Anxiety disorders such as panic disorder and panic disorder with agoraphobia are common psychiatric illnesses. As the Epidemiologic Catchment Area data show (
1), the lifetime prevalence rate for panic disorder in women is double that for men (2% versus 1%), and the rate for panic disorder with concurrent agora~phobia is even more disproportionate: 7.9% for women compared with 3.7% for men. Data from the National Comorbidity Survey (
2) also demonstrate that the lifetime prevalence of DSM-III-R panic disorder for women (5%) is more than twice that for men (2%), but the 2:1 sex ratio is retained for panic disorder with agoraphobia in the National Comorbidity Survey and in other community studies (
3,
4).
Aside from the variation in prevalence rates, only a few significant differences between men and women with either panic disorder or panic disorder with agoraphobia have been shown (
5,
6). Some studies have found that women who have panic disorder with agoraphobia endorse slightly greater fear (
7,
8), although other studies have found that men are more fearful, particularly regarding somatic concerns (
9). A more consistent finding is the higher rate of alcoholism in men than in women suffering from panic disorder with agoraphobia (
10–
12). Finally, there is some suggestion that the clinical course and outcome of anxiety disorders, including panic disorder with agoraphobia and panic disorder, differ between men and women. In one naturalistic study of anxiety neurosis (defined according to the Feighner criteria [13]), women had more symptoms and higher medical care utilization at 4-year follow-up (
14). A second observational study found that female sex predicted greater avoidance and panic after 1 year (
15). No sex differences were found in a third study that reinterviewed subjects an average of 3 years after their participation in a treatment study (
16).
While cross-sectional studies can address a number of questions, they are limited in their evaluation of clinical course. Using a prospective design and short-interval follow-up interviews, our group has shown that panic disorder and panic disorder with agoraphobia are chronic, recurring illnesses. We found 1-year remission rates of 37% for panic disorder and 17% for panic disorder with agoraphobia (
17), but among the patients who attained remission, relapse was common. This illustrates the potential for varying results in outcome evaluations if a single cross-sectional point is designated. This may also bear on the question of prevalence rates, since longer cumulative symptomatic periods, due to either lower remission rates or a higher likelihood of symptom recurrence, would increase apparent prevalence estimates. Given the mixed reports on differences between the sexes in clinical course, we used prospectively collected data to test whether women would experience lower remission rates or greater relapse into symptoms compared with their male counterparts. We also used these data to explore possible sex differences in demographic characteristics and comorbidity. Since previous studies have failed to find substantial differences between the sexes in demographic characteristics or age at onset, we hypothesized that there would be few differences in our study group. We did hypothesize that our study group, similar to others, would show more comorbid alcohol abuse in men but higher rates of co-occurring agoraphobia in women.
METHOD
This report is based on data from the Harvard/Brown Anxiety Disorders Research Program. The methods used in the program have been described in detail elsewhere (
17). The Harvard/Brown Anxiety Disorders Research Program is a prospective, naturalistic longitudinal study of patients with DSM-III-R-defined anxiety disorders. Entrance criteria for the study include at least one of the following DSM-III-R current or past diagnoses: panic disorder, panic disorder with agoraphobia, agoraphobia without panic disorder, generalized anxiety disorder, and social phobia. Subjects were at least 18 years of age and provided written informed consent. The exclusion criteria were organic mental disorder, schizophrenia, or psychosis within the last 6 months. Seven hundred eleven patients were recruited from private practices and teaching clinics of the psychiatry departments at Harvard Medical School, the University of Massachusetts, and Brown University. Five hundred twenty-seven subjects had a lifetime history of panic disorder or panic disorder with agoraphobia; 412 were in an episode of panic disorder or panic disorder with agoraphobia at intake and had at least one follow-up evaluation. Since data on course of panic were available only for the latter group, this set was used for the analysis in this report.
The initial comprehensive evaluation of subjects included selected items from the Personal History of Depressive Disorders (
18), the Structured Clinical Interview for DSM-III-R—Patient Version (SCID-P) (
19) (nonaffective disorders section), and the Schedule for Affective Disorders and Schizophrenia—Lifetime Version (SADS-L) (
20). Items from the SCID-P and SADS-L were combined to create the SCALUP (
21).
Follow-up was conducted at 6-month intervals for the first 2 years and annually after that point. The Longitudinal Interval Follow-up Evaluation (
22) was used to collect information on severity of symptoms and medication treatment.
All intake interviews were conducted in person or by telephone by experienced clinical interviewers who underwent an initial 3- to 6-month training period. Ongoing monitoring for interrater reliability included review and comparison of raw data, with an interview summary and one videotaped interview per month. The latter was rated independently by other monitors, who also met to discuss ratings. Three substudies to assess interrater reliability, subject recall, and validity of the Longitudinal Interval Follow-up Evaluation psychiatric status ratings were conducted with subjects already enrolled in the Harvard/Brown Anxiety Disorders Research Program (
23). Median intraclass correlations (ICC) for psychiatric status ratings according to disorder were the following: for panic, 0.72 (range=0.62–0.88); for agoraphobia, 0.81 (range=0.49–0.98); for social phobia, 0.87 (range=0.75–0.89); for major depressive disorder, 0.80 (range=0.73–0.93); and for Global Assessment Scale (GAS) score, 0.75 (range=0.72–0.77). The long-term test-retest reliability of subjects' retrospective recall over a 1-year period was found to be acceptable for panic (ICC range=0.62–0.80) and very good to excellent for all other index disorders and for major depressive disorder (ICC range=0.89–1.00). An independent external validity assessment comparing summed psychiatric status ratings with GAS scores found a significant inverse correlation of 0.57 (N=550, p=0.0001) (higher GAS scores reflect higher functioning, while higher psychiatric status rating scores are indicative of greater impairment).
Psychiatric Status Ratings
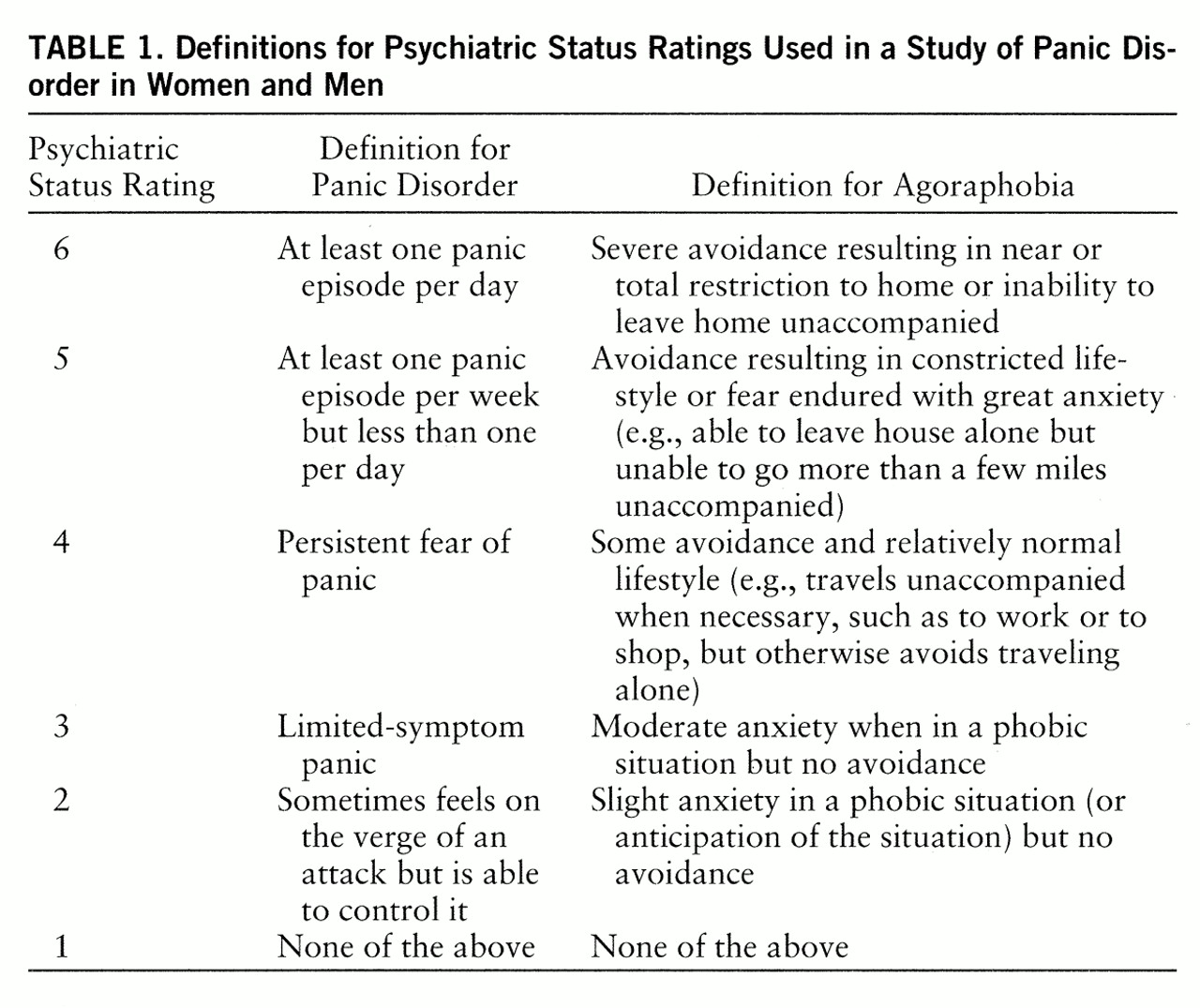
At each interview, individuals were assigned a psychiatric status rating ranging from 1 to 6 (
table 1) that corresponded to the number and frequency of symptoms and the degree of functional impairment experienced during each week of the study. Subjects were assigned a psychiatric status rating for panic and for agoraphobia if they experienced both. For this report, a subject's status for each given week was assessed by taking the higher of the two ratings for panic and agoraphobia; for example, if a subject's psychiatric status rating for panic was 5 and for agoraphobia was 4, the combined psychiatric status rating was 5. This gives a measure of whether the subject met the full DSM-III-R criteria (was in an episode), was asymptomatic (in remission), or was somewhere in-between (met partial criteria). To investigate possible differences missed by this simplification, panic psychiatric status ratings for the panic and agoraphobia groups were also compared separately.
Definitions of Remission and Relapse
A full discussion of the remission criteria has been previously published (
17). A sustained period of improvement for at least 8 weeks was required for a rating of remission. Symptom levels for remission were defined as no more than minimal symptoms of panic (no attacks, although sometimes the subject feels on the verge of an attack) or of agoraphobia (no more than slight anxiety in a situation and no avoidance). These levels correspond to psychiatric status ratings of 1 or 2.
We used two definitions in examining the likelihood that subjects in remission would return to meeting the full DSM-III-R criteria. A less stringent definition was first explored to ensure that substantial recurrence of symptoms was not missed. This definition required experiencing one or more panic attacks (psychiatric status rating ≥5 for panic) or severe agoraphobia (psychiatric status rating ≥5 for agoraphobia) for at least 1 week. The more rigorous definition used the same psychiatric status rating of at least ≥5 but required this rating for a minimum of 4 out of 8 weeks.
Treatment
Treatment in the Harvard/Brown Anxiety Disorders Research Program was not controlled but was recorded at each interval. In a previous report (
24), we analyzed pharmacological treatment received 6 months after intake. We used the literature to identify efficacious psychopharmacological treatments for panic disorder and panic disorder with agoraphobia. These treatments were rated according to the strength of evidence (i.e., placebo-controlled randomized clinical trials, open trials, case studies). Optimal dosage ranges were similarly rated. Subjects were assigned a level of antipanic therapy based on this analysis (see reference 24 for greater detail on methodology).
Statistical Analysis
All statistical analyses were conducted with SAS Version 6.07 (
25) with the use of PROC TEST and PROC FREQ. Longitudinal data were analyzed with standard survival analysis techniques (
26). The log rank test was used to compare distributions at several times for dichotomous variables. We tested for predictors of time to remission and time to improvement in symptoms by using Cox regression.
RESULTS
Only patients in an episode of panic disorder with or without agoraphobia at the time of intake to the Harvard/Brown Anxiety Disorders Research Program were examined. This resulted in a study group of 412 subjects out of the entire group of 711 patients in the program; the remaining patients either never had panic disorder or panic disorder with agoraphobia or were not in an episode of illness at intake. Of the 412 subjects in this report, 76 (18%) had panic disorder and 336 (82%) had panic disorder with agoraphobia at the time of intake. Forty-two (55%) of the patients with panic disorder were women, and 238 (71%) of those with panic disorder with agoraphobia were women. Although all 412 subjects had met the full DSM-III-R criteria for panic disorder at some point during their episode before intake, 29 (7%) of them met only partial criteria at intake. Severity of both panic and agoraphobia was assessed at intake with the DSM-III-R modifiers mild, moderate, and severe. The men and women did not differ in the severity of either panic or agoraphobia at intake.
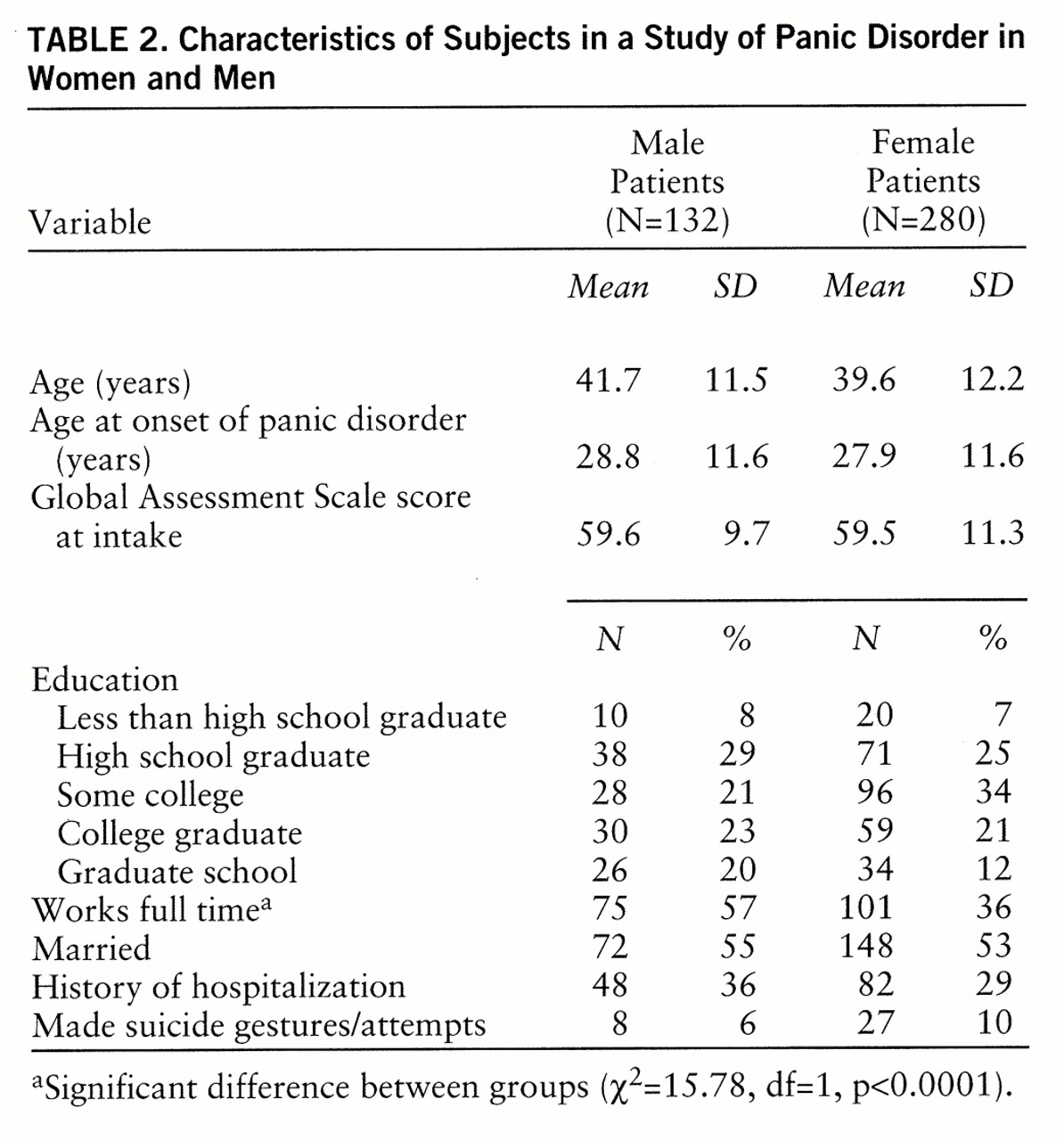
There were no significant differences between the men and women in education, marital status, age at onset of panic, or duration of the intake episode of panic (
table 2). There was, however, a difference between the men and women in full-time work status.
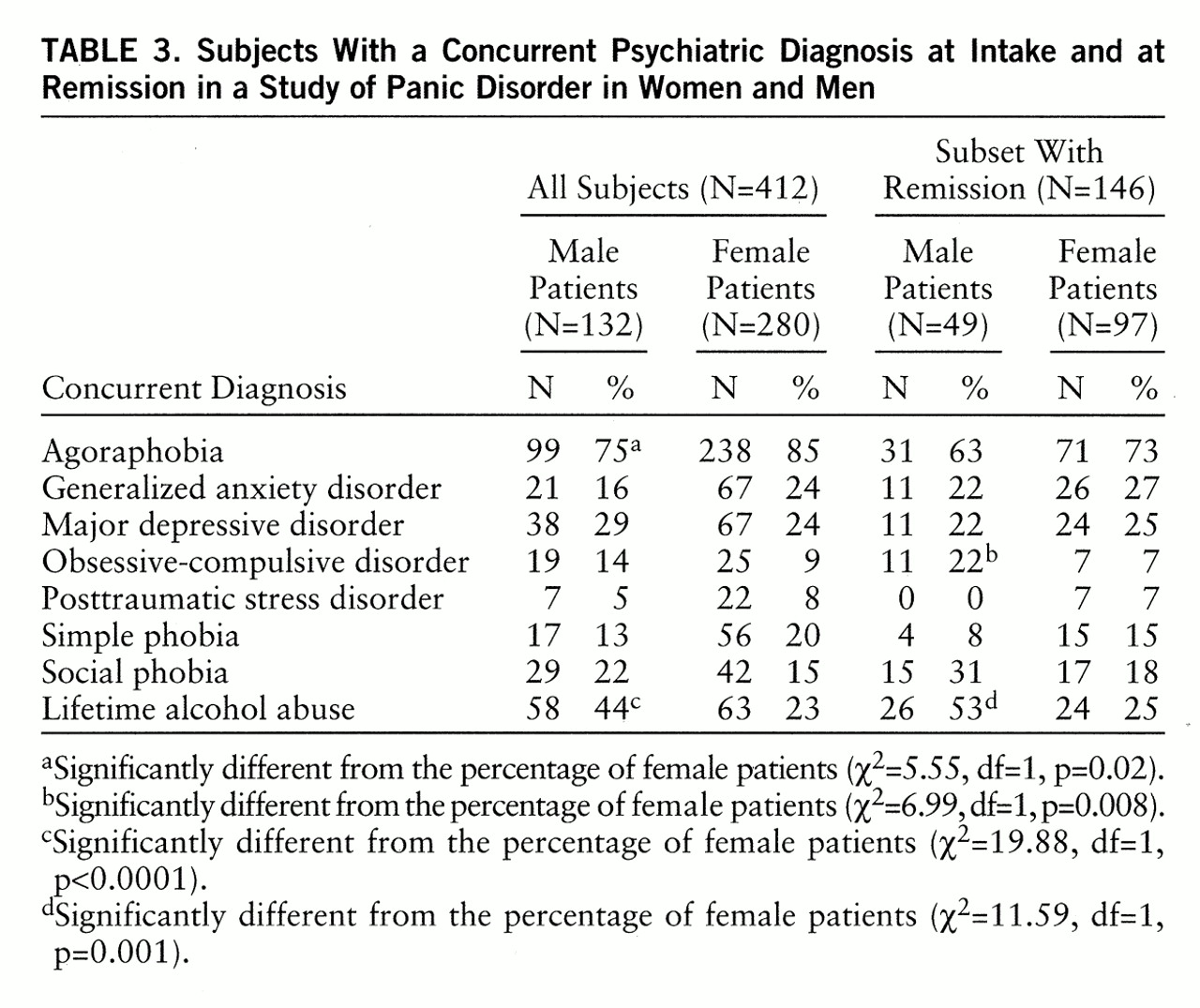
Comorbidity was operationally defined as active co-occurring disorders. The percentages of men and women with various concurrent diagnoses at intake and after remission are shown in
table 3. Among subjects in an episode at intake, women were more likely than men to have concurrent agoraphobia (85% versus 75%). Among subjects who experienced remission, the difference in rates of concurrent agoraphobia between men and women was not statistically significant. A past history of alcohol abuse/dependence was more common among the men both at intake (44% versus 23%) and after remission (53% versus 25%). Obsessive-compulsive disorder occurred significantly more often in men after remission (22% versus 7%).
There were no statistically significant differences between men and women in the percentages receiving psychosocial treatment. Among the 398 patients for whom psychosocial treatment information was available, 290 (73%) reported receiving psychosocial treatment in addition to medications. Psychotherapeutic techniques that were used included behavioral therapy (16%), relaxation/meditation treatment (13%), cognitive therapy (18%), and psychodynamic psychotherapy (37%).
Eighty-four percent of both men and women received psychoactive medication. Men and women had virtually identical rates of treatment with benzodiazepine anxiolytics (68%), tricyclic antidepressants (26%), mon~amine oxidase inhibitors (4%), and serotonin reuptake inhibitors (17%). There were no differences between men and women in the intensity of treatment received, as measured by antipanic therapy levels. Similarly, men and women did not differ in the number of weeks of medication use.
Remission
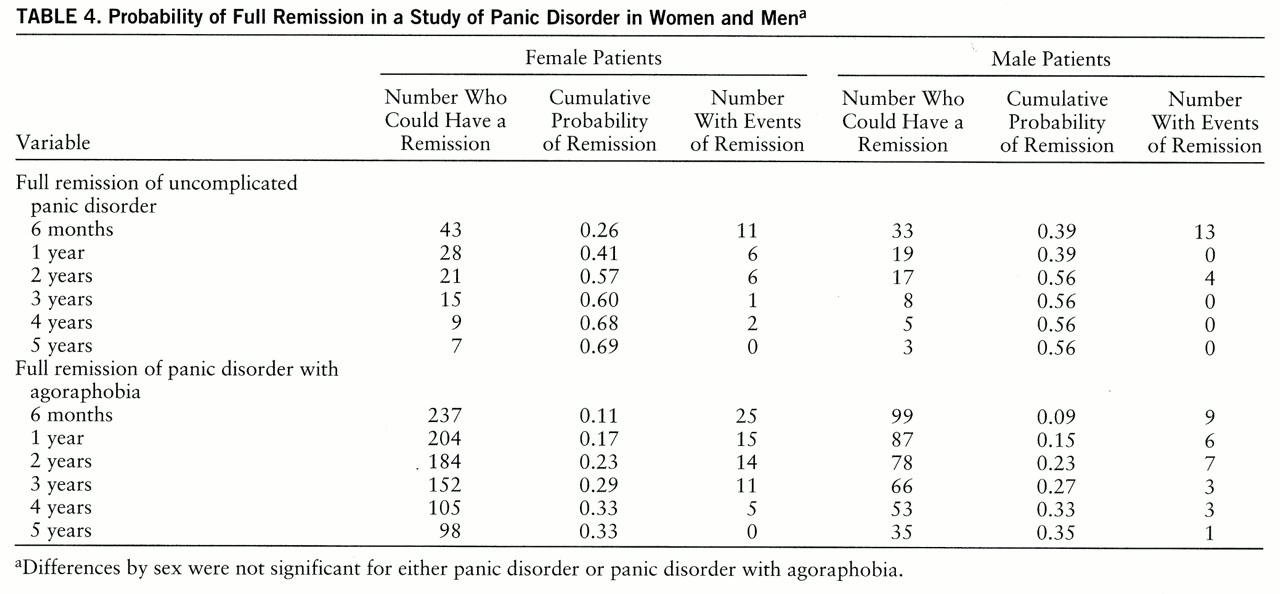
During the 5 years of follow-up, for both men and women, the probability of remission of panic disorder with or without agoraphobia was 0.39. At 5 years the remission rate for women with panic disorder or panic disorder with agoraphobia was 0.38, while for men it was 0.41, a difference that was not significant. As noted previously (
17), patients with panic and agoraphobia were less likely to have a remission than patients with uncomplicated panic. This is illustrated in
table 4, which presents results for men and women with either panic disorder or panic disorder with agoraphobia. There were no additional remissions for male patients with panic disorder after 3 years, which may be because of the very small number (N=8) eligible for remission. The number of women available for remission was higher (N=15), but still small. On the other hand, after 3 years the number of women in an episode of panic disorder with agoraphobia and thus eligible for remission was much higher than the number in the panic disorder group, but the rates of remission at 5 years remained nearly identical for men (0.35) and women (0.33) (
table 4).
Symptom Recurrence
Applying the 1 week of symptom recurrence definition, we found that over one-half (N=78) of the 146 subjects with either panic disorder or panic disorder with agoraphobia who achieved remission had a return of panic attacks or met the full criteria for panic disorder with agoraphobia during the 3-year period after their remission. In evaluating the risk of panic disorder independent of panic disorder with agoraphobia, we found that at 3 years the cumulative probability of symptom recurrence was 0.65 for women with panic disorder, while it was 0.39 for men. For panic disorder with agoraphobia, the cumulative probability of symptom recurrence at 3 years was 0.75 for women and 0.47 for men.
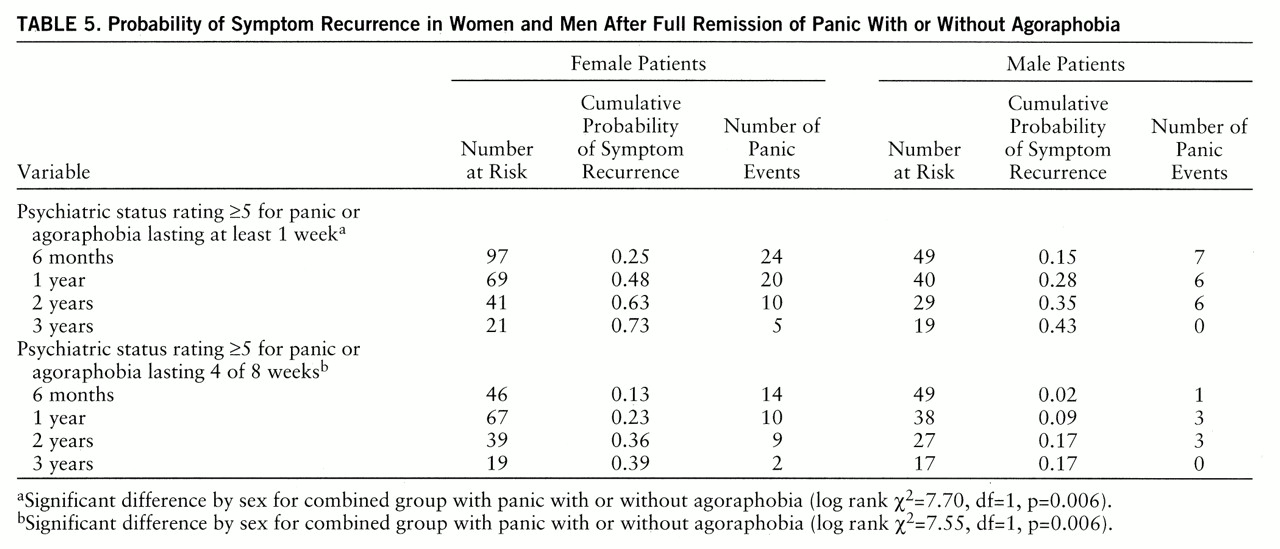
Since there was no significant difference in symptom recurrence for panic disorder or panic disorder with agoraphobia, these groups were combined (
table 5). The combined risk at 3 years was 0.73 for women and 0.43 for men. Of the subjects who experienced symptoms for at least 1 week, 28% of the women (95% confidence interval=18%–40%) and 36% of the men (95% confidence interval=18%–57%) had symptoms for 1 week only. This difference between men and women was not statistically significant, illustrating enduring symptom recurrence in both groups. Applying the more rigorous definition, a psychiatric status rating of 5 or more for at least 4 of 8 weeks, we found that symptom recurrence continued to be significantly higher in the women. When severity of panic symptoms and history of alcohol abuse or dependence were included in the statistical model (Cox regression), women were still more likely to reexperience panic or agoraphobic symptoms.
In the analysis of symptoms most likely to recur, panic attacks and not agoraphobic fear were almost invariably the trigger for clinical worsening in both the group with panic disorder and the group with panic disorder with agoraphobia, as noted in an earlier article (
17).
DISCUSSION
Results from this analysis support several prior cross-sectional follow-up studies which suggested that men and women with panic disorder and panic disorder with agoraphobia have a different course of illness. Our data show that the rate of recurrence of symptoms for women was nearly double the rate for men, and this held for subjects who had either panic disorder or panic disorder with agoraphobia. By 6 months, panic or agoraphobic symptoms had returned in 15% of the combined groups of men with panic disorder and panic disorder with agoraphobia and in 25% of the women with either panic disorder or panic disorder with agoraphobia. This difference in rates continued throughout the 3-year period after remission, so that 59 (61%) of 97 women and 20 (41%) of 49 men experienced symptom recurrence by 3 years. The higher rate of symptom recurrence in women held true even after alcohol abuse and concurrent agoraphobia were considered in the statistical model. As in an earlier analysis, subjects were more likely to reexperience symptoms of panic than of agoraphobia. This is consistent with the work of others, which found that compared with male patients, female patients experienced significantly more panic attacks during the interval before reevaluation (
14,
15). It also supports some treatment research (
27), but not all (
28), showing that behavioral therapy leaves women with more symptoms of panic attacks than men.
Given the greater risk of relapse for women after becoming well, it is likely that follow-up conducted after several years would find more women with symptoms. Thus, our current results are also consonant with follow-up studies conducted with groups of subjects with anxiety disorders (
14,
15). Those studies reevaluated patients between 3 and 4 years after the initial presentation, a time period that is ample for both remission and relapse. A worse outcome for women was not found in a third study by Noyes and colleagues (
16), who reinterviewed study participants an average of 3 years after the index protocol.
A previous report by our group (
17) showed that length of episode (i.e., time to remission) is longer for patients who have agoraphobia in conjunction with panic. Our hypothesis that remission in women would take longer was not substantiated, most likely because it was the presence of agoraphobia, rather than female sex, that most influenced remission (
17). However, women in community and clinical populations are more likely to suffer from panic disorder with agoraphobia, which has a slower time to remission than panic disorder. Thus, if concurrent agoraphobia is not controlled for in the outcome analysis, the remission rate appears to be worse for women.
While a difference in relapse rates may contribute to the higher prevalence rates for panic in women, it is not totally explanatory. Rather, there may be unique biological and psychosocial precipitants that lead to increased vulnerability to panic disorder and panic disorder with agoraphobia in women. Klein (
29) suggested that the last days of the menstrual cycle are associated with a decline in hyperventilation and an increased propensity to trigger a “false suffocation” alarm and, ultimately, panic. Yonkers (
30) has suggested that decreases in endogenous anxiolytics, such as progesterone metabolites, during the end of the premenstrual phase and in the follicular phase increase vulnerability to panic. A possible protective effect of progesterone has been empirically tested by one group (
31), who found that women were less likely to develop provoked panic when levels of progesterone and its metabolites were high.
In addition to biological explanations, psychosocial factors should not be ruled out. As noted in previous reviews (
5,
30), women are more likely to be harm-avoidant and are less likely to expose themselves to fear-inducing situations (
32). This may decrease the likelihood of therapeutic “autoexposure” after an initial fear has developed.
Although the data presented here do not address the issue, it appears that there are differences between the sexes in the course of at least one other anxiety disorder. Breslau and colleagues found that not only are women more likely to develop posttraumatic stress disorder (PTSD) (
33), but they are more likely to develop a chronic form of the illness (
34). Perhaps related processes are driving the high risk of chronicity when these illnesses occur in women.
In the current study, the demographic characteristics of the male and female subjects were similar. The only significant difference was that the men were more likely to have been employed full time, a characteristic true of the general population. The comorbidity findings in the Harvard/Brown Anxiety Disorders Research Program were similar to those reported by others, in that alcohol abuse was seen more commonly in men (
10,
12). Hallam (
11) suggested that men with phobias cope with their symptoms by drinking rather than staying home. This was supported somewhat by the finding of Cox and colleagues (
10) that men were more likely than women to view use of alcohol as an effective strategy for coping with anxiety. Despite these theories, alcohol abuse histories in our study did not influence course of illness.
This study had some strengths and weaknesses that differentiate it from previous work in this area. First, the study group was composed of patients recruited from psychiatric centers. Thus, these findings may differ from those that would be found in community samples, which may include persons with less severe illness or may include housebound persons with agoraphobia who are not in treatment. Second, the study was observational in nature rather than controlled, so the findings could have been caused by differences in the treatment received by the men and women. This is unlikely, however, because the men and women were equally likely to receive either psychotherapy or pharmacother~apy, and the latter was provided at the same intensity level for each sex.
The strengths of this study include the careful individual evaluation with use of DSM-III-R criteria, the use of standardized instruments, and the fact that a naturalistic study group was used. In addition, we used a prospective, longitudinal follow-up conducted on multiple occasions after a moderately short period of time (6 months for the first 2 years and then annually), lessening the bias that can be found when events are retrospectively reported. Further, standardized definitions of remission and symptom recurrence were imposed on these longitudinal data, which allowed us to clarify both. This is especially important in the evaluation of the course of illnesses that are chronic and relapsing.
CONCLUSIONS
Data from this longitudinal study of panic disorder and panic disorder with agoraphobia show that women and men are equally likely to have remissions of panic disorder, but women are more likely to reexperience symptoms after gaining remission. Differences in course of illness occurred after control for lifetime alcohol abuse or the presence of agoraphobia. Our findings for panic disorder and panic disorder with agoraphobia parallel findings for PTSD, which is also more chronic in women. It is unclear what types of biological and psychosocial substrates are contributing to the more chronic course of illness for women with these anxiety disorders, but further research into differences between the sexes may shed light on etiological factors.
ACKNOWLEDGMENTS
The Harvard/Brown Anxiety Disorders Research Program is conducted with the participation of the following investigators: P. Alexander, M.D., A. Gordon, M.D., M.B. Keller, M.D. (Chairperson), S. Rasmussen, M.D., R. Stout, Ph.D. (Butler Hospital–Brown University School of Medicine); M.G. Warshaw, M.S.S. (Brown University School of Medicine); T. Shea, Ph.D. (Veterans Administration Hospital, Providence–Brown University School of Medicine); E. Fier~man, M.D., F. Rodriguez-Villa, M.D. (Cambridge Hospital–Harvard Medical School); M.P. Rogers, M.D. (Brigham and Women's Hospital–Harvard Medical School); J. Cole, M.D., G. Mallya, M.D. (Mc~Lean Hospital–Harvard Medical School); R.M. Goisman, M.D. (Massachusetts Mental Health Center–Harvard Medical School); N. Weinshenker, M.D., R. Vasile, M.D. (Beth Israel/New England Deaconess Hospital–Harvard Medical School); J. Ellison, M.D. (Harvard Community Health Plan and the Cambridge Hospital–Harvard Medical School); A. Massion, M.D. (University of Massachusetts Medical School); G. Steketee, Ph.D. (Boston University School of Social Work); K.A. Yonkers, M.D. (University of Texas Southwestern Medical Center). Additional contributions from J. Curran, M.D., I. Goldenberg, Psy.D., R. Hirschfeld, Ph.D. (University of Texas, Galveston); J. Hooley, D. Phil. (Harvard University); P. Lavori, Ph.D. (Stanford University); J. Perry, M.D. (Jewish General Hospital–McGill School of Medicine); L. Peterson (Veterans Administration Hospital, Togus, Maine); J. Reich, M.D., J. Rice, Ph.D. (Renard Hospital–Washington University School of Medicine); H. Samuelson, M.A. (Brigham and Women's Hospital); D. Shera, M.S., M. Weissman, Ph.D. (Columbia University); K. White, M.D. (St. Elizabeth's Hospital, Brighton, Mass.).