Depression is common, is costly, and has a significant impact on functioning and quality of life (
1,
2,
3). Effective treatments for depression exist, and national treatment guidelines for major depression have been developed (
4,
5,
6). Nevertheless, it is common for persons with depression to receive no treatment or to be undertreated (
3,
7,
8,
9,
10,
11), and the quality of depression care in the United States is low, with rates of adequate treatment ranging from 7 percent to 30 percent (
3,
7,
10,
12,
13).
African Americans, elderly persons, and Medicaid enrollees are particularly vulnerable to undertreatment of depression (
10,
14,
15,
16,
17,
18,
19). Depression treatment rates for African Americans have been found to be between one-half and one-third of those for Caucasians (
10,
20,
21,
22), and individuals who do receive treatment are substantially less likely to receive guideline-concordant care (
12). Studies show that elderly persons are much less likely to receive a diagnosis of depression, and as many as half to three-quarters of elderly persons receive no antidepressant treatment for their depressive symptoms; of those who do receive antidepressants, less than one-third receive adequate treatment (
10,
18,
23,
24). Elderly patients also have lower rates of use of psychotherapy than nonelderly patients (
22). Medicaid patients have been found to be less likely to receive selective serotonin reuptake inhibitors and less likely to receive psychotherapy, and they have lower rates of continuous therapy compared with patients who are privately insured (
16,
17).
Although recent studies have investigated quality of care for depression by age, race, and type of insurance, many studies have not clarified whether low rates of adequate care for subpopulations stem from low rates of initiation of treatment or from low quality of care once treatment has been initiated (
3,
7,
10). Knowing the answer to this question will help policy makers and clinicians design appropriate health policy and other interventions with the best chance of improving depression care.
The study reported here used nationally representative data to compare rates of initiation of depression treatment, and, among those receiving treatment, rates of adequate depression treatment by race or ethnicity, age, and type of insurance. Rates of adequate treatment for persons who used psychotherapy or counseling services and those who used antidepressants were assessed separately.
Methods
Data
We used data from the 2000 Medical Expenditure Panel Survey (MEPS), a nationally representative annual survey sponsored by the Agency for Healthcare Research and Quality (AHRQ). The MEPS uses an overlapping panel design that collects data for individuals over a two-year period through a baseline interview and five follow-up interviews and can be used for cross-sectional or longitudinal analysis (
25). The MEPS Household Component (HC) collects detailed information about health care use and expenditures, health status, and health insurance coverage as well as demographic information and is designed to produce annual estimates of these measures. The MEPS HC sample is drawn from a subsample of households included in the previous year's National Health Interview Survey. The 2000 MEPS HC data are from baseline and follow-up interviews with 25,096 individuals. The data in the MEPS 2000 HC are described in detail at www.meps.ahrq.gov.
Individuals with depression
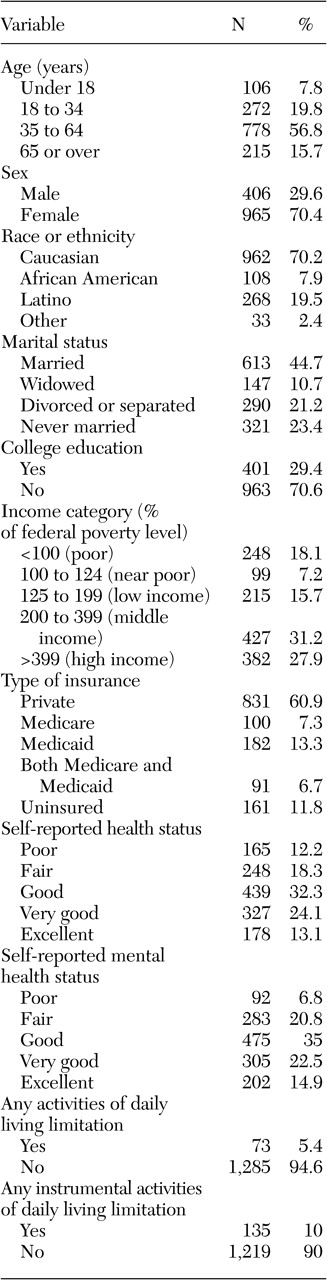
Individuals with depression were identified by using the MEPS HC medical conditions file. This file contains an observation for each self-reported medical condition that the individual experiences during the year. During each interview, respondents were asked about medical conditions they experienced during the four or five months since the previous interview. Thus all conditions are self-reported by respondents. Self-reported conditions were mapped onto three-digit ICD-9 codes by AHRQ. We classified conditions with ICD-9 codes of 296 or 311 as depression. Although the code 296 can also include bipolar disorder, more than 90 percent of individuals identified through these codes had a code of 311, corresponding to unspecified depression. In this study, the term "depression" is used to identify these individuals. On the basis of this method, 1,347 individuals were identified as having depression.
Antidepressant treatment
Antidepressant treatment was identified by using the prescribed medicines event file of the 2000 MEPS HC, which contains 182,677 prescribed medicine records. Each record represents one household-reported prescribed medicine purchased or obtained during 2000. Antidepressant medications were identified by drug name. The drugs classified as antidepressants were amitriptyline, amoxapine, bupropion, citalopram, clomipramine, desipramine, doxepin, fluoxetine, fluvoxamine, imipramine, isocarboxazid, maprotiline, mirtazapine, nefazodone, nortriptyline, paroxetine, phenelzine, protriptyline, sertraline, tranylcypromine, trazodone, trimipramine, and venlafaxine.
We calculated the daily dosage for each antidepressant prescription by using the pill dosage and the number of pills in the prescription. In our analysis, it was assumed that each antidepressant prescription was for a 30-day supply. After inspection of all prescription records by a psychiatrist (the second author), we decided to assume that if fewer than 30 pills were prescribed, the number of days supplied by the prescription equaled the number of pills supplied by the medication. Of the 8,944 prescriptions for antidepressants, 1,513 (17 percent) were for fewer than 30 pills. The daily dosages were then compared with the minimum adequate daily dosage developed by Weilburg and colleagues (
11) by using consensus of expert opinion and manufacturers' guidelines (
11). Because the purpose of this study was not to assess absolute rates of adequate treatment but to investigate differences in rates of treatment between groups, this method would not have introduced bias into the analysis if the differences in days supplied were distributed equally across groups.
Psychotherapy or mental health counseling visits
Psychotherapy or mental health counseling visits were identified by using the 2000 MEPS outpatient visit file (N=10,937) and the 2000 MEPS office-based medical provider visits file (N=99,939). These files contain one observation for each self-reported visit to a hospital-based outpatient clinic or office-based medical provider during 2000. For each visit, the respondent was asked which category best described the care provided during the visit. One possible category of response was "psychotherapy or mental health counseling."
Adequate depression care
Adequate depression treatment over a one-year period was defined as receipt of at least four antidepressant prescriptions at the minimum adequate daily dosage or at least eight outpatient or office-based psychotherapy or counseling visits. This definition was based on evidence-based treatment guidelines (
5,
26) and is similar to that used by Kessler and colleagues (
3) in their analysis of depression care that used data from the National Comorbidity Survey Replication.
Health and functional status
We adjusted for self-perceived health and mental health status and for functional limitations by using responses from the MEPS HC. Respondents rated overall health as excellent, very good, good, fair, or poor at three points during the calendar year. Respondents rated mental health by using the same categories. Respondents were also asked about functional limitations by using the Activities of Daily Living scale (
27) and the Instrumental Activities of Daily Living scale (
28). A dummy variable was coded 1 if the individual had at least one limitation on the Activities of Daily Living scale and was coded 0 otherwise. A dummy variable was coded in the same way for the Instrumental Activities of Daily Living scale. All health and functional status variables used measures collected during the first interview of the calendar year.
Sociodemographic measures
The analysis examined differences in adequate care by race or ethnicity, age, sex, insurance type, income, education, and marital status. Race or ethnicity consisted of four mutually exclusive groups: Caucasian, African American, Latino, and other. Any respondent who identified him- or herself as Latino was categorized as Latino, regardless of race. Age was coded as less than 18 years, 18 to 34 years, 35 to 64 years, and 65 years and over. Insurance type was categorized as any private insurance, Medicaid, Medicare, both Medicaid and Medicare, and uninsured. Income was measured as a percentage of the poverty level and was assigned to five categories: poor (less than 100 percent of the federal poverty level), near poor (100 to 124 percent), low income (125 to 199 percent), middle income (200 to 399 percent), and high income (more than 399 percent). Education was included as a dichotomous variable, coded 1 if the individual had a college education or above and coded 0 otherwise. Marital status was classified as married, widowed, divorced or separated, and never married.
Statistical analysis
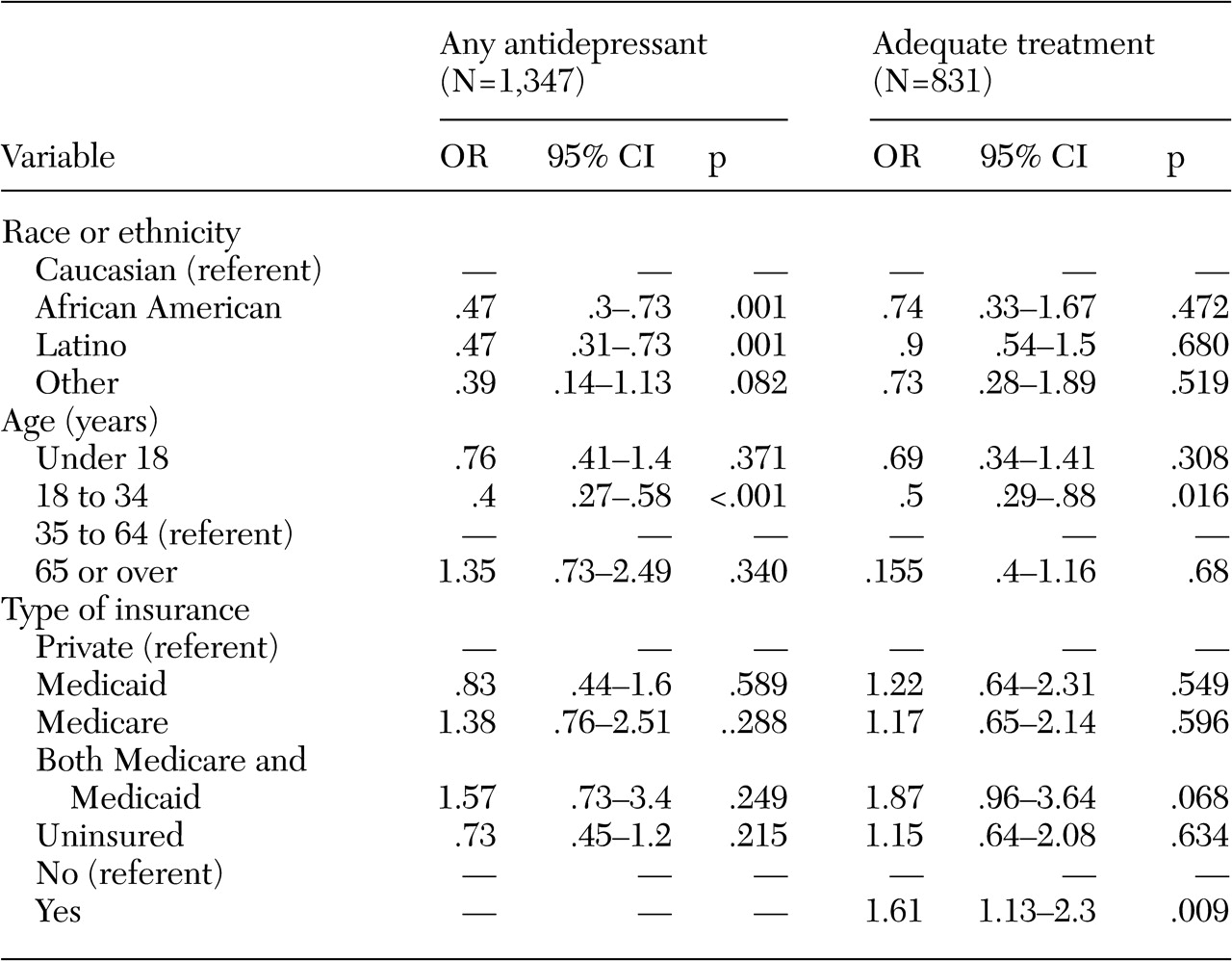
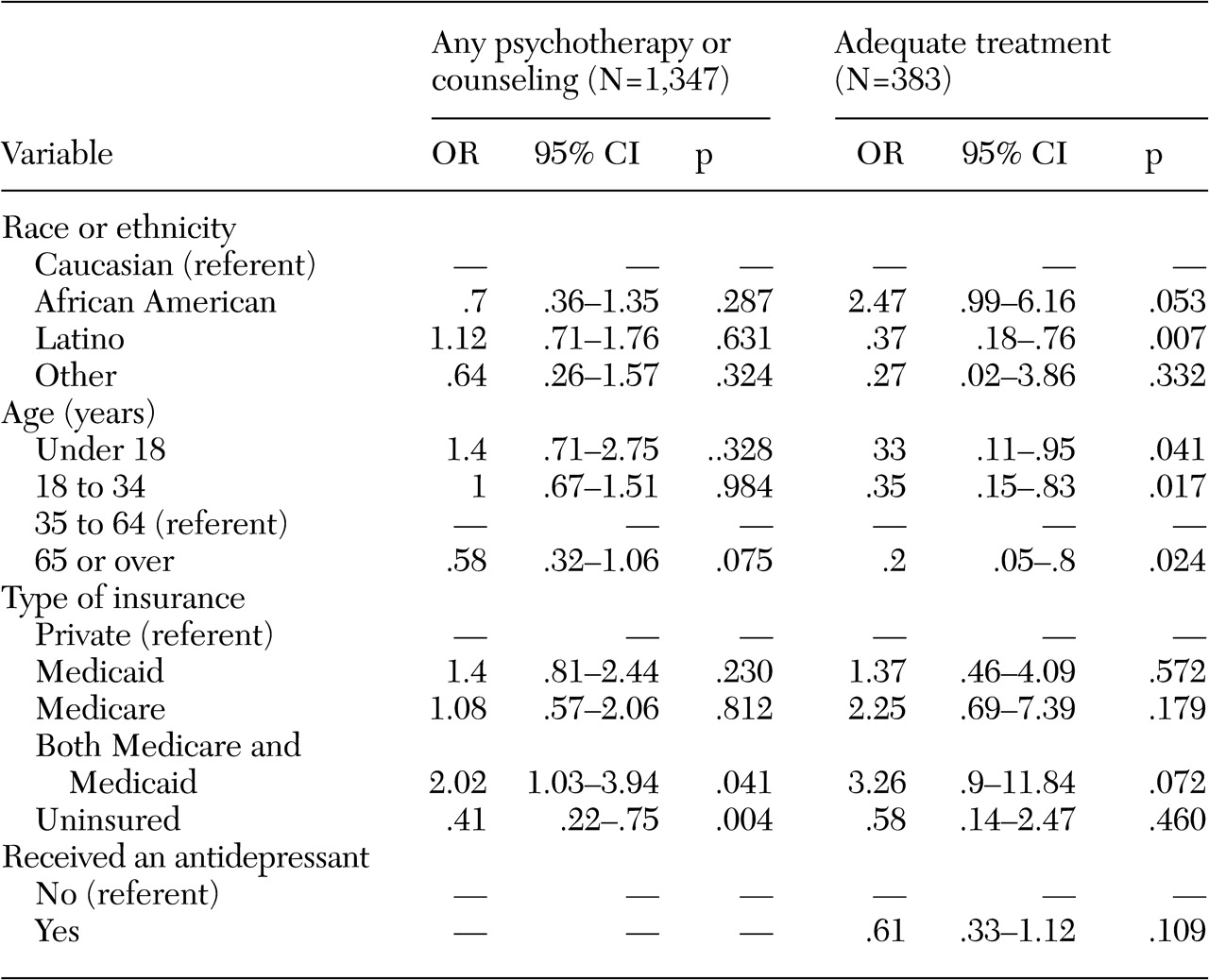
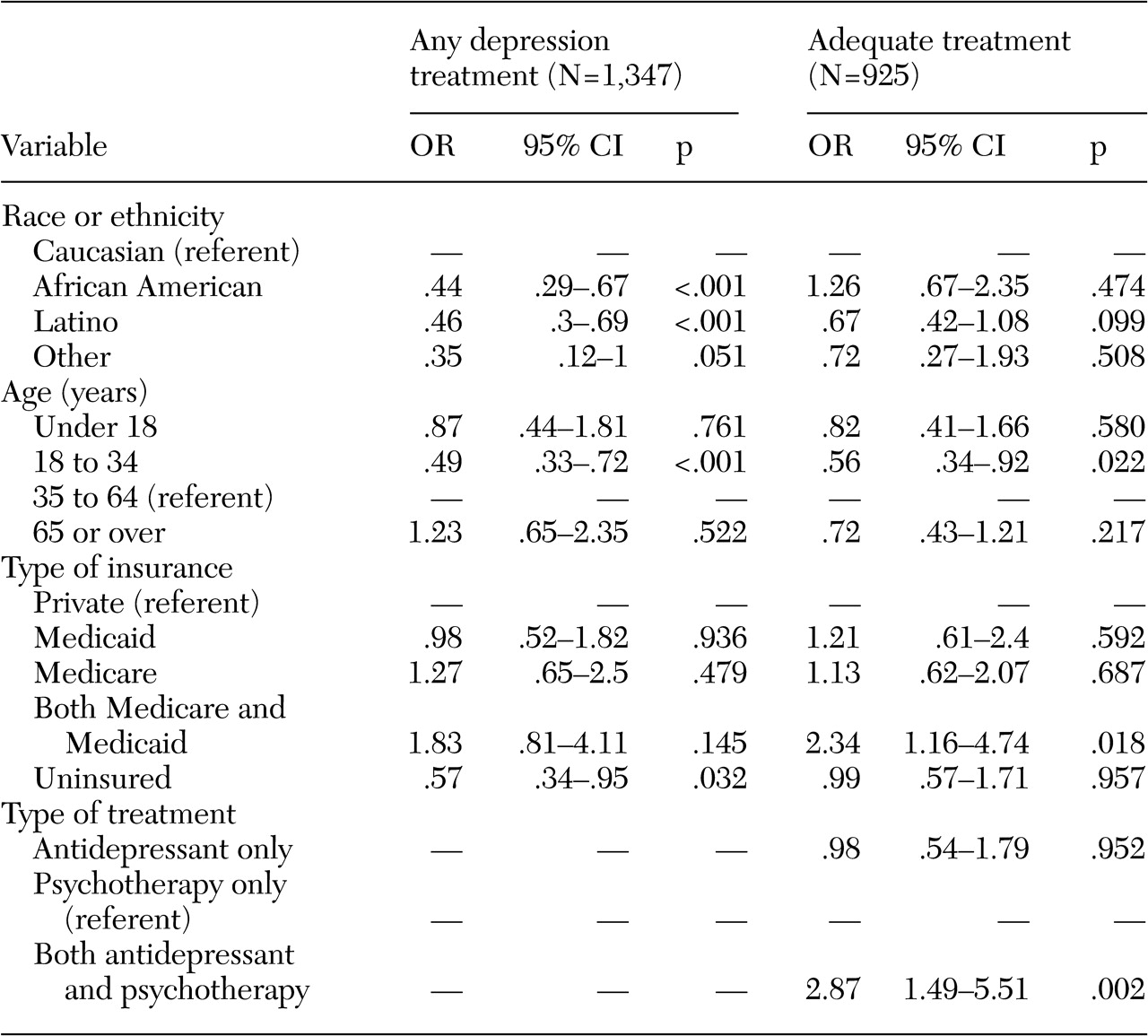
Logistic regression was used, because all dependent variables were dichotomous. The first regression examined receipt of at least one antidepressant prescription among persons with depression. The second regression examined the probability of receipt of an adequate course of antidepressants among persons with depression who had received at least one prescription for an antidepressant. The third regression assessed the probability of receipt of psychotherapy or mental health counseling among persons with depression. The fourth regression assessed the probability of receipt of an adequate course of psychotherapy among persons with depression who made at least one psychotherapy visit. To investigate whether persons who were receiving combination therapy were more likely to receive adequate treatment than those who were receiving antidepressants only or psychotherapy or counseling only, the two models that assessed whether adequate treatment was provided included independent variables indicating whether the person received both antidepressants and psychotherapy during the year. Finally, to help assess whether the type of treatment initiated (antidepressants or psychotherapy or counseling) was associated with higher rates of adequate care, a fifth regression examined the probability of receiving any form of adequate care given that the individual was depressed and used either antidepressants or psychotherapy or counseling at any point during the year, with indicator variables included in the model to indicate the type of treatment initiated. Models were estimated by using the survey procedures of Stata statistical software, using weights to account for the complex sampling strategy and to produce estimates that were nationally representative (
29).
Discussion
These results suggest that much of the disparities in depression care may be due to differences in rates of obtaining depression treatment, as has been found in previous studies (
10,
16,
17,
19,
21). It appears, for the most part, that once depression treatment is initiated, disparities in adequate care are not significant. Our study found that, among individuals who received psychotherapy or counseling, African Americans were more likely to receive an adequate course of treatment than Caucasians. Among individuals who received an antidepressant, no racial differences were observed in the probability of receiving adequate pharmacotherapy. Latinos were significantly less likely to receive any treatment and also significantly less likely to receive an adequate course of psychotherapy or counseling.
Young adults were the only age group consistently less likely to receive any treatment, less likely to fill an adequate number of prescriptions among antidepressant users, and less likely to receive an adequate number of counseling sessions. This finding may be due to the fact that young adults are less likely to use health services in general, although we did control for self-perceived health status. In contrast with previous studies, which have found that older persons use depression care less frequently than younger ones (
10,
15,
30), this study showed no significant differences in obtaining depression care among the elderly. Some of the differences in findings between this study and others may be due to differences in samples and sample selection criteria.
Unlike some previous studies that found that persons covered by Medicaid were less likely to receive depression treatment (
16,
17), our study showed no differences either in obtaining depression treatment or in the adequacy of depression care once care was initiated. It may be that the quality of depression care for individuals with Medicaid has improved, as found in more recent studies (
10,
31).
Persons who used both psychotherapy or counseling and antidepressant medications were significantly more likely to receive adequate depression care. This finding could be due to the fact that individuals who use both treatment modalities are more likely to be seen in mental health specialty care, where rates of appropriate treatment are higher and dropout rates are lower (
10,
12,
32). Persons who receive combination therapy may also have greater perceived need, and thus motivation, for services than those who use antidepressants only or psychotherapy or counseling only, although we did control for self-reported mental health status. Another possibility is that attending psychotherapy or counseling increases adherence to antidepressant medication regimens, increasing the probability of adequate antidepressant treatment. This last hypothesis is directly supported by our findings. However, this study provided no evidence that using antidepressants increases the probability of receiving an adequate course of psychotherapy or counseling.
Our results should be interpreted with several limitations in mind. First, identification of persons with depression was based on patient self-report. It is possible that some patients with depression were not identified as having depression and, similarly, some patients who were identified as having depression did not meet the diagnostic criteria for depression. It is also possible that reporting of depression varied by ethnic group, although a previous study showed no difference in the rate of reporting emotional problems to medical providers by ethnic group (
33). However, if African Americans and Latinos underreported depression, the estimates of relative rates of receipt of any treatment would be conservative, because persons from ethnic minority groups who self-reported depression would have had higher severity levels than Caucasians. Underreporting by these groups would be less likely to affect estimates of adequate treatment for persons who received treatment because all individuals in this subsample were judged by a clinician to have depression severe enough to warrant treatment. Also, because the analysis included all individuals with an
ICD-9 code of 296, some individuals with bipolar disorder were included in the analysis.
Another limitation is that the type or duration of individual psychotherapy or mental health counseling sessions was not known. In addition, the date that antidepressant medication prescriptions were filled and the number of days of medication supplied were not known. Because only treatments that were provided during the calendar year were assessed, our data might be subject to left or right censoring—that is, some individuals may have initiated a treatment regimen before the beginning of the calendar year or may have continued treatment after the end of the calendar year; for these patients, it is possible that not all prescriptions or psychotherapy or counseling were included in our data. Left censoring has also been an issue in past studies that have examined care in the previous 12 months (
7,
10). Also, use of depression treatment was based on self-report, which introduces the possibility of recall bias. However, because we were interested primarily in differences in adequacy of treatment among different sociodemographic groups, not the actual prevalence of adequate treatment, as long as the measurement errors were distributed randomly among respondents, these limitations should not affect the findings.