Survey instrument
The survey instrument was divided into four major sections assessing subjects' demographic characteristics and training, practice patterns, professional outlook, and experience with barriers to and resources for providing preventive services.
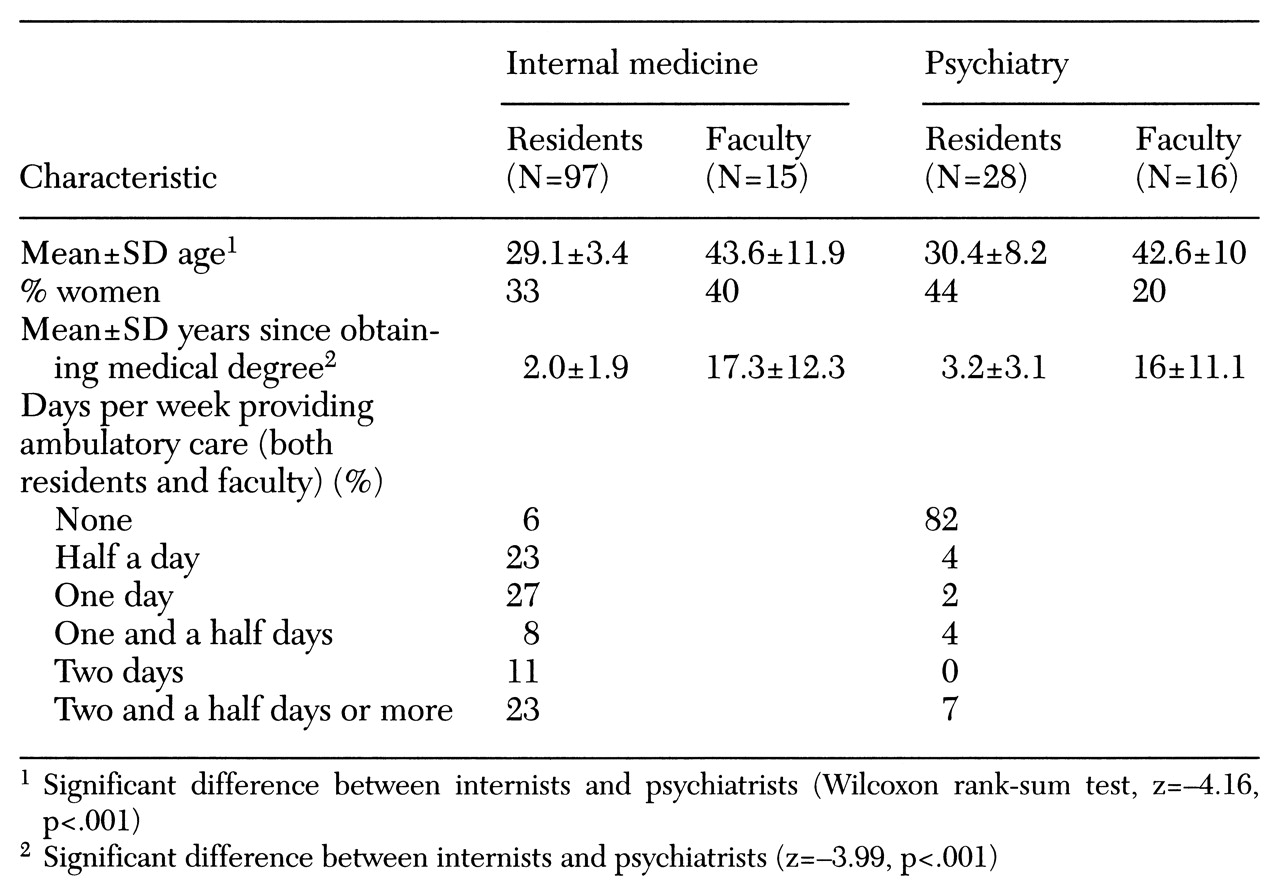
Demographic and training factors requested by the instrument included age, gender, number of years of practice or training, and year of medical school graduation.
Data requested on practice patterns included time spent in ambulatory and inpatient care and the frequency of asking about and providing advice about preventive services. These survey items were selected by a panel of four academic generalists, based on the U.S. Preventive Services Task Force guidelines and their relative importance in preventing morbidity and mortality.
Subjects were asked how often, during the past three months, they had asked about or assessed several areas associated with preventive services as part of the examination of or history taking with new patients. These areas were alcohol use, diet, exercise, immunization history, history of screening for colon cancer, use of seat belts, number of recent sexual partners, tobacco use, illicit drugs, use of female contraceptives, use of male contraceptives, history of Pap tests for women age 18 and older, history of mammograms for women age 50 and older, and exposure to ultraviolet light and use of sunscreens.
Frequency for these areas was ranked on a 7-point Likert-type scale on which the anchor points were never, or 0 percent of the time (scored 1); rarely, or between 1 and 20 percent of the time (scored 2); sometimes, or between 21 and 40 percent of the time (scored 3); about half the time, or between 41 and 60 percent of the time (scored 4); often, or between 61 and 80 percent of the time (scored 5); usually, or between 81 and 99 percent of the time (scored 6); and always, or 100 percent of the time (scored 7).
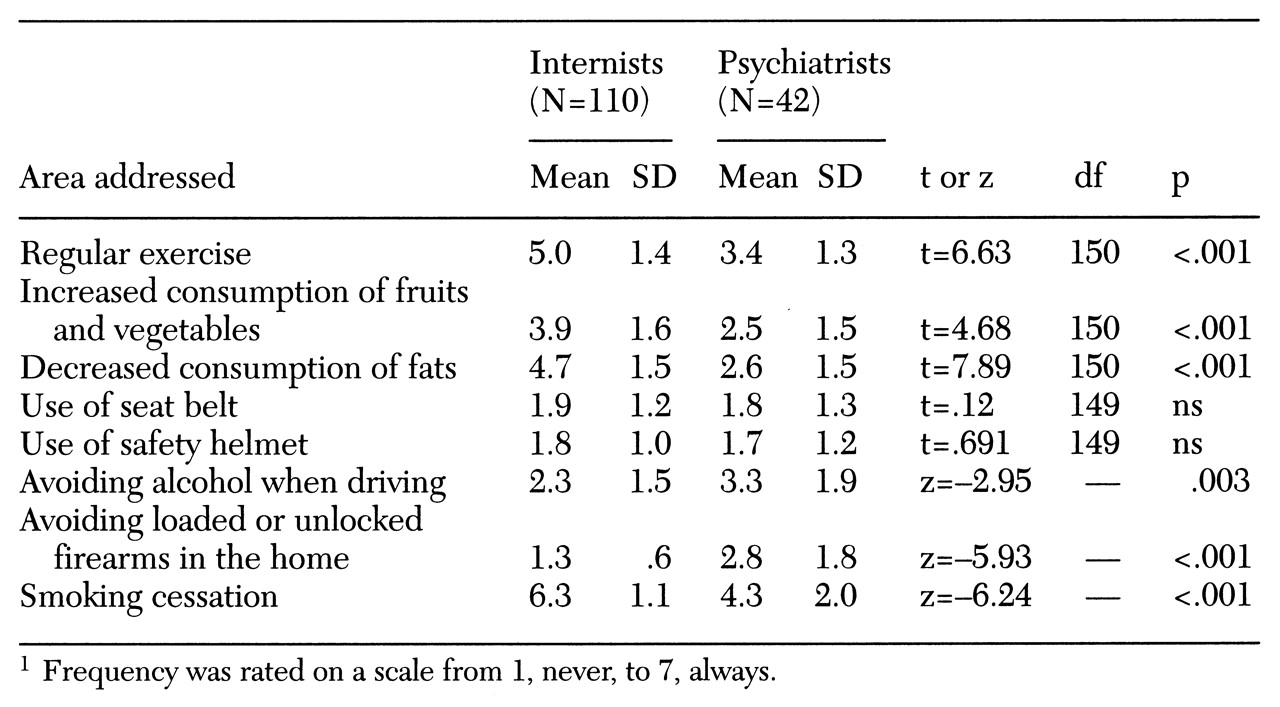
Respondents were next questioned about the frequency of advice delivered to patients. They were asked how often over the past three months, when they saw an adult patient in the clinic, they advised the patient about several health-related preventive measures, including exercising regularly, increasing consumption of fruits and vegetables, decreasing dietary fat consumption, always using a seat belt when operating or riding in a motor vehicle, wearing a safety helmet when operating or riding a motorcycle or bicycle, avoiding alcohol when driving, and avoiding loaded or unlocked firearms in the home. Answers were given on the same 7-point Likert-type scale.
Preventive counseling related to use of tobacco was assessed with a question that asked respondents how often over the last three months, when they saw a patient who smoked cigarettes, did they advise the patient to quit smoking, advise setting a specific "quit date," see or call the patient near the quit date, refer the patient to a group clinic or intensive smoking cessation program, prepare the patient for withdrawal symptoms, and prescribe a nicotine patch or gum. Responses were given on the same 7-point Likert-type scale.
The third section of the survey assessed respondents' attitudes toward preventive medical counseling by asking them to rate their own effectiveness in changing their patients' behavior in the areas of alcohol reduction, smoking cessation, exercise, safe sex practices, and diet. For each area, physicians were asked to assess whether they were minimally effective (scored 1), somewhat effective (scored 2), quite effective (scored 3), or extremely effective (scored 4). They were also given the option to respond "I never do this." This response was not scored.
Twenty questions depicting different clinical scenarios were used to assess overall knowledge about clinical preventive services. The 20 scenarios included questions such as the recommended frequency for a Pap smear and mammogram for a normal-risk 50-year-old woman and a normal-risk woman under age 35 and the recommended frequency of testing blood pressure and cholesterol and administering the graded-exercise cardiac stress test. Appropriate delivery of the pneumococcal pneumonia vaccine was also questioned. Knowledge scores were tabulated by summing the correct answers for a maximum score of 20.
The fourth section of the survey assessed the extent to which barriers such as lack of time, lack of allied health personnel, lack of prompts, lack of patients' interest, uncertainty about which preventive medical services to provide, and lack of educational materials prevented the physician from providing effective health promotion. The amount of medical education in clinical preventive medical services received in the last six months was categorized in terms of informal and formal hours ranging from none to greater than 12 hours.
The reliability and validity of the instrument were recently reported (
12). Copies of the survey instrument are available from the first author.