Weight gain frequently occurs during treatment with clozapine
(1) or olanzapine
(2) and sometimes limits treatment compliance. Clozapine has been shown to increase circulating levels of leptin
(3), a hormone produced by fat cells that is thought to signal the size of the adipose tissue to the brain. Mice and humans deficient in leptin are obese
(4,
5). In
ob/ob mice, leptin administration reduces food intake and weight
(6,
7), indicating a role for this hormone in weight regulation. In humans, circulating leptin level correlates positively with body mass index; patients with anorexia nervosa, for example, have low leptin levels that increase in parallel to weight during treatment
(8).
To explore the pathophysiology of weight gain during antipsychotic treatment, we longitudinally investigated weight, body mass index, and leptin level in patients treated with clozapine or olanzapine. In addition, we included a group of patients treated with haloperidol, which is known to induce only minor changes in weight
(2). To control for the effect of minor dietary changes upon hospitalization, we also investigated patients who did not receive any pharmacological treatment.
METHOD
Consecutively admitted inpatients fulfilling the DSM-IV diagnostic criteria for a schizophrenic disorder were assigned according to clinical decisions to monotherapy with clozapine (N=11), olanzapine (N=8), or haloperidol (N=13). The clozapine group comprised seven women and four men, whose mean age was 37 years (SD=19). In the olanzapine group there were five women and three men, and their mean age was 26 years (SD=6). The haloperidol group contained seven women and six men, and their mean age was 36 (SD=16). The mean doses (in milligrams per day) during weeks 1, 2, 3, and 4, respectively, were as follows: clozapine—85 (SD=50), 145 (SD=63), 199 (SD=80), and 251 (SD=117); olanzapine—11 (SD=3), 13 (SD=3), 13 (SD=3), and 14 (SD=4); haloperidol—5 (SD=3), 5 (SD=3), 5 (SD=3), and 6 (SD=3). Twelve patients (seven women and five men; mean age=30, SD=12) suffering from various psychiatric disorders other than schizophrenia received no psychopharmacological treatment. The absence of medication was due either to diagnostic purposes (N=4) or to the fact that the patients were treated with behavioral psychotherapy exclusively (N=8). All patients received a standard hospital diet. After complete description of the study, all patients gave informed written consent to participate in the investigation, which had been approved by an independent ethics committee.
Weight was assessed at baseline and weekly thereafter. The body mass index was calculated by dividing the weight (in kilograms) by the squared height (in meters). The plasma levels of leptin were assessed by using radioimmunoassay (DRG Instruments, Marburg, Germany). The limit of detection was 0.5 ng/ml, and the intra- and interassay coefficients of variation were 7% and 9%, respectively. For statistical analysis, multivariate analysis of variance (MANOVA) for repeated measures was used. Post hoc comparisons were performed by tests with contrasts. As the nominal level of significance an alpha level below 0.05 was accepted and corrected according to Bonferroni for the post hoc tests. To account for baseline differences in weight, body mass index, and leptin level between groups, all values were divided by the mean at baseline for the respective treatment group before statistical analysis.
RESULTS
Analysis of variance revealed a significant overall treatment-by-time interaction (averaged Wilks"s multivariate test of significance: F=1.9, df=36, 476, p=0.001). Weight (F=4.4, df=12, 160, p<0.05), body mass index (F=4.6, df=12, 160, p<0.05), and leptin plasma level (F=2.3, df=12, 160, p<0.05) all contributed significantly to this interaction term.
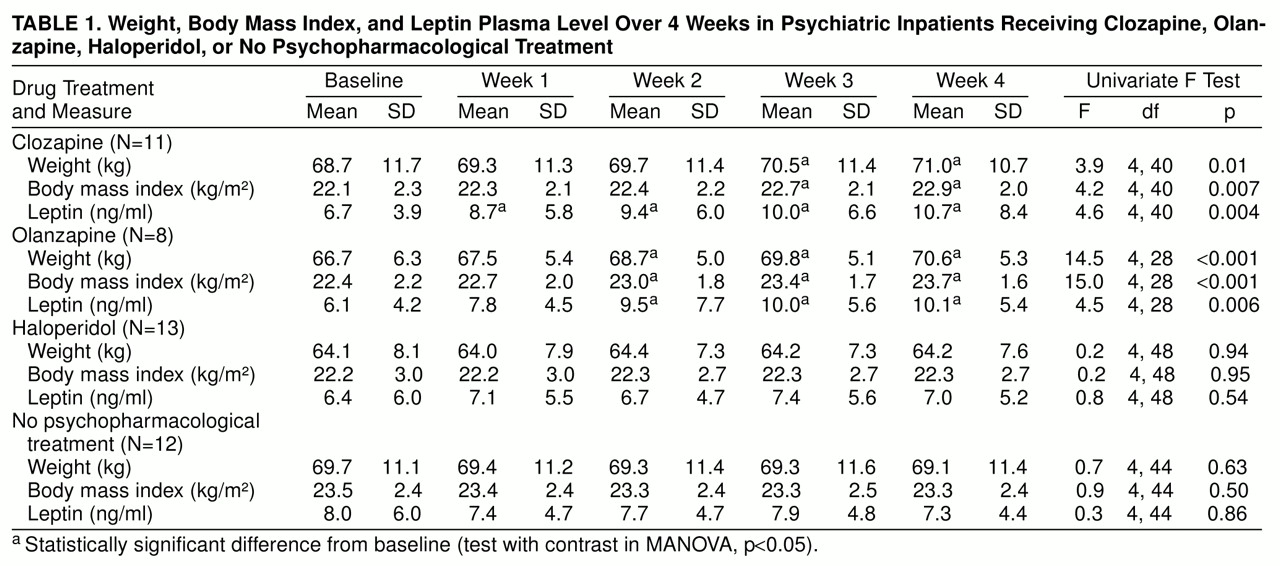
As can be seen from
table 1, clozapine and olanzapine treatment significantly increased weight, body mass index, and plasma leptin level. In the clozapine-treated group, leptin plasma level was significantly increased from baseline already at the end of the first treatment week; effects on body mass index and weight were evident from the third week onward. In the patients treated with olanzapine, plasma leptin level, weight, and body mass index were significantly increased from baseline starting at the end of the second week of treatment. MANOVA did not reveal a significant difference between the clozapine- and olanzapine-treated patients in the time course of any of the variables assessed.
In the drug-free patients and those treated with haloperidol, weight, body mass index, and leptin level showed no significant changes across time. MANOVA did not reveal a significant difference between these two groups in the time course of any of the variables assessed.
DISCUSSION
The present study confirms that clozapine-induced weight gain is associated with an increase in circulating leptin level
(3). Moreover, we showed that olanzapine has similar effects, whereas weight, body mass index, and leptin level remain stable in patients receiving haloperidol or no psychopharmacological treatment. Therefore, the increases in weight and leptin level induced by clozapine and olanzapine cannot be explained by dietary changes upon hospitalization.
It has been shown that 75% of patients treated with clozapine report an increased desire to eat, and some patients report binge eating
(3), suggesting that overeating leads to weight gain. Although we did not gather the respective information in the present study, it is likely that overeating underlies olanzapine-induced weight gain as well. Hence, the most probable reason for clozapine- and olanzapine-induced increases in leptin levels are overeating and weight gain. These may be due to the drugs’ effects on various neurotransmitter systems involved in the regulation of appetite
(1–
3). Alternatively, clozapine and olanzapine might reduce the feedback sensitivity of the CNS to the leptin signal, thus leading to a cascade of increased appetite, leptin secretion, and weight gain.
Apart from its involvement in the regulation of appetite, leptin has CNS effects such as blunting of stress responses
(9). Because weight gain has some predictive value for a positive response to clozapine treatment
(1,
10), it seems worthwhile to investigate leptin levels and psychopathology in parallel to test the hypothesis that leptin mediates the beneficial effects of neuroleptic treatment.