Pregnancy rates continue to climb in adolescents, with a 9% increase for teenage girls 15 to 19 years old and a 13% increase for teenage girls 13 and 14 years old from 1980 to 1990
(1). The social, academic, and economic impact of adolescent pregnancy has been amply documented
(2,
3). Pregnant teenagers are likely to have future unintended pregnancies
(2), to have limited educational achievement
(4,
5) to rely on public assistance
(6), and to receive lower wages for employment
(4). The children born to young teenage mothers have a higher risk of health problems, low academic achievement, and behavioral problems
(4,
5).
Causal factors related to adolescent pregnancy span political, social, and individual domains. Limited access to contraception, abortion, and sex education
(7), poverty
(8), demise of the traditional family
(9), drug use
(9), and normative community behavior
(5) have been associated with teenage pregnancy. Some individual factors for adolescent pregnancy include level of ego development
(10), self-esteem
(11), establishing a sense of identity
(12), and bringing meaning to life
(13).
The role of cognitive processes related to adolescent decisions about pregnancy is another area of investigation. Gordon
(14) suggested that adolescents who become pregnant have difficulty envisioning and assessing alternatives and have problems with perspective taking. Another cognitive model deals with attributions of causality and perceptions of controllability
(15). This theory posits that when an event occurs, an individual assesses it along three dimensions: internal-external, global-specific, and stable-unstable. Internal refers to a “self” attribution, and external refers to an “other” attribution. Global refers to factors that occur over a wide range of situations, and specific refers to factors that occur in a limited range of situations. Stable refers to factors that are long-lived or recurrent, and unstable refers to short-lived and nonrecurring factors
(15). Therefore, individuals with a negative attributional style attribute adverse-uncontrollable events to internal, global, and stable characteristics. That is, a bad outcome results because of character deficits (internal) that will be manifested in a wide range of settings (global) and that either will persist or may reoccur (stable). This leads to depression and feelings of helplessness and hopelessness
(16,
17). Although attributional style has been examined in pregnant adults
(18,
19), this cognitive model has not been investigated in pregnant teenagers.
The purpose of study 1 was to investigate attributional style and depressive symptoms in pregnant teenagers. It was hypothesized that pregnancy would serve as a stressful life event that would be associated with depression for teenagers with a negative (pessimistic) attributional style but not for those with a positive (optimistic) attributional style.
STUDY 1
Method
Subjects. A total of 218 subjects were obtained from the Adolescent Obstetrics Clinic and Family Planning Clinic at the University of Texas Medical Branch at Galveston. These clinics provide care to pregnant adolescents 18 years of age or younger who reside in Galveston and the surrounding counties. Most patients are from Caucasian, Mexican American, or African American backgrounds and have a family income at or below the poverty level.
Eligible potential subjects were approached in the waiting room by a research associate and were asked to complete questionnaires about their background, mood, and perception of events. Since these adolescent patients did not require parental consent for obstetrical or gynecological treatment, verbal assent (as approved by our institutional review board) was obtained from them.
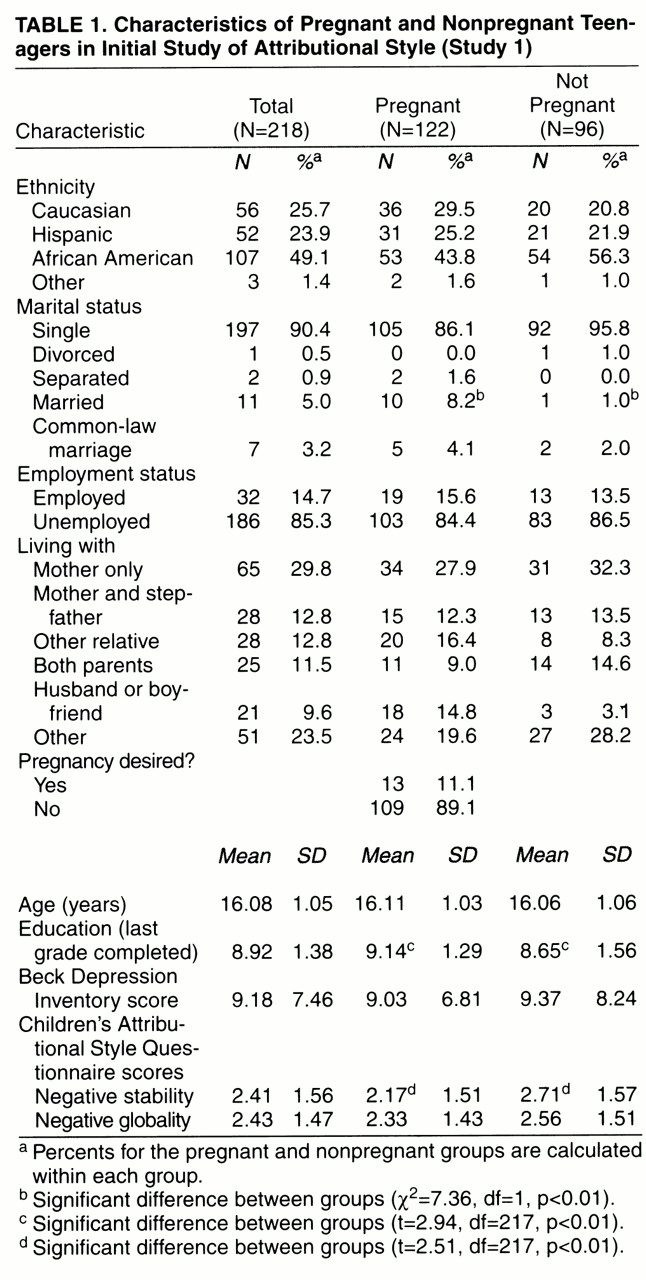
The subjects’ ages ranged from 13 to 18 years (mean=16.08). The majority of subjects were African American (49.1%), followed by Caucasian (25.7%) and Hispanic (23.9%). Most subjects (90.4%) were single. The average educational level achieved was eighth grade, and the majority of subjects (85.3%) were unemployed.
Of the total subjects, 122 were pregnant and receiving prenatal care at the adolescent obstetrics clinic. Ninety-six subjects were not pregnant. There were no significant differences between the pregnant and nonpregnant teenagers in age, ethnicity, employment status, or living arrangements. Although the majority of teenagers in both the pregnant group (86.1%) and the nonpregnant group (95.8%) were single, there were significantly more married teenagers in the pregnant group (8.2% versus 1.0%). The educational level achieved by the pregnant group (9.14 years) was slightly higher than that for the nonpregnant group (8.65 years). The majority of pregnant teenagers (89.1%) did not desire the pregnancy (
table 1).
Procedure. After verbal assent was obtained, patients were instructed to simply report their feelings and were told that there were no right or wrong answers. The questionnaires took, on the average, 15 minutes to complete. On completion, participants were given a small bottle of nail polish or hand lotion.
Attributional style was assessed with the Children’s Attributional Style Questionnaire
(17), a 48-item forced-choice measure of causal explanations for 24 positive and 24 negative events. Hypothetical events are presented, and children are requested to select the response that explains why the event happened to them. Consistent with the hopelessness theory and empirical work
(20), the stability and globality dimensions for negative outcomes were used. Robinson et al.
(21) provided reliability and validity data. Scores on each dimension range from 1 to 7; high scores reflect a tendency to attribute negative events to more stable and global factors. Depression level was assessed by the Beck Depression Inventory
(22,
23), a 21-item self-report inventory of depressed symptoms. The Beck inventory has yielded adequate reliability estimates, with a mean coefficient alpha of 0.81 for nonpsychiatric subjects
(24). The Beck inventory also has been well validated as a measure of severity of depressive symptoms
(24).
Results
The scores for the pregnant and nonpregnant groups on the Beck inventory and the negative stability and negative globality factors of the Children’s Attributional Style Questionnaire are reported in
table 1.
Consistent with the recommendations of Cohen and Cohen
(25), a setwise hierarchical multiple regression procedure was used to test predictions pertaining to the Children’s Attributional Style Questionnaire-by-pregnancy status interaction. Beck inventory scores served as the dependent variable. Children’s Attributional Style Questionnaire stability and globality scores, along with the pregnancy status variable (1=not pregnant, 2=pregnant), were entered into the regression equation simultaneously as a set. At step 2, the set of two-way interactions was entered into the equation, followed at step 3 by entry of the Children’s Attributional Style Questionnaire stability-by-globality-by-pregnancy status three-way interaction term. Regression analysis indicated that the attributional style questionnaire stability-by-globality-by-pregnancy status three-way interaction was, indeed, a significant predictor of Beck inventory depression scores (partial correlation [r]=0.15, t=2.13, df=210, p<0.05).
However, a significant interaction can indicate several different scenarios. To examine whether the form of the three-way interaction conformed to our hypothesis, following Cohen and Cohen
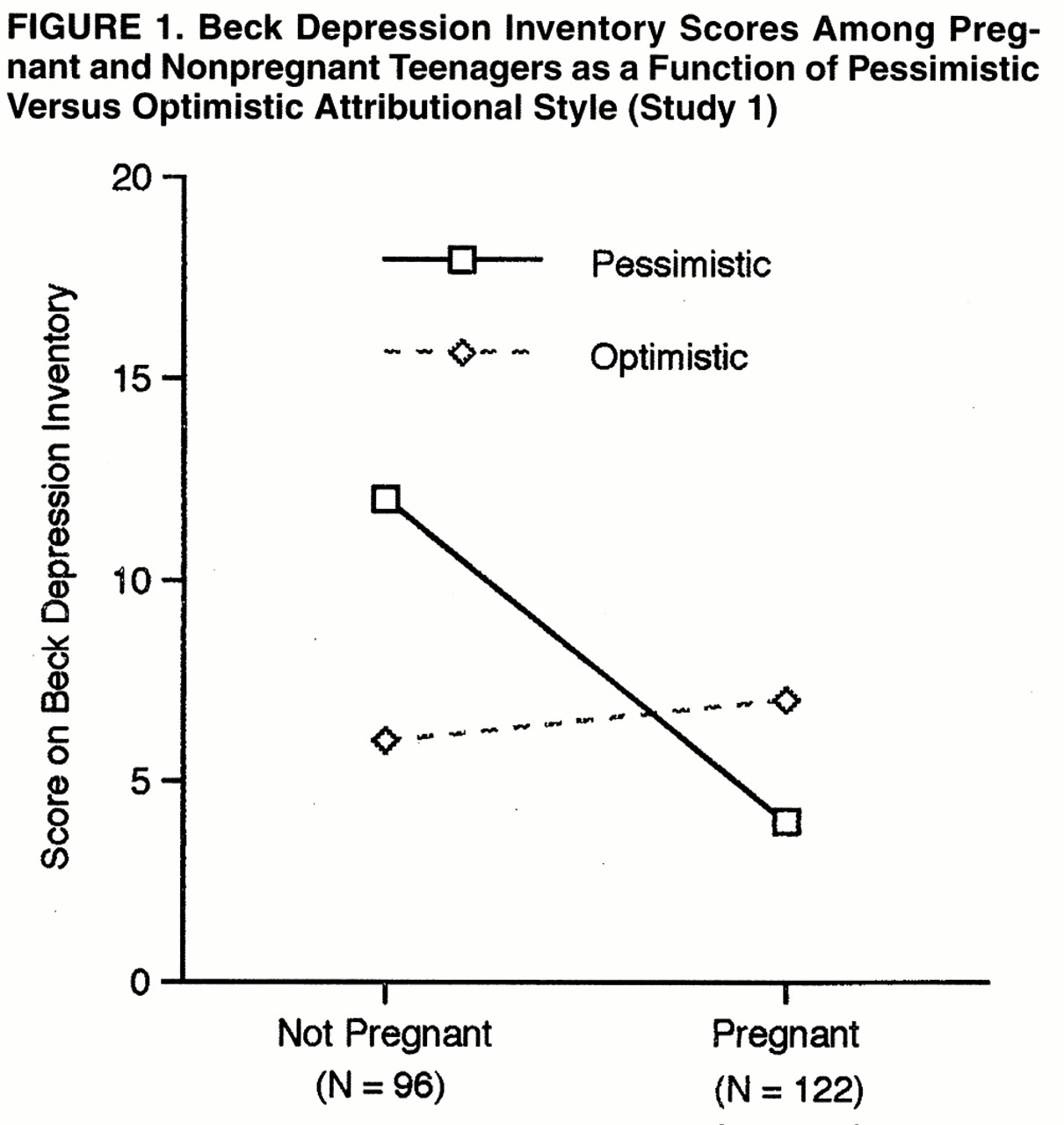
(25), Beck inventory scores were computed by inserting specific values for Children’s Attributional Style Questionnaire stability and globality factors (i.e., 1.5 standard deviations above and below the mean; results were similar when 1 standard deviation above and below the mean was used) and for pregnancy status (1=not pregnant, 2=pregnant) into the regression equation
(26,
27). The results of this analysis are depicted in
figure 1. As can be seen in
figure 1 and contrary to prediction, subjects who both possessed a negative attributional style and were pregnant were less, not more, depressed.
Discussion
Although it was expected that pregnancy would be a stressful life event that would be associated with depression in teenagers with a negative attributional style, this hypothesis was not supported by the data. In fact, pregnant teenagers who had a pessimistic attributional style were less depressed than pregnant teenagers with an optimistic attributional style, as well as the nonpregnant group. Because these findings, while interesting, were not predicted, a second study was conducted to replicate the findings of study 1.
STUDY 3
Method
Subjects. In this follow-up study, the 165 pregnant teenagers from studies 1 and 2 were contacted by mail to complete questionnaires. Sixty-three subjects (38%) completed and returned the questionnaires. The subjects ranged in age from 13 to 18 years (mean age=16.1). The majority of subjects were African American (46.0%), followed by Caucasian (26.9%) and Hispanic (22.2%). Most subjects (95.2%) were single.
Procedure. Questionnaires were mailed to subjects’ homes. Subjects were reminded about their previous participation in the study and were asked to complete the same questionnaires. Subjects were reimbursed $5.00 for completion of the questionnaire. The same set of measures as in studies 1 and 2, i.e., the Children’s Attributional Style Questionnaire and the Beck Depression Inventory, were used.
Results
The scores for the group were as follows: Beck inventory, mean=9.86, SD=8.67; Children’s Attributional Style Questionnaire negative stability factor, mean=2.28, SD=1.56; and the attributional questionnaire negative globality factor, mean=2.03, SD=1.22. Similar to our regression approach in studies 1 and 2, we examined the interaction between Children’s Attributional Style Questionnaire stability and globality as a predictor of Beck inventory scores. A very interesting pattern of results emerged.
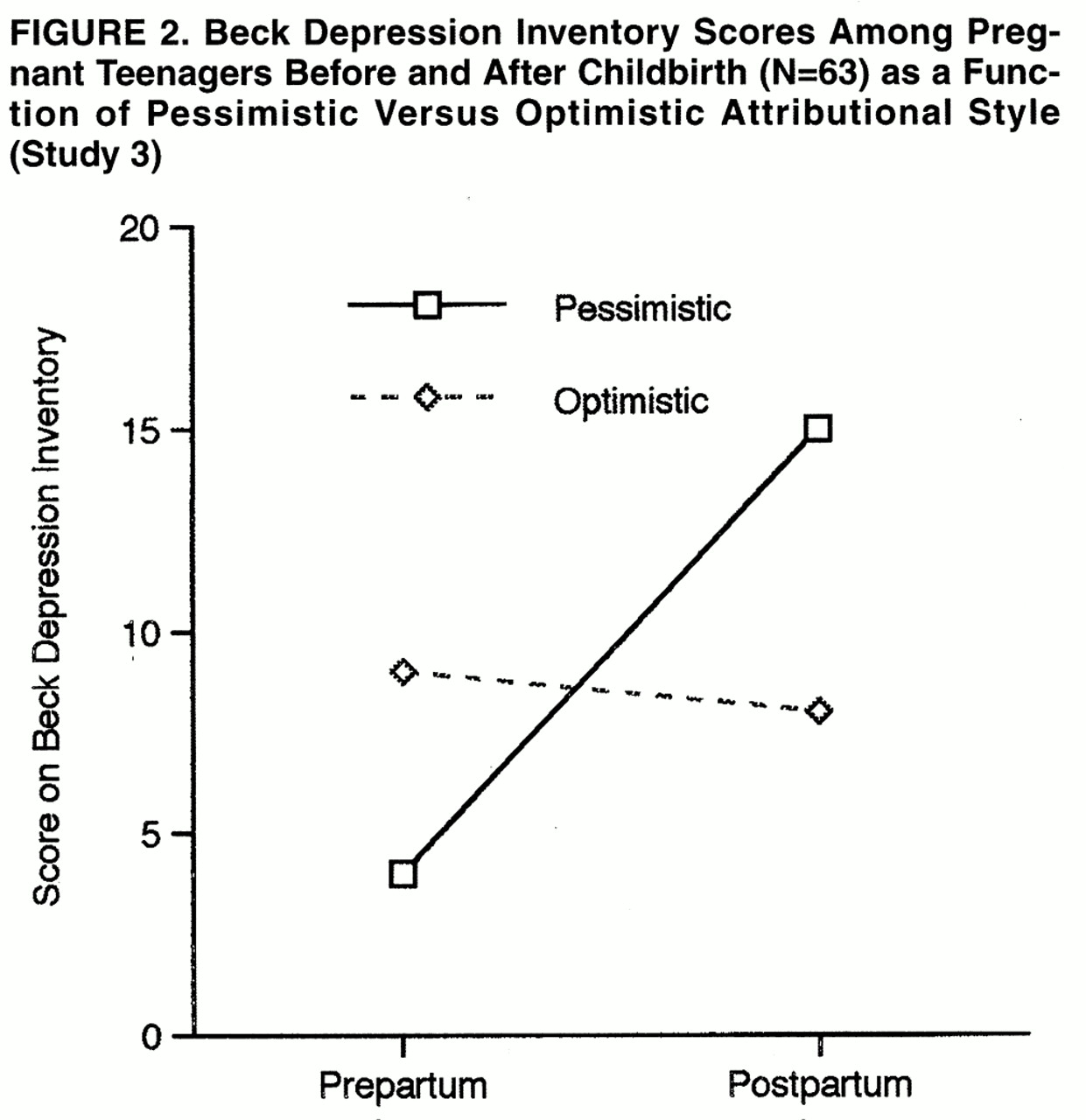
Among this subset of pregnant girls, there was no significant relationship between prepartum Beck inventory scores and the prepartum Children’s Attributional Style Questionnaire stability-by-globality interaction (partial correlation [r]=0.11, t=0.83, df=59). That is, pessimistic girls were no more likely to be depressed than optimistic girls while pregnant (similar to studies 1 and 2, in which the pessimistic pregnant girls were actually less likely to be depressed than the optimistic pregnant girls). However, there were differences after childbirth. The postpartum attributional style questionnaire stability-by-globality interaction served as a significant predictor of postpartum Beck inventory scores (partial correlation [r]=0.30, t=2.45, df=59, p<0.05). The form of this interaction (examined as described in study 1) was such that new teenage mothers with a more stable and more global attributional style for negative events were more depressed than new teenage mothers with an optimistic attributional style.
Discussion
Taken together, the results suggest an intriguing conclusion that higher levels of depression following childbirth were associated with a pessimistic attributional style (
figure 2). By contrast, while the subjects were pregnant, depression scores were not related to pessimism and may even have been negatively associated with pessimism (studies 1 and 2).
DISCUSSION
The results of these studies have important clinical implications with regard to teenage pregnancy. It was expected that pregnancy would serve as a stressful life event that would be associated with depression for teenagers with a pessimistic attributional style. In fact, the findings of these studies were contrary to this expectation. Pregnant teenagers with a pessimistic attributional style were less depressed than nonpessimistic teenagers. However, following childbirth the pessimistic teenagers did experience a higher level of depression than the nonpessimistic girls. These findings support the notion that pregnancy serves to protect pessimistic teenagers from depression. This relief, however, is short-lived, since pregnancy is a temporary event. It is important for the clinician to be aware that these pessimistic teenagers may develop depression after childbirth.
The results of this study of teenagers contrast with findings regarding pregnant adult women. Manly et al.
(18) found no relationship between attributional style during pregnancy and level of depression following childbirth. Although Cutrona
(19) showed a relationship between attributional style during pregnancy and depression following childbirth, attributional style accounted for only a small percentage of the variance in depression score.
To clarify the findings of this study, further research is necessary to understand the meaning of being pregnant, especially to pessimistic teenage girls. Pregnant girls who are emotionally deprived have described feeling important, special, and proud when pregnant
(12). The significance of these positive feelings may be more pronounced for pessimistic teenage girls and may protect them from the experience of depression. Comparing the relative importance of these factors in pregnant adolescents with pessimistic and optimistic attributional styles would shed light on this issue.
Similarly, the perceived demands of motherhood require further investigation, especially for the pessimistic teenagers. Teenagers, given their own developmental level, have significant emotional and social needs. Following childbirth, the adolescent is faced with complicated issues of child rearing, as well as potential problems with finances, completion of education, and the relationship, if any, with the baby’s father. These demands may overwhelm the pessimistic teenager, remove any positive feelings that had been associated with the pregnancy, and contribute to the development of depression.
Pregnant teenagers with a pessimistic attributional style may require therapeutic intervention. Although these teenagers may not appear depressed during the pregnancy, as demonstrated in our studies, depression may develop after childbirth. These adolescents may need preparation to deal effectively with the demands of an infant without becoming emotionally overwhelmed. Positive child rearing attitudes, as well as social support, have been shown to reduce stress for adolescent mothers
(28) and should be components of an intervention program.
Recent attention has focused on psychopathology related to teenage pregnancy. Wiemann and associates
(29) found low rates of psychopathology in pregnant teenagers. Kovacs and associates
(30) reported that conduct disorder, rather than depressive disorders, predicted teenage pregnancies. Steer and associates
(31,
32) found no differences in depression between pregnant and nonpregnant adolescents. Our studies demonstrate the importance of attributional style in its relationship to depression and teenage pregnancy.
The finding of this study, that pregnancy may reduce pessimism for teenagers, adds to the literature on adolescent risk behaviors. As discussed by Jessor
(33), risk behaviors such as smoking, drinking, substance abuse, and reckless driving are purposeful, functional, and goal directed and are not irrational. Jessor suggested that these behaviors foster adolescent development by reducing stress and anxiety, increasing independence, and establishing an identity in one’s peer group. Sensation seeking
(34) and unconventionality
(35) have been linked to unprotected sexual intercourse for adolescent girls. Jessor
(33) has commented that these risk behaviors for adolescents will continue unless healthy alternative behaviors are promoted that would serve these same goals.
Repeated adolescent pregnancies are common, with prevalence rates of 30% and 40% to 50% during the first and second postpartum years, respectively
(36). This is a major issue of concern, since intervention programs have not demonstrated efficacy in reducing the rates of repeated pregnancies
(37). Therefore, risk factors for repeated pregnancies have become a critical issue
(38,
40). Our studies suggest that pregnancy protects a pessimistic teenager from depression and that these pessimistic teenagers are more prone to experience depression after childbirth. This may be a previously unidentified risk factor for repeated pregnancies in teenagers. It may be the case that the experience of depression following childbirth is relieved by another pregnancy. This parallels the literature, which reports mood stabilization
(41,
42) and low risk of suicide
(43) during pregnancy.
There are a number of limitations to our study that may affect the conclusions. Depression was assessed with a self-report measure, and it is possible that different levels of depression might have been found with a clinician-administered instrument. The follow-up response rate was modest, which may have biased the results. No information was obtained about the teenagers’ expectations of child rearing; this may have confounded the results if the pessimistic teenagers had anticipated that child rearing would be a positive experience. Despite these limitations, the potential clinical significance of these findings argues for examination of clinician-assessed depression, attributional style, and childbearing expectations and realities in teenagers before and after childbirth.