rated health as the indicator of perceived health difficulties because it had the highest intercorrelations (r=.08 for positive self-rated health and .33 for negative self-rated health) among the other potential measures (instrumental activities of daily living and the number of physical disorders); it was rated on a 4-point scale from 1, poor, to 4, excellent.
In the model the category to assess beliefs in the efficacy of medical care consisted of two variables. Frequency of medical care (other than a psychiatrist) was scored as follows: daily, 7.0; weekly, 1.0; monthly .25; and quarterly, .625, and so forth. These scores were then multiplied by 100 for analytic purposes. The second variable in this category was the conceptualization subscale of the Dementia Rating Scale (
19 ), which was used to assess any changes in reasoning ability that are postulated to occur with increased stress (
10 ). We assessed the categories of stress-focused support and belief in medical care by significant others by using the Network Analysis Profile (
20 ), which generated a measure of the number of persons in the participants' social networks who assisted them with food or money or in times of illness. To assess tangible aid, we used the summed score of the total number of entitlements received from a list of 13 possible items. We assessed informal care by asking whether the respondent saw a spiritualist or purchased items from a religious shop or botanica.
We included three demographic variables—age, race, and gender. We did not specifically examine self-care, although persons who did not use informal care and went infrequently to their physicians may have been using more self-care. The internal reliability (Cronbach's alpha) scores for the scales were as follows: CES-D, .88; PANSS positive scale, .83; PANSS negative scale, .78; Dementia Rating Scale, .89; and the Acute Stressors Scale, .88. All scales attained recommended alphas of .60 or higher.
On the basis of a literature review, we identified four common medical conditions—diabetes mellitus (
21 ), hypertension (
21 ), heart disease (
22 ), and gastrointestinal ulcers (
23 ) —that are among the common causes for mortality and morbidity of persons with mental illness. Treatment of these conditions formed the basis for our dependent variable. We used a self-report instrument to elicit whether a person had one or more of these medical disorders and whether he or she had received medication treatment for them. Previous investigators have demonstrated acceptable accuracy and validity of self-report measures for study of health and symptom domains among patients with schizophrenia (
24,
25 ). None of the four conditions were objectively defined. Physical examination or laboratory tests were not done to confirm diagnosis. The dependent variable for this study was based on dichotomizing the sample into persons who reported receiving medication treatment for all of the conditions that they had (high-treatment group) and those who reported not receiving medication treatment for one or more of these conditions (low-treatment group). We opted to use medication as the indicator of treatment because it is an empirical marker.
Interviewers were trained via audiotapes and videotapes, and they were generally matched to respondents from similar ethnic backgrounds. Interviewers were periodically monitored with audiotapes. The intraclass correlation coefficients ranged from .79 to .99 on the various scales. Raters had a mean of 99% and 94% agreement with ratings by the expert (author CIC) on the physical illness score and the network profile contact scores, respectively.
Data analysis
We compared the schizophrenia and comparison groups with chi square tests for categorical variables and t tests for continuous variables. Initially, for the schizophrenia group, we examined the 13 independent variables in our model associated with being in the two treatment groups by using bivariate tests for categorical variables and t tests for continuous variables. For t tests the unequal-variance test was used when findings of the Levine test were significant. We used logistic regression analysis to examine concurrent association of the independent variables with treatment adequacy. There was no evidence of colinearity among the independent variables; that is, all variance inflation factors were less than 2.5, with ten variables below 1.5. Inflation factors greater than 5.0 suggest high colinearity (
26 ). Because multiple comparisons were used in the bivariate and multivariate model testing, we used a significance level of p<.01. For other analyses, we used a significance level of p<.05.
Results
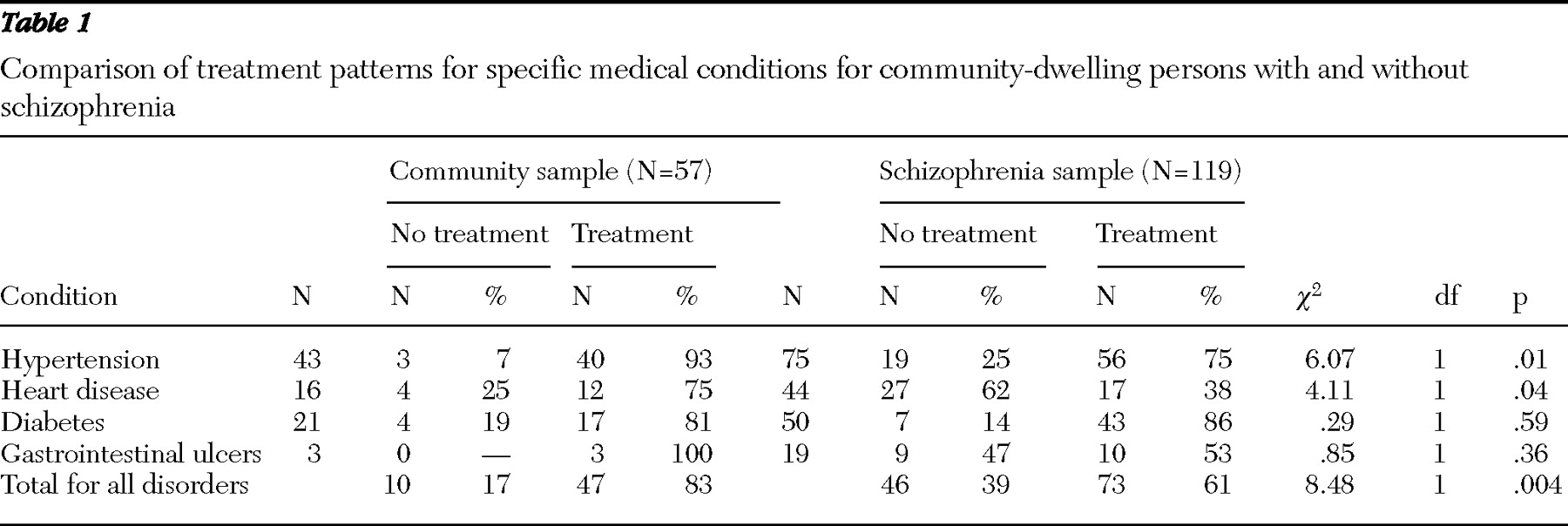
We reviewed schizophrenia and comparison groups for presence of at least one of four medical disorders (heart disease, hypertension, diabetes, or gastrointestinal ulcers). We identified 119 persons with schizophrenia (60% of the schizophrenia sample) and 57 persons in the community without schizophrenia (50% of the community sample) who had at least one medical condition. The mean number of the four possible physical disorders was 1.5±.7 and 1.6±.8 for the schizophrenia and community comparison groups, respectively. The difference between the groups was not statistically significant. As evident in
Table 1, the percentage of persons in the schizophrenia group who received treatment for their hypertension was 75%; for heart disease, 38%; for diabetes, 86%, and for gastrointestinal ulcers, 53%. The percentage of persons in the community comparison group receiving treatment for these conditions was 93%, 75%, 81%, and 100%, respectively. Thus the community comparison group reported higher rates of treatment for three of the four conditions, and for two conditions, hypertension and heart disease, this difference attained statistical significance. Of note is that for diabetes, the patients with schizophrenia had a higher rate of treatment than the community group, but this difference was not statistically significant.
When the two groups were compared with respect to the percentage of persons receiving treatment for all of their conditions, 83% of participants in the comparison group versus 61% of the schizophrenia group reported being in the high-treatment category; the difference between the groups was significant (
Table 1 ). There were no differences between the schizophrenia and community groups in the number of visits to a physician for physical problems during the past 12 months. The number of persons seeing a physician three or more times, one or two times, or not at all were 83 (70%), 27 (23%), and nine (8%) for the schizophrenia group and 40 (70%), nine (16%), and eight (14%), respectively, for the community group.
Next, we separately analyzed data from the schizophrenia group. There was no difference in the mean number of the four possible disorders between the two treatment groups: 1.5 for the low-treatment group and 1.6 for the high-treatment group. In bivariate analysis, only three of the 13 variables in the model—lower levels of clinical depression, fewer visits to physicians, and fewer entitlements—were significantly (p<.01) related to being in the high-treatment category (
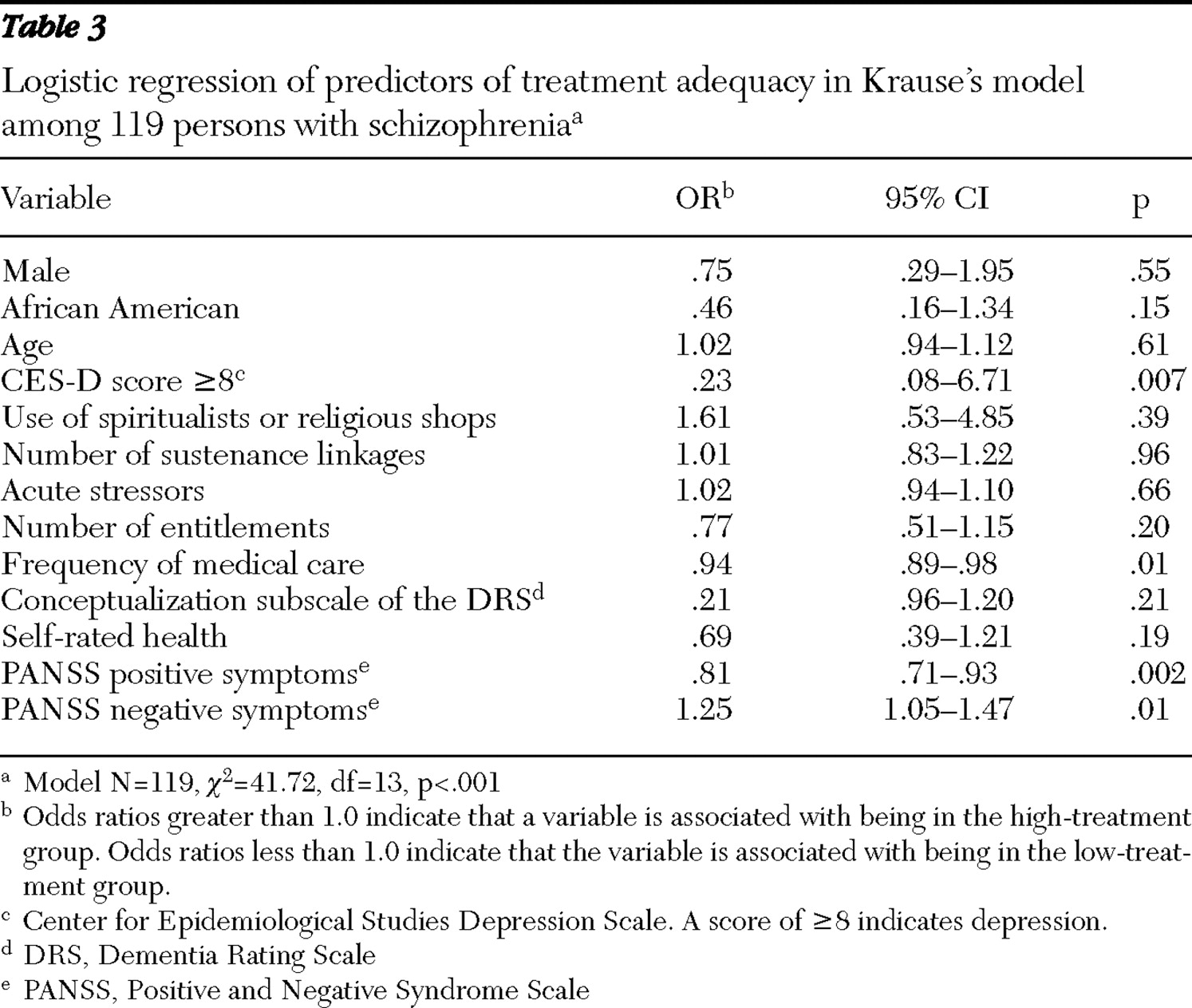
Table 2 ). When the 13-variable model was examined with logistic regression analysis, only clinical depression and lower levels of medical treatment retained statistical significance, and two additional variables emerged as being significantly associated with the high-treatment group: fewer positive symptoms and more negative symptoms (
Table 3 ). The overall model was statistically significant (
χ 2 =35.54, df=13, p=.001).
Discussion
To our knowledge this is the first study to examine factors associated with adequacy of medical treatment among older adults with schizophrenia. Because of the exploratory nature of this study, we began with the most elemental of assessments. That is, if people know that they have a medical condition, are they receiving medical treatment for it? To examine this question, we selected four conditions—diabetes, hypertension, heart disease, and gastrointestinal ulcers—that are sufficiently serious to almost always require medication. Of course, adequacy of treatment can also be assessed more stringently with physical examination and laboratory tests. Presumably, this type of analysis would have yielded substantially lower rates of treatment adequacy in both the schizophrenia and community comparison groups. However, given the findings of lower overall treatment levels among persons with schizophrenia, in particular for hypertension and heart disease, it would be practical to focus on ensuring that medication is being administered before undertaking more complex clinical assessments.
Even though our findings were similar to those of an earlier study (
27 ) that showed that persons with schizophrenia received inadequate medical care, our data indicated that this was not secondary to an inability to see a physician. The frequency of physician visits among the schizophrenia group was not different from a comparison group; 92% of the schizophrenia sample had seen a physician in the past year. The facts that patients with schizophrenia had rates of medical care equivalent to those of the comparison group and that persons with schizophrenia in the low-treatment group actually saw physicians more frequently than those in the high-treatment group suggests that the lower adequacy-of-treatment rate among patients with schizophrenia may be due to insufficient care rather than to poor accessibility.
Three clinical variables—positive and negative symptoms and depression—were significantly (p<.01) related to treatment in the schizophrenia group. The finding that positive symptoms were associated with being in the low-treatment category is consistent with reports in younger schizophrenia populations that physicians are often uncomfortable with patients with more flagrant symptoms of the disorder (
8 ), although our study did not provide data to demonstrate such discomfort. If this was indeed the case, it may lead to conducting inadequate physical examinations, taking poor histories, or misinterpreting physical symptoms as manifestations of psychoses (
8,
28 ). Moreover, positive symptoms have been thought to create impediments to care because of patients' difficulty in communication and their lack of insight regarding the condition and its treatment (
8 ).
On the other hand, somewhat surprisingly, we found that negative symptoms, which include symptoms of passivity, apathy, and lack of motivation, were associated with being in the high-treatment category. This is consistent with the observations by Felker and colleagues (
8 ) that passivity and concreteness are patient characteristics that may be valued by physicians.
Depression was also associated with being in the low-treatment group. In the literature, depression has been linked to increased service utilization (
29,
30 ). However, in our study, the fact that depression had an independent significant effect in logistic regression regardless of the number of visits to a physician meant that its impact on treatment adequacy was not related to service utilization. Because our data were cross-sectional, it is not clear whether persons with depression are less apt to communicate their symptoms to their physicians or whether failure to obtain treatment increases severity of medical illness and, consequently, produces more depressive symptoms. It is also plausible that this may be a bidirectional phenomenon.
The inverse association between fewer visits to a physician and being in the high-treatment group was a puzzling finding. We speculate that receiving more adequate treatment might result in a diminished need to see a physician. Another possibility is that it is related to factors that we did not measure; for example, some persons may be more adept at expressing their medical needs and more likely to obtain appropriate treatment. As noted above, this finding underscores how inadequate treatment is due not to inability to see physicians but to other factors.
Although Krause's model attained statistical significance, only four of the 13 variables in the model were significant. At a minimum this suggests that some of the model's components may need to be refined to accommodate aging populations with chronic mental illness. One variable that was significant in bivariate analysis—number of entitlements—was no longer significant in logistic regression, and three variables—number of visits to physicians and positive and negative symptoms—emerged as significant in the logistic regression analysis after having not attained significance in bivariate analysis. These findings probably reflect modest correlations of these variables with other variables in the model. We do not believe this finding reflects unstable parameter estimates because in bivariate and logistic analysis these variables were in the same direction.
This study has several strengths, including the fairly large size of the schizophrenia sample, a well-matched comparison group, an ethnically diverse urban sample, and the use of the multivariate analysis that allowed for the exploration of several variables in tandem. However, limitations were that the schizophrenia group was not randomly selected, the schizophrenia group was confined to a single geographical region, the data were cross-sectional, medical diagnosis and treatment were based on self-reports, medical conditions were not defined in detail, physical examinations or laboratory tests were not done, and illness severity was not measured. Finally, the variables measured in this study were largely about the patient, and to understand the interaction between health care and schizophrenia it will be necessary to include such variables as communication issues, access to care, and disease recognition from the provider and systems perspectives.
With respect to this study's clinical relevance, our findings suggest several potential patient variables that may affect treatment adequacy. For example, more aggressive identification and treatment of depression and positive symptoms of schizophrenia may be effective points of interventions. Perhaps health education approaches that teach persons to express their medical needs can be a useful adjunct. Moreover, physicians must focus more on the concept of treatment adequacy, in which the emphasis is placed not on frequency of visits but on receipt of appropriate treatment and measurable improvements in various parameters of disease. Finally, preliminary findings from Bartels and colleagues (
31 ) indicate that transforming the role of the traditional psychiatric case manager into a health care manager may enhance the quality of medical care of older adults with schizophrenia.
For several decades, the community mental health movement has concentrated on the psychiatric care and rehabilitation of persons with schizophrenia. It is a sad irony that although many individuals in this population have improved psychiatrically and functionally as they reach middle and older age, they often suffer from excess physical disability and mortality because of inadequate health care. Our medical system must give its highest priority to developing strategies for enhancing the health care of aging patients with schizophrenia.
Conclusions
Compared with their age peers in the general community, older adults with schizophrenia received less adequate medication treatment for four common medical conditions. Within the schizophrenia group, high treatment adequacy was associated with lower rates of depression, fewer positive symptoms, more negative symptoms, and fewer visits to medical care providers. The findings adumbrate several points for clinical interventions that may improve the adequacy of medical care among older persons with schizophrenia.
Acknowledgments and disclosures
This study was supported by grants SO6-GM-54650 and SO6-GM-74923 from the National Institute of General Medical Sciences.
The authors report no competing interests.