Therapeutic Drug Monitoring
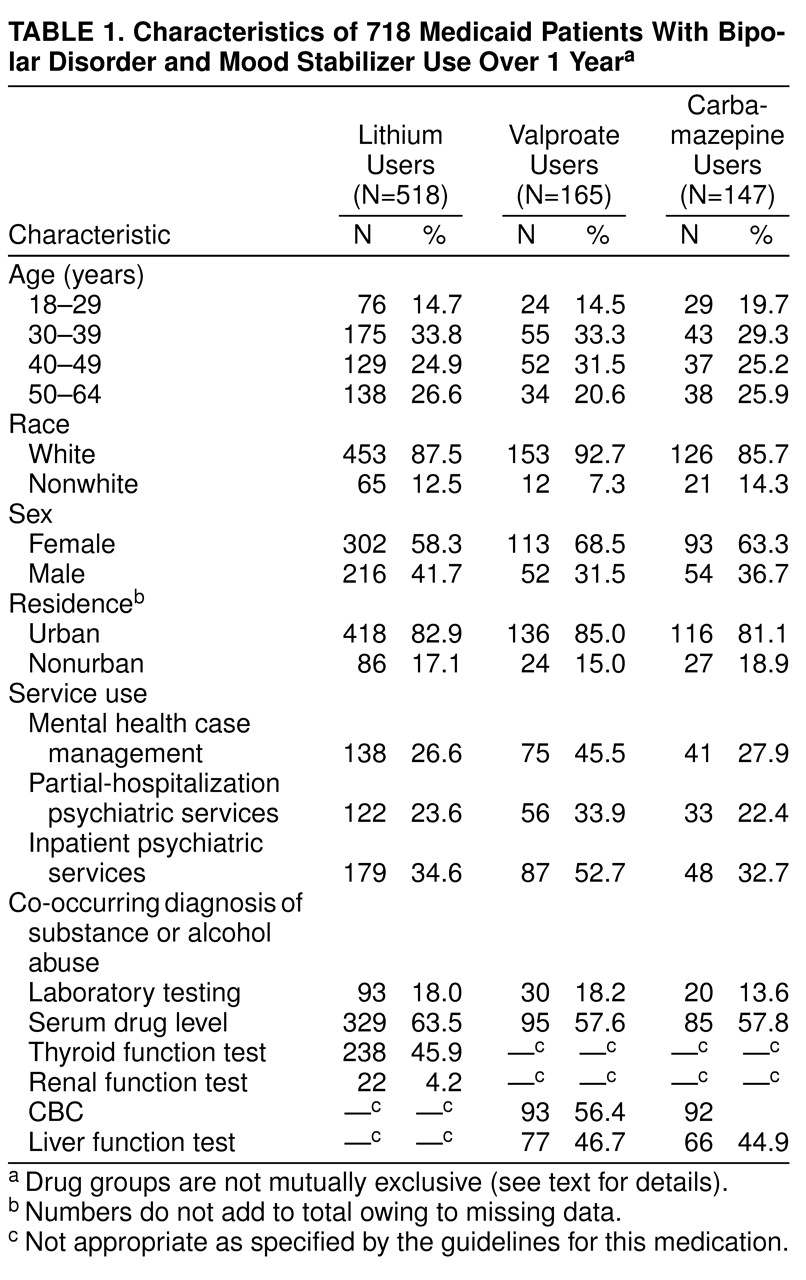
Approximately two-thirds of the lithium users received a blood test to determine the lithium blood level during the 12-month study period (
Table 1). Slightly smaller percentages of the valproate and carbamazepine users received serum drug level testing during this period. The patients who received prescriptions during four calendar quarters did not have significantly higher rates of drug monitoring than those with three quarters of use.
The guidelines recommend that lithium users receive, at a minimum, yearly thyroid and renal function tests. Slightly fewer than one-half were tested for thyroid function, and few were tested for renal function during that time (
Table 1). Somewhat more than one-half of the valproate and carbamazepine users received CBCs, and slightly fewer than one-half received liver function tests. Among the lithium users, those who received partial-hospitalization psychiatric services had a higher rate of serum drug level testing (73.8% versus 60.4%) (χ
2=7.2, df=1, p<0.001). Mental health case management for valproate users was associated with a lower rate of serum drug level testing (49.3% versus 64.4%) (χ
2=3.8, df=1, p=0.05). Age, race, sex, urban/nonurban residence, co-occurring diagnosis, and other service use were not significantly associated with receiving serum drug level testing for any of the three mood stabilizers (data not shown).
Lithium users were more likely to receive the recommended serum level test if they also received partial hospitalization. Somewhat surprisingly, valproate users who received mental health case management services were less likely to receive serum level testing than those who did not receive case management. There were no statistically significant factors for carbamazepine testing.
After the demographic and service use variables were controlled for, logistic models revealed that lithium users who received partial hospitalization were approximately twice as likely to receive a lithium serum level test as were other lithium users (odds ratio=1.9, Wald χ2=7.0, df=1, p=0.008). Women were 1.5 times more likely (Wald χ2=4.6, df=1, p=0.03). Carbamazepine users who were 30 to 39 years old were 7.4 times less likely (Wald χ2=9.8, df=1, p=0.002) to receive a serum level test than the 18–29-year-old group. Those 40 to 49 years old were 6.3 times less likely to receive such tests (Wald χ2=8.3, df=1, p=0.004). Women were 3.3 times more likely (Wald χ2=7.9, df=1, p=0.005) to receive the test than were men. Valproate users who were 30 to 39 years old were 3.3 times less likely (Wald χ2=4.0, df=1, p=0.04) to receive a serum level test than the 18–29-year-old group. Those 40–49 years old were 3.4 times less likely to receive such tests (Wald χ2=4.1, df=1, p=0.04). In addition, valproate users were 2.6 times less likely to be tested if they used mental health case management (Wald χ2=6.4, df=1, p=0.01) and 2.4 times more likely if they were users of partial hospitalization (Wald χ2=5.1, df=1, p=0.02).
Correlations between the recommended laboratory tests were generally high. A lithium user who received a serum level test was also likely to receive a thyroid function test (ϕ=0.62, χ2=198.0, df=1, p=0.001) but not necessarily a renal function test (ϕ=0.14, χ2=10.1, df=1, p=0.001). Valproate users who were tested for serum drug level were likely to receive a CBC (ϕ=0.65, χ2=46.8, df=1, p=0.001) and a liver function test (ϕ=0.53, χ2=5.1, df=1, p<0.0001). Likewise, carbamazepine users who were tested for serum level usually received a CBC (ϕ=0.85, χ2=105.8, df=1, p=0.001) and a liver function test (ϕ=0.60, χ2=53.8, df=1, p=0.001).