Peritraumatic dissociation has been studied in war veterans
(1,
2), disaster survivors
(3) and emergency workers
(4). Those with greater peritraumatic dissociation appear to be at greater risk for chronic posttraumatic stress disorder (PTSD) and posttraumatic symptoms. Importantly, peritraumatic dissociation predicts risk of PTSD independent of the level of trauma exposure and general dissociative tendencies
(2). Despite the number of studies of peritraumatic dissociation, most studies have been limited by retrospective design and lack of standardized clinician ratings of peritraumatic dissociation and PTSD.
Motor vehicle accidents are an important cause of PTSD
(5,
6); however, the relation between peritraumatic dissociation and motor vehicle accident-related PTSD has been infrequently examined
(7). In addition, prior PTSD is a risk factor for PTSD following motor vehicle accidents
(6), increasing the risk of PTSD by 6.81 to 8.02 times
(5). It is not known whether the risk associated with peritraumatic dissociation is independent of that due to prior PTSD and thus reflects different underlying psychological and biological mechanisms.
Earlier, in a prospective longitudinal study
(5), we reported increased rates of PTSD following serious motor vehicle accidents. In order to better understand the relation between peritraumatic dissociation and PTSD, we have now examined peritraumatic dissociation in that same group of subjects by using standardized clinician ratings of peritraumatic dissociation. To determine whether the risk of peritraumatic dissociation is independent of prior PTSD, we also examined the relation of peritraumatic dissociation to PTSD after adjusting for the presence of PTSD before the motor vehicle accidents.
METHOD
We recruited 122 subjects who had been in motor vehicle accidents, 72% from the regional trauma center of a major suburban hospital and 28% from police reports. Demographic and dependent variables did not differ between subjects from the two recruitment sources. A full description of the study method has been previously published
(5). Of the participants, 64 (52.5%) were male and 58 (47.5%) female. Most were white (N=93, 76.2%), were not married (N=76, 62.3%), had at least some college education (N=89, 73.0%), and had an annual income above $20,000 (N=69, 56.6%). The mean age at the time of the accidents was 35.6 years (SD=13.1).
The subjects were drivers or passengers, between the ages of 18 and 65 years, who had been in serious motor vehicle accidents involving another vehicle. They resided within 40 miles of the recruitment hospital. Persons who agreed to participate gave written informed consent. Two physicians systematically reviewed hospital records and excluded individuals with evidence of head trauma, coma, or organic brain syndrome identified by positive results on a neurological examination, a mental status examination, or a computed tomography scan.
One month after the motor vehicle accident we administered the Structured Clinical Interview for DSM-III-R (SCID) with the PTSD supplement
(8) to assess lifetime and current PTSD and the Peritraumatic Dissociative Experiences Questionnaire—Rater Version
(2). We obtained two Peritraumatic Dissociative Experiences Questionnaire scores: presence of any peritraumatic dissociative symptom (at least one of eight symptoms scored “threshold”) and total number of symptoms endorsed. Interviews were conducted at the subject’s home by senior licensed clinical social workers experienced with the SCID. Analyses showed excellent overall agreement between raters
(5).
Significance was set at p=0.05 for all analyses. Risks of acute and chronic motor vehicle accident-related PTSD were evaluated by univariate logistic regression and chi-square analyses. Odds ratios with 95% confidence intervals (CI) and Wald chi-square test results are reported. Multivariate logistic regression and goodness-of-fit chi-square tests were used to examine the relation of peritraumatic dissociation to PTSD, adjusting for race and prior PTSD.
RESULTS
Of the 122 subjects, 96 (78.7%) reported at least one peritraumatic dissociative symptom (mean=2.10, SD=1.83, range=0–8). The most common peritraumatic symptom was a change in the sense of time (time speeding up or slowing down) during the event (N=69, 56.6%). White subjects were 3.98 times more likely than nonwhite subjects to report peritraumatic dissociative symptoms (Wald χ2=8.44, df=1, p=0.004, 95% CI=1.56–10.12), and unmarried subjects were 2.86 times more likely than married subjects to report such symptoms (Wald χ2=5.38, df=1, p=0.02, 95% CI=1.18–6.94). Neither race nor marital status was related to total symptoms. Younger subjects reported more peritraumatic dissociative symptoms (r=–0.22, df=120, p=0.01). Peritraumatic dissociation was not associated with gender, education, or income.
At 1 month 42 (34.4%) of the 122 subjects, and at 3 months 25 (25.3%) of 99 subjects, had a diagnosis of PTSD. Thirteen subjects (10.7%) had a lifetime diagnosis of PTSD before the motor vehicle accident. Because both peritraumatic dissociation and PTSD were associated with race
(5), we used a multivariate logistic regression adjusting for race to examine this relationship. Subjects who reported peritraumatic dissociation were 4.12 times more likely to develop acute PTSD (Wald χ
2=5.33, df=1, p=0.02, 95% CI=1.24–13.67). Total number of symptoms did not significantly affect the risk of acute PTSD. Subjects who reported peritraumatic dissociation were 4.86 times more likely to develop chronic PTSD (Wald χ
2=3.86, df=1, p=0.05, 95% CI=1.00–23.50). Those with a greater number of peritraumatic dissociative symptoms were also at increased risk for chronic PTSD (Wald χ
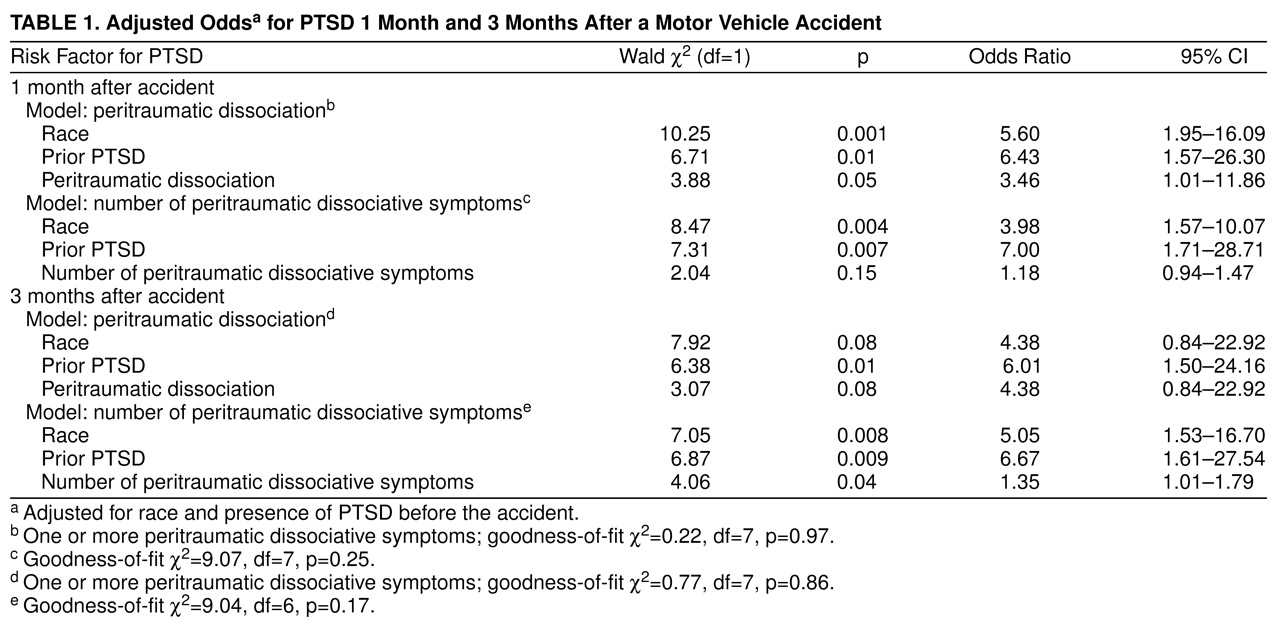
2=4.60, df=1, p=0.03, odds ratio=1.35, 95% CI=1.03–1.77). Even after we adjusted for prior PTSD, those with peritraumatic dissociation were 3.46 times more likely to develop acute PTSD, but not more likely to develop chronic PTSD (
table 1). In contrast, the total number of peritraumatic symptoms did not increase the risk of acute PTSD but significantly increased the risk of chronic PTSD. Prior PTSD remained a significant risk factor for acute and chronic PTSD.
DISCUSSION
To our knowledge, this is the only longitudinal, prospective study of PTSD and peritraumatic dissociation that has controlled for the type of traumatic event and used standardized clinician ratings. Our results indicate that clinician-assessed peritraumatic dissociative symptoms are common (79%). This percentage is similar to, but somewhat greater than, the 51% in the study by Shalev et al. of injured trauma victims
(9), in which a self-report measure of peritraumatic dissociation was used. This difference suggests that people may underreport symptoms, or it may reflect the effect of different traumatic events. Our subjects with peritraumatic dissociation were 4.12 times more likely to experience acute PTSD and 4.86 times more likely to develop chronic PTSD. The risk of chronic PTSD is similar to that in previous studies of combat veterans and disaster workers
(2,
4) and underscores the clinical importance of assessing peritraumatic dissociation after motor vehicle accidents.
Importantly, after adjusting for prior PTSD, peritraumatic dissociation remained a significant risk factor for acute PTSD (odds ratio=3.46) and chronic PTSD (odds ratio=4.38). Therefore, prior PTSD and peritraumatic dissociation appear to be independent risk factors.
Our finding that the most common peritraumatic symptom was a sense of time change during the event agrees with findings in previous studies
(9,
10). Laboratory studies have linked the basal ganglia
(11) and cerebellum
(12) to a brain timing system. Both decreased cerebellar blood flow and increased left cerebellar blood flow
(13) have been associated with an altered sense of time. These brain regulators may therefore be important to peritraumatic dissociation. Although our study group was more substantial than those in some previous studies, replication with a larger study group is needed. In addition, assessments of peritraumatic dissociation should be done as close to the motor vehicle accident as possible. Neuroimaging studies of stress and altered sense of time will advance our understanding of the neurobiological regulators underlying peritraumatic dissociation and PTSD. Future studies should also examine predictors of peritraumatic dissociation and the interaction of peritraumatic dissociation with other risk factors for PTSD.